Post Anti SARS-CoV2 Vaccination Guillain Barre Syndrome: A Case Report and Literature Review
Received Date: November 28, 2021 Accepted Date: December 28, 2021 Published Date: December 30, 2021
doi: 10.17303/jnnd.2021.9.203
Citation: Giorgia Sivori (2021) Post Anti SARS-CoV2 Vaccination Guillain Barre Syndrome: A Case Report and Literature Review. J Neurophysiol Neurol Disord 9: 1-19
Abstract
Guillain–Barrè syndrome is a rare but potentially serious disease. The exact cause of Guillain–Barrè syndrome (GBS) is still unknown. Campylobacter jejuni infection is the most commonly identified precipitant of GBS. Cytomegalovirus, influenza virus, human immunodeficiency virus (HIV), and Zika virus have also been associated with GBS. A small percentage of patients develop GBS after another triggering event such as surgery, trauma, bone-marrow transplantation or immunization. The relationship between Guillain–Barrè syndrome and vaccinations like after a meningococcal vaccine, influenza vaccine, and others vaccine, is well known.
In the recent pandemic context, the start of the vaccination campaign has led to the observation of related manifestations: in this case report, we are presenting a case of vaccine-associated Guillain–Barrè syndrome due to SARS-CoV2 vaccine (AstraZeneca) in a women, who presented with lower limb weakness and gait ataxia.
Keywords: Guillain Barrè; GBS; Covid Vaccines
Introduction
Overview of Plasmonic Biosensors
Guillain–Barrè syndrome is a rare but potentially serious disease: is fatal in about 3 percent of patients, even with treatment [1]; up to 25 percent of patients require intubation and mechanical ventilation. The prognosis is worse in older patients, those with severe symptoms, and those with rapid onset of symptoms. Up to 20 percent of patients have residual disability, which in half of the cases is severe [1,2].
The exact cause of Guillain–Barrè syndrome is still unknown. Campylobacter jejuni infection is the most commonly identified precipitant of GBS [3,4]. Cytomegalovirus [5,6], influenza virus [7,8] human immunodeficiency virus (HIV) [9], and Zika virus [10,11] have also been associated with GBS.
A small percentage of patients develop GBS after another triggering event such as surgery, trauma, bone-marrow transplantation or immunization [12].
Also the relationship between Guillain–Barrè syndrome and vaccinations like after a meningococcal vaccine [13-15], influenza vaccine [16,17], and others vaccine, is known.
We are in a pandemic context: from the first case of severe acute respiratory syndrome coronavirus 2 was reported in Wuhan, China, in December 2019, rapidly the disease spread and became a global pandemic.In February 2020, the World Health Organization designated the disease COVID-19 (coronavirus disease 2019). The World Health Organization declared COVID-19 a pandemic on March 11, 2020.
Covid 19 predominantly causes respiratory illness with symptoms such as myalgia, sore throat, cough, fever, anosmia and diarrhea, but sometimes also moderate to severe symptoms of acute respiratory distress syndrome, with possible evolution towards multiorgan failure.
Multiple neurological complications have been associated with Covid 19 infection [18,19], especially in hospitalized patients: more than 80 percent of hospitalized patients have Covid-related neurological complications [20,21]. Among them, to date there are many cases and series already published asserting a causal link between SARS-CoV-2 and Guillain-Barrè Syndrome [22-24].
In the recent pandemic context, the start of the vaccination campaign has led to the observation of related manifestations: in this case report, we are presenting a case of vaccine-associated Guillain–Barrè syndrome due to SARS-CoV2 vaccine (AstraZeneca) in a women, who presented with lower limb weakness and gait ataxia.
Case Presentation
A 69-year-old women presented to the Emergency Department with a history of back, right leg and hands pain, progressive lower limbs weakness for five days with gait disorders and imbalance.
About 15 days prior to these symptoms, she received AstraZeneca COVID-19 vaccine.
Remaining past medical history was insignificant, and particularly in the past months she presented neither respiratory or gastrointestinal infections, nor dog bites or anything else.
On physical examination, the patient was afebrile and her vitals were:
a) Blood pressure: 190/96 mm Hg;
b) Respiratory rate: 18 breaths/minute;
c) Heart rate: 82 bpm.
Neurological examination revealed: no facial weakness and intact cranial nerves. The patient was alert, oriented in time, space and people, collaborating. Higher mental functions were in order. Motor system examination of the four limbs revealed following: normal strength except for weakness of the upper limbs at the level of the interossees and extensors of the fingers (Medical Research Council scale grading muscle strength, MRC, 4/5 bilaterally) and in the dorsiflexion of the foot (MRC 4/5 bilaterally). There were no disorders of the coordination. We observed also diffuse hyporeflexia (in particular complete absence of patellars, and extremely weak ankle reflexes bilaterally) and gait ataxia. The patient reported feelings of hypoesthesia in the left deltoid region, left hemiaddome and external face of the left thigh. MRC sum score: 58.
GBS Disability Scale: 2. (GBS disability scale: from Plasma Exchange/Sandoglobulin GBS Trial Group, 1997). Laboratory investigations revealed hemoglobin of 15 g/dl with the hema tocrit of 42,60%; PCR was 1,50 mg/dl. The other investigations carried out were: first, she performed an MRI scan of the spine with contrast agent that showed alteration of hyperintense signal in STIR with hypointense equivalent in both T1 and T2 and lively impregnation after gadolinium ev in the upper portion of the right hemisome of L4; depression of the right somatic hemilimitant, which was related to edema of the bone spongy probably from vertebral collapse, also in the absence of anamnestic traumas.
Was prescribed by orthopedists a semi-rigid torso. The spine MRI showed no clear contrast enhancement of the nerv roots. Then, a brain MRI with contrast agent (in the emergency room she had already performed a CT scan showing multinfartual encephalopathy) showed not areas of compatiblished diffusion with recent ischemic lesion, but multiple areoles of hypersignal in T2 and FLAIR in both subcortical and subcortical white matter deep at the bilateral fronto-parieto-insular level with confluent appearance at the periventricular level, probable parenchymal suffering on a chronic vascular basis.
A cardiological evaluation was performed and set antiplatelet therapy. Cerebrospinal fluid examination (CSF) was performed ten days after the onset of symptoms, revealed clear fluid, normal opening pressure, glucose 74 mg/dl (normal range: 45–100 mg/dl), proteins 0.43 g/l (normal range: 0.18–0.45 g/dl) and WBCs 1/cmm: not clear albuminocytologic dissociation. Immunoblot: not oligoclonal bands in serum and liquor.
The electrophysiological study performed on the seventh day from the onset of symptoms shows:
- motor alterations of the demyelinating type, increased of motor distal latency on left ulnar and median nerve and velocity reduction on median nerve;
- sensory alterations with a “sural sparing pattern” with amplitude reduction on left ulnar e median with normal amplitude on left sural nerve (early-stage pathognomonic finding of dysimmune neuropathy. It does not help discriminate between demyelinating and axonal subtypes).
- a prolonged F-wave in the left ulnar nerve and a prolonged distal latency of the right tibial nerve.
The neurophysiological findings were compatible with acute demyelinating sensory-motor polyneuropathy (AIDP) (Hadden criteria et al 1998) [38].
From “CRITERIA FOR ELECTROPHYSIOLOGICAL CLASSIFICATION “(38) PRIMARY DEMIELINATING (At least one of the following in each of at least two nerves, or at least two of the following in one nerve if all others are inexcitable and dCMAP≥ 10%LLN) MCV<90% LLN (85% if dCMAP<50% LLN) DML>110% ULN (120% if dCMAP<100% LLN) pCMAP/dCMAP ratio<0,5 and dCMAP ≥ 20% LLN F response latency >120%VLN
Serum antiganglioside antibody detection has been performed: no antibody detected.
With reference to NINDS criteria 1978 revised in 1990 (39-40) and subsequently modified in a review paper (41), we could make a diagnosis of Guillain Barrè syndrome.
The day after the electrophysiological study (on the eight day from the onset of symptoms), she underwent an immunoglobulin cycle (0.4 g/kg/day for 5 days) with improvement of the clinical conditions (plasmapheresis wasn’t performed in our hospital).
During the subsequent hospitalization there was a gradual progressive improvement. The patient began to walk under the supervision of the physioterapists, first with a walker and then with a single support. GBS disability scale: 1.
On the nineteenth day of hospitalization, after an electrophysiological check substantially unchanged compared to the previous one, she was transferred to the Intensive Rehabilitation Department of our hospital.
After an initial continuation of clinical recovery with clear benefit of physiotherapy, our patient presented on the 15th day after the transfer, weakness in the lower extremities widely.
(MRC4/5 bilaterally and widely). MRC sum score: 54/60. GBS disability scale: 3. It was interpreted as treatment related fluctuation (TRF) [36]. A new electrodiagnostic test was performed: it revealed a worsening compared to the previous control.
Often treatment-related fluctuation (TRF) required repeated IVIg treatment (about 10% of GBS patients have a secondary deterioration within the first 8 weeks after start of IVIg [30]). Despite uncertain benefit and and the evidence of recent literature [37], we too have decided to administer a second dose of immunoglobulins (0.4 g/kg/day for 5 days).
There was a subsequent gradual new recovery. To date, the patient is able to walk with stepping gait bilaterally but autonomously without support for at least ten meters. MRC sum score: 56/60. GBS disability scale: 2. An electrophysiological study performed three and a half months after the onset showed a slight neurophysiological improvement.
She never developed respiratory failure or autonomic dysfunctions.
Discussion
The so many global cases of the COVID-19 respiratory illness caused by the virus SARS-CoV-2 resulted in a global pandemic and medical and economical devastation worldwide.
To date there are many cases and series already published asserting a causal link between SARS-CoV-2 and Guillain-Barrè Syndrome [22-24].
The relationship between Guillain–Barrè syndrome and vaccinations like after a meningococcal vaccine [13-15], influenza vaccine [16,17], and others vaccine, is well known, also if the risk of GBS after vaccination appears substantially lower than the risk of GBS triggered by acute infection [24,25]. In addition, preventing acute illness through vaccination can reduce infection-triggered GBS.
In the recent pandemic context, a worldwide mass vaccination programme has been started since the end of 2020-beginning of 2021.
Vaccine-associated Guillain–Barrè syndrome is defined as those with the onset of Guillain–Barrè syndrome symptoms within a six-week period after receiving the vaccine, as reported by Vaccine Adverse Event Reporting System (VAERS) [26].
To date, based on available epidemiological data, a potential association between the adenovirus vector vaccines (AstraZeneca COVID-19 and especially Janssen/Johnson & Johnson COVID-19 vaccine) and Guillain-Barrè syndrome is being investigated [31-34]. Especially, although a causal link has not been yet unequivocally established, 100 cases of GBS have been observed in the United States occurring within six weeks of immunization, among 12.5 million patients given a dose of Janssen/Johnson & Johnson COVID-19 vaccine [43]. The estimated rate (7,8 cases per million doses) was approximately five times the background rate. Cases have also been reported after AstraZeneca vaccine, but with less significant numbers than the former.
Instead, a similar signal has not been observed with the mRNA COVID-19 vaccines.
On 22 July 2021 European Medicines Agency (EMA) announced that, with regard to the Janssen vaccine, Guillain-Barrè syndrome will be added to the Product Information as a side effect undesirable very rare, based on GBS cases examined until June 30, 2021 (108 cases out of more than 21 million administrations of this vaccine) (22 luglio 2021 EMA/408515/2021).
Even more recently EMA announced that the same syndrome will be added as very rare effect also of AstraZeneca COVID-19 vaccine: until July 31, 833 cases of the neurological syndrome have been reported worldwide, with over 592 million doses of the Anglo-Swedish serum administered.
We have reported another vaccine-associated Guillain–Barrè syndrome case due to Sars Cov 2 vaccine (Astra Zeneca) in a women. Our case presentation was not strictly typical, with occurence of lower limb weakness, gait ataxia (and some sensory disorders).
In GBS, the increase in protein in the liquor is observed in 66% of cases in the first week, and in 82% of cases in the second week [35]. At the time we performed lumbar puncture, there wasn’t a clear albuminocytologic dissociation, but the electrophysiological study revealed neurophysiological finding indicative of acute demyelinating sensory-motor polyneuropathy (AIDP) in the 4 limbs.
In some GBS post COVID-19 vaccine already described, therapy with IV Ig exhibited only a marginal effect [28,29].
In our case, after an initial clinical recovery with clear benefit of therapy and physiotherapy, our patient presented treatment-related fluctuation (TRF). Treatment related fluctuation (TRF) is defined as at least one grade increment in the GBS disability scale after completion of immunotherapy (immunoglobulin in this case) followed by at least one grade worsening of the disability scale within the first two months after disease onset [36]. Often treatment-related fluctuation (TRF) required repeated IVIg treatment [30].
Despite uncertain benefit and and the evidence of recent literature [37], after a second dose of immunoglobulins (0.4 g/kg/day for 5 days every time one month apart), there was, and is still ongoing, a subsequent gradual new recovery. We’ve found to date only one other described cases of GBS post COVID vaccine that have presented TRF [38]; also in this case patient was successfully treated with reinstitution of immunoglobulin therapy.
Conclusions
To date, a potential association between the adenovirus vector vaccines (Janssen/Johnson & Johnson COVID-19 vaccine and AstraZeneca COVID-19 vaccine) and Guillain-Barrè syndrome (GBS) is being investigated.
We have reported another vaccine-associated Guillain–Barrè syndrome case due to Sars Cov 2 vaccine (Astra Zeneca) in a women; it was responsive to therapy with immunoglobulins, that, repeated and together with physiotherapy, led the patient to a gradual recovery. About 10% of GBS patients have a secondary deterioration within the first 8 weeks after start of IVIg (treatment-related fluctuation: TRF) (36)- but we do not know yet the frequency of TRF in this GBS subgroup)- that are treated repeating IVIg treatment. Generally, second course of IVIG is not beneficial for patients with severe Guillain-Barrè syndrome (37), but we don’t know if in this GBS subgroup therapeutic outcome may differ.
Based on the available data, the US FDA and CDC and European regulators affirm that the benefits of these vaccines outweigh their risks (43, 44). Someone, for people with a documented history of GBS, prefers suggest using COVID-19 vaccines other than adenovirus vector vaccines (exacerbation of previous GBS after viral vector vaccine has also been observed and described: (45)); this may be a reasonable choice to date, pending further data, but the safety of all available anti Sars Cov2 vaccines is confirmed.
- Walling AD, Dickson G (2013) Guillain–Barrè syndrome Am Fam Physician 87: 191- 7.
- Alshekhlee A, Hussain Z, Sultan B, Katirji B (2008) Guillain-Barré syndrome: incidence and mortality rates in US hospitals. Neurology 70: 1608–13.
- Rees JH, Soudain SE, Gregson NA, Hughes RA (1995) Campylobacter jejuni infection and Guillain- Barrésyndrome.AU N Engl J Med 333: 1374.
- Hao Y, Wang W, Jacobs BC, Qiao B, Chen M, et al. (2019) Antecedent infections in Guillain- Barrésyndrome: a single-center, prospective study. AU Ann Clin Transl Neurol 6: 2510.
- Orlikowski D, Porcher R, Sivadon-Tardy V, Quincampoix JC, Raphaël JC, et al. (2011) Guillain-Barrésyndrome following primary cytomegalovirus infection: a prospective cohort study. AU Clin Infect Dis 52: 837.
- Steininger C, Popow-Kraupp T, Seiser A, Gueler N, Stanek G, et al. (2004) Presence of cytomegalovirus in cerebrospinal fluid of patients with Guillain-Barre syndrome. AU J Infect Dis 189: 984.
- Espinosa PS, Rizvi Z, Sharma P, Hindi F, Filatov A (2020) neurological complications of coronavirus disease COVID 19 encephalopathy, MRI brain and cerebrospinal fluid findings: case 2. Cureus 12: e7930.
- Sivadon-Tardy V, Orlikowski D, Porcher R, Sharshar T, Durand MC, et al. (2009) Guillain-Barrésyndrome and influenza virus infection. AU Clin Infect Dis 48: 48.
- Brannagan TH 3rd, Zhou Y HIV-associated Guillain-Barrésyndrome. AU J Neurol Sci 208: 39.
- Parra B, Lizarazo J, Jiménez-Arango JA, Zea-Vera AF, González-Manrique G, et al. (2016) Guillain-BarréSyndrome Associated with Zika Virus Infection in Colombia. AU N Engl J Med 375: 1513.
- Cao-Lormeau VM, Blake A, Mons S, Lastère S, Roche C, et al. (2016) Guillain-BarréSyndrome outbreak associatedwith Zika virus infection in French Polynesia: a case-control study. AU Lancet. 387: 1531.
- Rudant J, Dupont A, Mikaeloff Y, Bolgert F, Coste J, et al. (2018) Surgery and risk of Guillain- Barrésyndrome: A French nationwide epidemiologic study. AU Neurology 91: e1220.
- Menveo (meningococcal groups A, C, Y, and W-135 oligosaccharide diphtheria CRM197 conjugate vaccine). US Food and Drug Administration (FDA) approved product information. Revised December, 2019. US National Library of Medicine.
- MenQuadfi (2020) US Food and Drug Administration (FDA) approved product information. October, 2020. US National Library of Medicine.
- Menactra (2018) US Food and Drug Administration (FDA) approved product information. Revised April, 2018. US National Library of Medicine.
- Stowe J, Andrews N, Wise L, Miller E (2008) Investigation of the temporal association of Guillain-Barre syndrome with influenza vaccine and influenzalike illness using the United Kingdom General Practice Research Database. AU Am J Epidemiol. 169: 382.
- Tam CC, O'Brien SJ, Petersen I, Islam A, Hayward A, Rodrigues LC Guillain-Barrésyndrome and preceding infection with campylobacter, influenza and Epstein-Barr virus in the general practice research database. AU PLoS One 2: e344.
- Helms J, Kremer S, Merdji H, Clere-Jehl R, Schenck M, et al. (2020) Neurologic Features in Severe SARS-CoV-2 Infection N Engl J Med 382: 2268.
- Filatov A, Sharma P, Hindi F, Espinosa PS (2020) Neurological complications of Coronavirus disease (COVID 19): encephalopathy. Cureus 12: e7352.
- Montalvan V, Lee J, Bueso T, De Toledo J (2020) Neurological manifestations of COVID-19 and other coronavirus infections: A systematic review.Clin Neurol Neurosurg 194: 105921.
- Liotta EM, Batra A, Clark JR, Shlobin NA, Hoffman SC, et al. (2020) Frequent neurologic manifestations and encephalopathy-associated morbidity in Covid-19 patients. Ann ClinTransl Neurol 7: 2221.
- Toscano G, Palmerini F, Ravaglia S, Ruiz L, Invernizzi P, et al. (2020) Franciotta D, Baldanti F, Daturi R, Postorino P, Cavallini A, Micieli G Guillain-BarrèSARS-CoV 2. N Engl J Med 382: 2574-6.
- Abu-Rumeileh S, Abdelhak A, Foschi M, Tumani H, Otto M (2020) Guillain-Barrésyndrome spectrum associated with COVID-19: an up-to-date systematic review of 73 cases. J Neurol 268: 1133.
- Greene SK, Rett MD, Vellozzi C, Li L, Kulldorff M, et al. (2013) Guillain- BarréSyndrome, Influenza Vaccination, and Antecedent Respiratory and Gastrointestinal Infections: A Case- Centered Analysis in the Vaccine Safety Datalink, 2009-2011. AU PLoS One 8: e67185.
- Kwong JC, Vasa PP, Campitelli MA, Hawken S, Wilson K, et al. (2013) Risk of Guillain-Barré syndrome after seasonal influenza vaccination and influenza health-care encounters: a self-controlled study. AU Lancet Infect Dis 13: 769.
- Chen RT, Rastogi SC, Mullen JR, Hayes SW, Cochi SL, et al. (1994) The vaccine adverse event reporting system (VAERS). Vaccine 12: 542–50.
- F Aomar-Millan, J Martinez de Victoria-Carzo, JA Peregrina-Rivas (2019) COVID-19, Guillain Barrè y vacuna. Una mezcla peligrosa, Revista Clinica Espanola.
- Shreena Umit Patel, Ruhaid Khurram, Anjali Lakhani, Bernardine Quirk (2021) Guillain Barre syndrome following the first dose of the chimapnzee adenovirus-vectored COVID-19 vaccine, ChAdOx1. BMJ Case Rep 14: e242956.
- Boby V Marmattom, Parameswaran Khrisnan, Reji Paul, Sandeep Padmanabhan Soumya Cherudal Vishnu Nampoothiri, Akheel A (2021) Syed FRCP Halinder S. Mangat “guillain-Barrè Syndrome following ChAdOx1-S/nCoV-19 Vaccine. Ann Neurol 00: 1-3
- Pieter A van Doorn (2013) Quarterly Medical Review “Diagnosis, treatment and prognosis of Guillain-Barrè syndrome (GBS) La Presse Mèdicale 42: e193-e201.
- Updated GTH statement on vaccination with the AstraZeneca COVID-19 vaccine, as of March 22, 2021.
- Shreena Umit Patel, Ruhaid Khurram, Anjali Lakhani, Bernardine Quirk (2021) Guillain Barre syndrome following the first dose of the chimapnzee adenovirus-vectored COVID-19 vaccine, ChAdOx1” BMJ Case Rep 14: e242956.
- Boby V Marmattom, Parameswaran Khrisnan, Reji Paul, Sandeep Padmanabhan Soumya Cherudal Vishnu Nampoothiri, Akheel A. Syed FRCP Halinder S. Mangat “guillain-Barrè Syndrome following ChAdOx1-S/nCoV-19 Vaccine. Ann Neurol 00: 1-3.
- Jospef Finsterer (2021) Exacerbating Guillain-Barrè Syndrome Eight Days after Vector-Based COVID-19 Vaccination. Hundawi Case Report in Infectious Disease 2021: 1-3.
- Christian Fokke (2014) Brain 137: 33-43.
- Visser LH, van der Meché FG, Meulstee J, van Doorn PA (1998) Risk factors for treatment related clinical fluctuations in Guillain-Barré syndrome. Dutch Guillain-Barré study group. J Neurol Neurosurg Psychiatry 64: 242–4.
- Walgaard C, Jacobs BC, Lingsma HF, Steyerberg EW, van den Berg B, et al. (2021) Study Group Second intravenous immunoglobulin dose in patients with Guillain-Barrésyndrome with poor prognosis (SID-GBS): a double-blind, randomised, placebo-controlled trial. Lancet Neurol 20: 275.
- Hadden RD, Cornblath DR, Hughes RAC, Zielasek J, Hartung HP, et al. (1998) Electrophysiological classification of Guillain-Barré syndrome: clinical associations and outcome. Ann Neurol 44: 780-8.
- Asbury AK, Arnason BGW, Karp HR, McFarlin DE (1978) Criteria for diagnosis of Guillain Barrè syndrome. Ann Neurol 3: 565-6.
- Asbury AK, Cornblath DR (1990) Assesment of current diagnostic criteria for guillain Barrè syndrome Ann. Neurol 27: S21-S24.
- Willison HJ, Jacobs BC, Van Doorn PA (2016) Guillain Barrè sindrome. Lancet 388: 717-27.
- Subhadeep Gupta, Atanu Chandra, Biman Kanti Ray,Alak Pandit (2020) Treatment related fluctuation and response to intravenous immunoglobulin therapy in post COVID-19 Guillain-Barre syndrome. Case Reports Diabetes Metab Syndr 15: 102246.
- FDA COVID-19 Response (2021).
- European Medicines Agency (2021).
- Jospef Finsterer (2021) Exacerbating Guillain-Barrè Syndrome Eight Days after Vector-Based COVID-19 Vaccination. Hundawi Case Report in Infectious Disease 2021: 3.
FIGURE 1
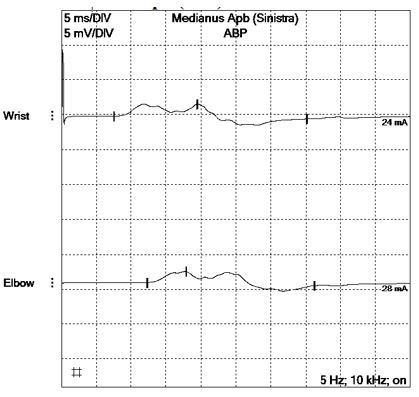
Figure 1: Motor Medianus Apb (Left)
FIGURE 2
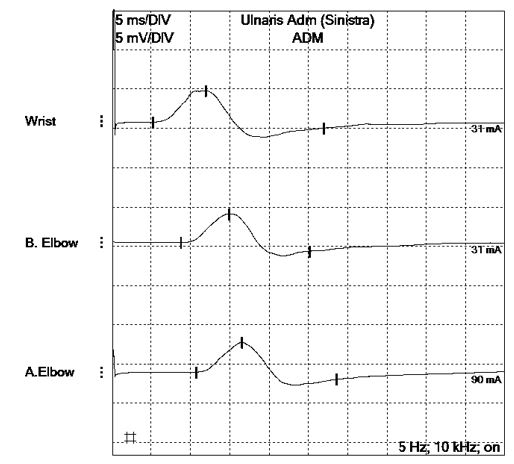
Figure 2: Motor Ulnaris Adm (Left)
FIGURE 3
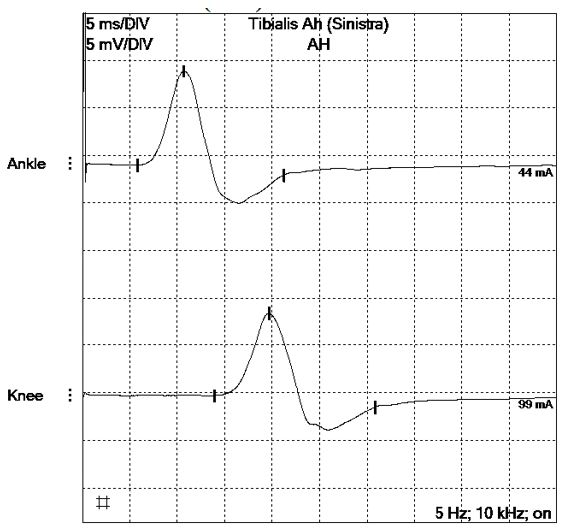
Figure 3: Motor Tibialis Ah (Left)
FIGURE 4
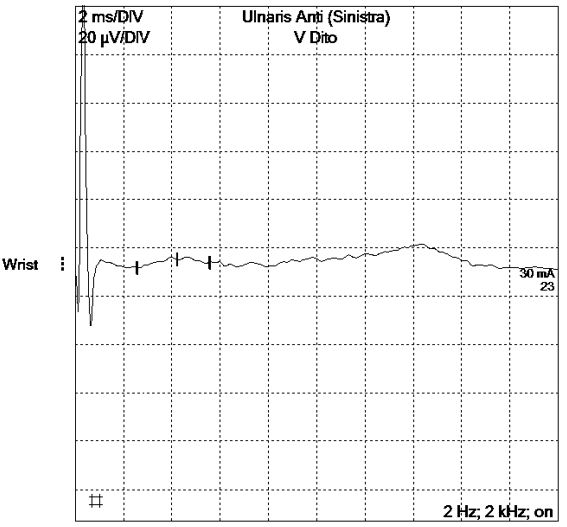
Figure 4: Sensory Ulnaris Anti (Left)
FIGURE 5
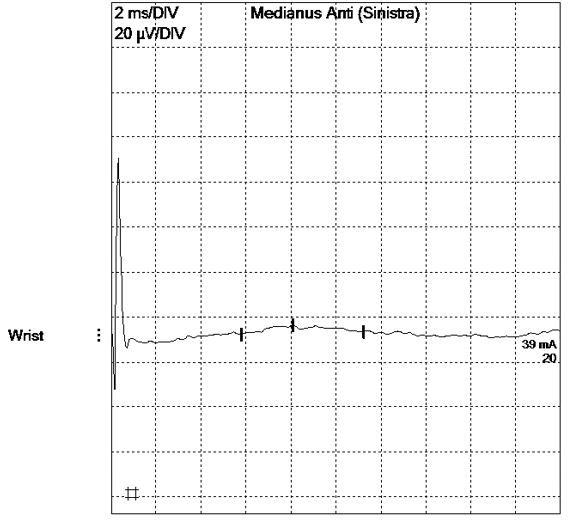
Figure 5: Sensory Medianus Anti (Left)
FIGURE 6
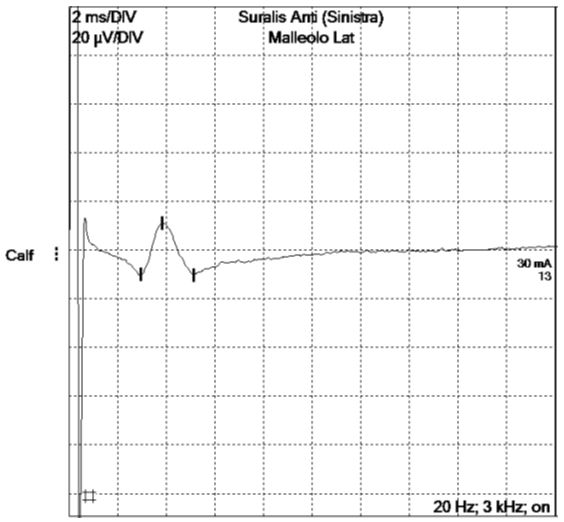
Figure 6: Sensory Suralis Anti (Left)
FIGURE 7
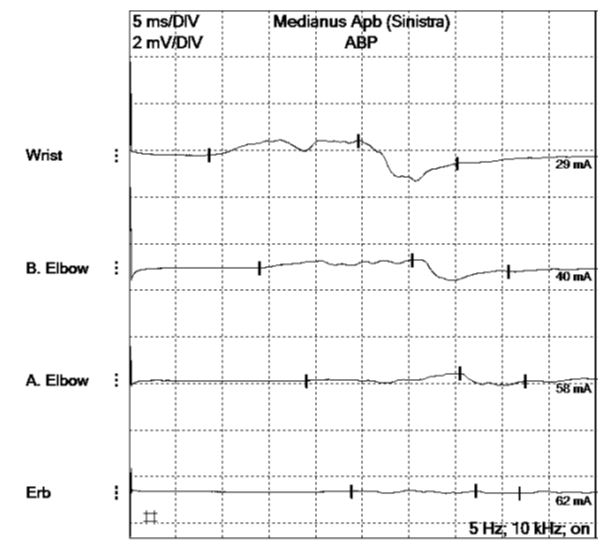
Figure 7: Motor Medianus Apb (Left)
FIGURE 8
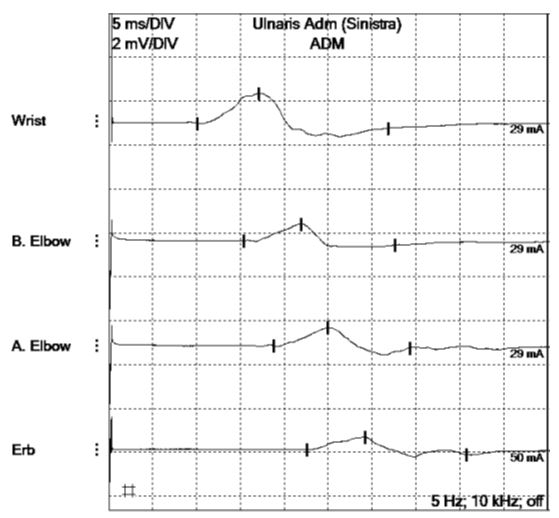
Figure 8: Motor Ulnaris Adm (Left)
FIGURE 9
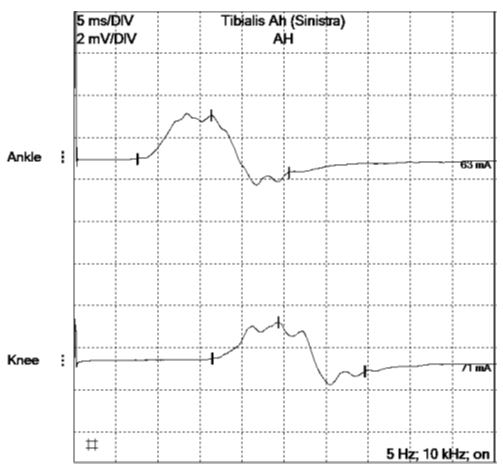
Figure 9: Motor Tibialis Ah (Left)
FIGURE 10
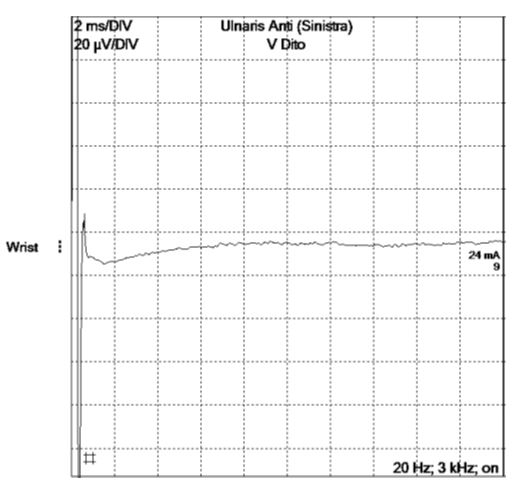
Figure 10: Sensory Ulnaris Anti (Left)
FIGURE 11
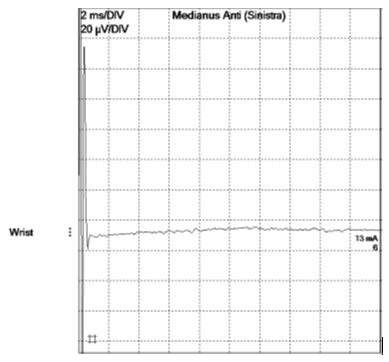
Figure 11: Sensory Medianus Anti (Left)
FIGURE 12
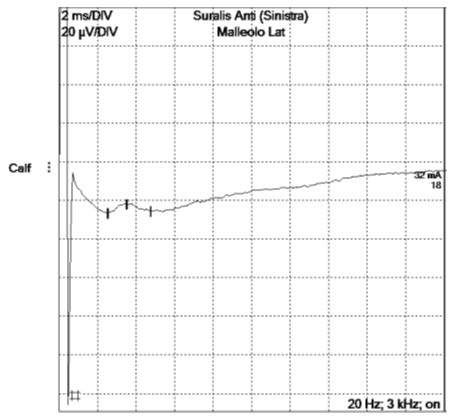
Figure 12: Sensory Suralis Anti (Left)
FIGURE 13
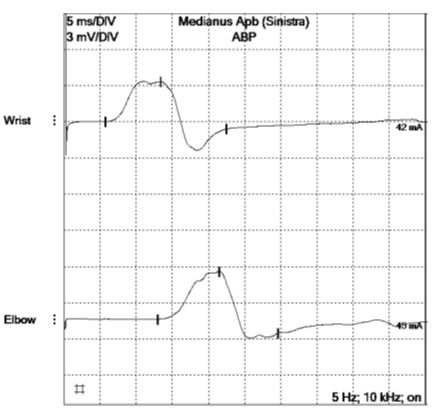
Figure 13: Motor Medianus Apb (Left)
FIGURE 14
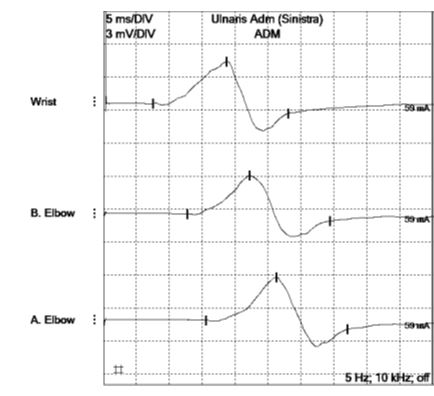
Figure 14: Motor Ulnaris Adm (Left)
FIGURE 15
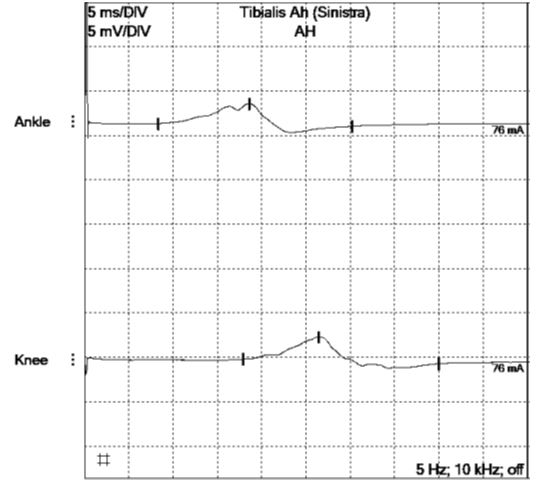
Figure 15: Motor Tibialis Ah (Left)
FIGURE 16
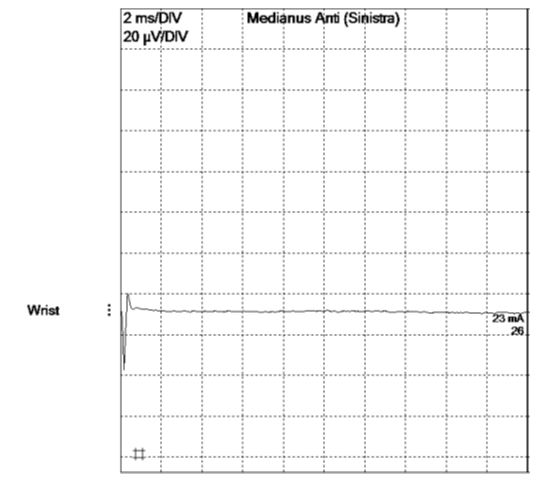
Figure 16: Sensory Medianus Anti (Left)
FIGURE 17
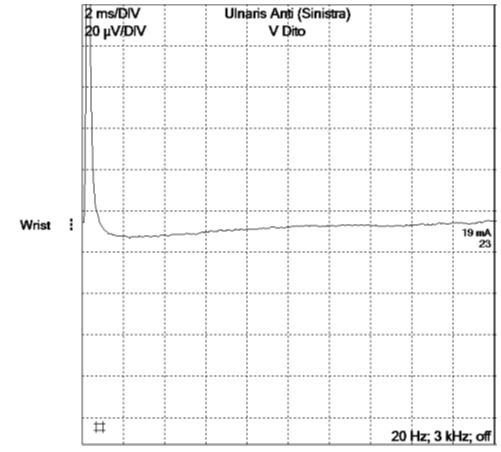
Figure 17: Sensory Ulnaris Anti (Left)
FIGURE 18
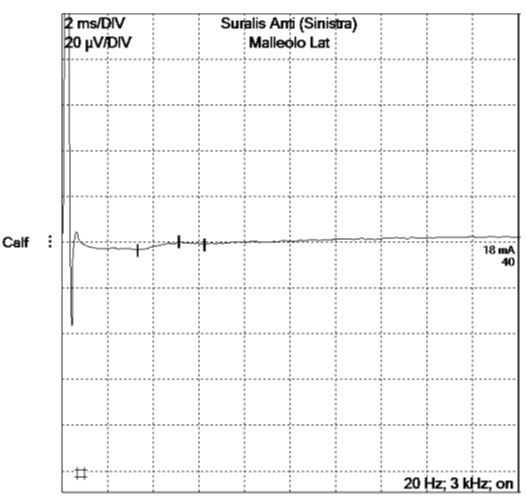
Figure 18: Sensory Suralis Anti (Left)
Tables at a glance
Figures at a glance
Figure 1
Figure 2
Figure 3
Figure 4
Figure 5
Figure 6
Figure 7
Figure 8
Figure 9
Figure 10
Figure 11
Figure 12
Figure 13
Figure 14
Figure 15
Figure 16
Figure 17
Figure 18