A Review on Technological and Manufacturing Advancement of Transdermal Patch for Effective Management of Alzheimer Disease
Received Date: December 28, 2023 Accepted Date: January 28, 2024 Published Date: January 31, 2024
doi: 10.17303/jnsm.2024.10.101
Citation: Vanshita Hardiya, Dr. Shashikant Bagade, Akshita Rana, Krisha Patel, Nishi Mohile (2024) A Review on Technological and Manufacturing Advancement of Transdermal Patch for Effective Management of Alzheimer Disease. J Nanotech Smart Mater 10: 1-13
Abstract
Alzheimer's Disease International estimates a dementia prevalence of over 50 million people globally in 2018, with the number expected to quadruple by 2050, with two-thirds residing in low- and middle-income nations.20 According to the most recent estimates, dementia prevalence in Europe will more than double by 2050.Alzheimer's disease is the leading cause of dementia and is rapidly becoming one of the most costly, fatal, and burdensome diseases of the twenty- first century. There is various root of administration are available for AD but one the best is TDDS in the form of patch. This article covers Transdermal Drug Delivery for Alzheimer disease, the importance, advantages, disadvantages, type and basic component of transdermal patch, mainly including use of nanoparticle and microneedle in transdermal patch drug delivery along recent advancement in transdermal patch like use of smart patch that can be used for AD in future. And overall this article provides brief introduction about application and future challenges of transdermal patch for AD.
Keywords: Transdermal Patch; Alzheimer Disease; Manufacturing Advancement; Technological Advancement
Introduction
Alzheimer’s disease (AD) dementia is refers to a particular onset and course of cognitive and functional decline associated with age together with a particular neuropathology. It was first described by Alois Alzheimer in 1906 about a patient whom he first encountered in 1901. It is a neurodegenerative disorder.
Alzheimer's disease is described by various hypothesis: Tau hypothesis, Amyloid Hypothesis and on the basis of Oxidative Stress Reactive oxygen species, Cellular and Vascular Dysfunction Advancing age, vascular risk factors, Cholesterol, Metal Imbalance, and Cholinergic Deficit During the progression of AD [1].
An additional method of administering medications through the skin layer is transdermal drug delivery [1]. Before the medication reaches the target region, it is absorbed through the skin into the bloodstream and circulated throughout the body [2,3]. Compared to other administration methods, transdermal medication delivery provides a number of benefits. Examples include the capacity to administer medication in continuous doses over an extended period of time, the ability to omit the digestive tract, and the capacity to prevent first- pass liver metabolism [4]. Other drug delivery methods, such intravenous, can hurt and raise the risk of infection. However, the oral route is ineffective, and the breathing technique makes dosage management challenging. Transdermal administration is frequently used to give medications for illnesses like quitting smoking, chronic pain, motion sickness, and hormone replacement therapy due to its advantages over conventional routes.
A transdermal patch is a medicated patch that can administer medications to the bloodstream at a controlled rate via the layers of skin. In actuality, applying medication using patches is the most practical technique. They are noninvasive, and the course of treatment may persist for many days before being discontinued. They have several ingredients and come in various sizes. The patch can use diffusion processes to transport active chemicals into the systemic circulation after being placed to the skin. High concentrations of active ingredients may be present in transdermal patches, which stay on the skin for a long time.
AdvantagesXontinuous administration, multiple-day therapy, circumvent the digestive system, do not use first-pass metabolism, it is less intrusive and can be stopped at any time [1].
DisadvantagesSkin irritation, inconsistent absorption, patch failure, and a limited dose option are all issues with this medicine [1].
Purpose and ScopePurpose of this study is to collect data about technological advancement and manufacturing advancement through out the years. Examining recent advances in formulation is critical for staying current, enhancing formulation delivary, complying with laws, remaining competitive, and grabbing possibilities for innovation and efficiency. It's a proactive strategy to making ensuring your formulas are as effective and current as feasible.
Transdermal Patch DesignDrug transport over the skin is influenced by a number of parameters, including skin permeability, application area and duration, and skin metabolic activity. (i.e., first pass metabolism). In fact, each medicine has distinct features that can influence transdermal delivery. To breach the skin barrier and obtain optimal skin absorption and penetration, the medicine should be non-ionic and somewhat lipophilic. Molecules Larger than 500 Daltons make crossing the stratum corneum problematic, and the therapeutic dosage of the medicine should preferably be less than 10 mg per day [1].
Transdermal Drug Delivery for Alzheimer diseaseOral drug delivery systems have issues such as first-pass metabolism, limited efficacy, and low bioavailability, treating Alzheimer's disease is difficult. There are also alternate delivery modalities available, such as intranasal and transdermal administration. The transdermal medication delivery technique provides for the continuous release of active ingredients/drugs while avoiding first-pass metabolism and thereby reducing systemic adverse reactions.
Some drugs have been approved by FDA Rivastigmine (cholinesterase inhibitor) and tacrine, donepezil, galantamine and memantine as (antagonists of the NMDA receptor). This drug provides prolonged benefit for symptoms of Alzheimer's disease [14].
Cholinesterase InhibitorsAccording to the oldest theory, AD is caused by a shortage of acetylcholine. Transdermal administration may make it easier to transfer drugs through the skin easily and reliably, while also providing long-term efficacy with relatively low doses [15]. They act by binding with cholinesterase enzyme and maintain acetylcholine level by decreasing its breakdown rate.
PhysostigminePhysostigmine was the first anticholinesterase medication used transdermally to treat Alzheimer's disease. Certain difficulties with physostigmine oral and intravenous administration can be mitigated using a patch, including lower bioavailability, a narrow therapeutic window, high first-pass metabolism, and poor user compliance [16]. In 1986, Levy et al. produced a patch containing physostigmine in the enhancer carrier propionic acid and a vinyl acetate/ethylene copolymer membrane with an aluminium foil cover on one side and an adhesive on the other [15]. Another transdermal medication administration of Physostigmine was created to avoid first pass metabolism and reduce dose frequency when compared to the oral route. Transdermal patches of the matrix type were produced. was determined to be the best, with 96.5% medication release in 12 hours [17].
TacrineTacrine was one of the experimental drugs utilised in the early stages of transdermal therapy techniques for Alzheimer's disease. Tacrine possesses a reversible cholinesterase inhibitor as well as being lipophilic and weak base, making passive diffusion difficult, hence ion-exchange fibres and iontophoresis were used to transport the molecule [18]. A develop matrix based transdermal patches containing Tacrine to overcome the first pass metabolism and to reduce frequency of dosing compared to oral route. Among all formulation, formulation that contain Methocel K15M 100 mg had shown 97.61% % cumulative drug release within 12 hours [19].
RivastigmineThe rivastigmine transdermal patches was first developed in the 1970s and received FDA clearance in 1979 [20]. there is difference between Cmax oral solution verses transdermal patch. For oral (3 mg oral solution) it reaches .63 ng/mL in 1hr on average and it shows elimination halflife 1.45 h. transdermal patch (9.5 mg/24 h) Cmax reaches at 5.84 ng/mL after a 14.1 h and it shows elimination halflife 3.02 h. and studies conclude that rivastigmine patch shows 14-time longer Tmax and 20% lower Cmax then oral solution [14].
The first generation of patches was a basic reservoir made comprised of an alcohol-based drug and a solution-soaked sticky edge composed of a plastic sheet; nonetheless, this device caused skin pain. The next stage in developing the matrix patch was to fix this problem. The four layers of this approach enable the drug release uniformly, decreasing skin concerns and boosting adherence time [21]
In a single layer, this patch comprises the medicine, antioxidants, the polymer matrix, and a silicon matrix adhesive. As a result of this endeavour, the patch's thickness and surface were reduced, resulting in medication delivery that was based on patient compliance, as seen in Figure 2. This patch was available on the market in three different sizes (5 cm2, 10 cm2, and 15 cm2), and its flow rate per 24 hours was exactly proportionate to its size (4.6 mg, 9.5 mg, and 13.3 mg, respectively [22]. Chitosan, an Ndeacetylated derivative of chitin, is the novel drug reservoir or drug carrier for controlled release due to the structural flexibility of mechanical and chemical manipulation [23].
DonepezilThe transdermal application of donepezil's prescribed dose form was evaluated in late 2008. Because of the enzyme's great potency and selectivity in the CNS, it is the most efficient cholinesterase inhibitor [24]. There is difference between Cmax oral verses transdermal patch of donepezil. For oral it ranges from 3.2–11.6 ng/mL after 3.2–4.7 h and its elimination half-life ranges from 53.8 to 82.8 h. transdermal patch Cmax ranges from 5.24 to 20.36 ng/mL at 74 to 76 h and its elimination half-life is ranges from 63.77 to 94.07 h [1]. So different study proposed various type patches like Drug-matrix-in-adhesive patches and drug-reservoir-in-adhesive patches were proposed by Valia et al. The migration of medicine from the reservoir into and through the adhesive layer resulted in a faster input of functional material in the second edition. These approaches enabled controlled release by modifying the patch's active surface, which comes into direct contact with the skin surface [14]. To improve compliance, a new method of delivering DPZ via transdermal patch was devised. By dissolving dicarboxylic acid and DPZ in ethanol, ionic linkages were formed, resulting in a stable ionic liquid (IL) state. In both in vitro and ex vivo skin permeability investigations, DPZ ILs and DPZ IL patch formulations fared better than the DPZ free-base patch [25].
Another approach for increasing distribution across the skin, efforts to improve skin permeability are being studied extensively, with microneedles showing great promise. Hydrogel-forming microneedles are placed into the skin, and after dissolving a drug-loaded reservoir and moving the drug via the formed channels, the microneedle array is withdrawn intact and may be securely discarded. In vitro penetration of donepezil hydrochloride from patch was 54.71g122.71g in 24 hours, while animal model plasma values were 51.817.6ng/mL [5].
PhenserinePhenserine, a physostigmine derivative, was initially reported as an acetylcholinesterase (AChE) inhibitor. It reduces APP translation, which reduces the quantity of - amyloid precursor protein (APP) in neuronal cell culture. Phenserine is additionally distinct due to the different effects of its enantiomers: The potent enantiomer for AChE inhibition is (-)- phenserine, but (+)-phenserine ('posiphen ') has limited action as an AChE inhibitor and may be dosed considerably higher. Phenserine has the same drawbacks as other anticholinesterase medications, such as digestion, metabolism, and first-pass hepatic absorption. PST phase 3 studies in Europe show that the duration of action may restrict any clinically significant activity of PST. So transdermal formulations of PS and PST (ointment/ patch) were created and characterised in vitro and in vivo to minimise the kinetic limits of first-pass metabolism. They believe that advantages over oral treatments may include avoiding first-- pass metabolic effects and improving dosage compliance [26].
GalantamineGalantamine is a competitive, reversible tertiary alkaloid AChE inhibitor. The medication targets AChE (selective) rather than butyrylcholinesterase. Galantamine, in addition to inhibiting AChE, interacts allosterically with nicotinic acetylcholine receptors to enhance the effect of agonists at these receptors [27]. Galantamine was created as a drug-in-adhesive transdermal patch to offer a new therapy option for Alzheimer's patients. The impacts of formulation features such as pressure-sensitive adhesives, enhancers, and medication concentration were investigated [28]. Another formulation was developed as an optimised matrix-type patch for transdermal distribution of galantamine free base using four pressure sensitive adhesives (each with a different functional group). The diffusion release kinetics of an optimised patch were well matched with Higuchi's model, providing a permeation rate of 32.4 1.41 g/cm2/h over human cadaver skin [29].
Noncompetitive N-Methyl-D-Aspartate
MemantineMemantine has been licenced for the treatment of moderate to severe Alzheimer's disease dementia in the United States and the European Union. Memantine (Ebixa, Axura, Namenda, Akatinol) is a voltage-dependent, moderate-affinity NMDA-receptor antagonist with fast on/off kinetics that inhibits excessive calcium influx produced by chronic NMDA receptor overstimulation [46]. Increased NMDA receptor activation was thought to be a role in cholinergic cell degeneration. Memantine works by inhibiting NMDA receptors during the extended-release of low glutamate concentrations. It was developed in a transdermal dose form as an alternative therapeutic method for Alzheimer's disease [30].
Some another formulation like fabricated patches were prepared for memantine, and from all of them Formulation B2 containing 137.5 mg HPMC, 400 mg EC, and 300 mg xanthan gum had a flux of 212.24 g/cm2/h, permeability of 2.32 cm/h, and 27.95% release at 8h, with first-order and non-Fickian drug release kinetics. It was non-irritating, and in vitro release experiments revealed that it may be released for up to 48 hrs. In vivo experiments in rabbits revealed that the patches provided better medication absorption and sustained release than tablets [31].
Other Drugs
Huperzine AHuperzine A is a substance derived from the plants Chinese club moss (Huperzia serrata) or fir club moss (Huperzia selago). It can also be created in a laboratory. People with Alzheimer's disease or other kinds of dementia take huperzine A to enhance memory and mental function. It is also claimed to treat depression, schizophrenia, and a variety of other diseases, although there is no solid scientific evidence to back up these claims. Qinying Yan et al. investigate the efficacy of a dissolving microneedle patch (DMNP) as a transdermal delivery device for Hup A. In vivo pharmacokinetic research revealed that the DMNP group had a twofold longer Tmax, a fivefold longer t1/2, a lower Cmax (3:4), and a twofold bigger AUC (0-1) than the oral group at the same dosage of Hup A. Pharmacodynamic studies revealed a substantial improvement in cognitive performance in AD rats treated with DMNP-Hup A and OralHup A compared to the control group. These findings show that this predesigned DMNP is a potential option for delivering Hup A transdermally for the treatment of Alzheimer's disease [32].
Newer Techniques for Trasdermal Patch Based Delivery
Microneedle-Based PatchesMN technology is a type of active transdermal medicine delivery intended to replace traditional syringe injections. The MN array is used to non-invasively penetration the stratum corneum and distribute the medicament. These arrays are made up of micro-sized needles with heights ranging from 25 to 2000 nanometers. MNs have been employed in a variety of applications, including medicine and vaccine administration, cosmetics, and illness diagnosis.
External factors like as skin physiology, physiochemical properties, and environmental conditions can all have an impact on the MN drug delivery route. These include the relative humidity and temperature in the surrounding area. Excess water and the presence of other salts will interfere with drug release kinetics, altering the osmotic gradient for transdermal drug delivery. Excessive sweating can also prevent the microneedle patch from sticking to the skin, reducing medicine elution through the skin. Similarly, medicine penetration into the stratus corneum and beyond can be reduced by either low or extremely high pH values near the skin [33].
Excessive lipid film formation on the skin forms a barrier layer to the stratus corneum, and defatting this layer can help with transdermal absorption and in case raising skin temperature can improve medication penetration by increasing diffusivity and vasodilation of skin arteries [34]. When compared to the oral route, the pharmacokinetics of microneedles indicate quick absorption in the circulation, which might be useful for treating localized disorders with considerably lower drug loading. When opposed to solid microneedles, hollow microneedles act as drug reservoirs and have the ability to carry greater doses. Solid microneedles constructed of ceramic or metal materials can be coated with very accurate drug formulations utilizing inkjet and spray atomization processes.The amount of medicine loaded for microneedle depends heavily on the medication kind, intended treatment plan, and patient profile. Because of the control over manufacturing processes and drug loading methods, MNs provide a very accurate delivery mechanism [35]. Microneedle devices are currently available (single needle with applicator, microneedle array patch, microneedle pen, microneedle pump patch, and microneedle roller) [36]. According to a recent Future Market Insights study, the Minnesota drug delivery system market will be worth $1.2 billion by 2030, with a compound annual growth rate (CAGR) of 6.6% [37].
There are some Advantages of MN:- MN is regarded as one of the greatest methods for transdermal medication administration since pharmaceuticals supplied through this approach bypass critical human organs such as the liver.
- Furthermore, by offering a pain-free experience, it removes the suffering associated with IV injection so as a result, it is regarded as the greatest option for persons who are afraid of needles (trypanophobia). Because microneedle transdermal medication administration does not require skilled staff, it is simple to utilize
- Furthermore, the stratum corneum acts as a barrier, preventing therapeutic agent molecules from passing through the skin and reaching the epidermis or dermis layers, reducing the risk of infection entering the body
- In contrast, a microneedle may pass through the stratum corneum barrier and deliver drugs into the epidermis or higher dermis layer without producing discomfort. The MN array is also long enough to penetrate the stratum corneum while being short enough to avoid skin injury or contact with nerve terminals, making it painless [38].
- Using a microneedle for transdermal drug administration has drawbacks such as increased application time, many patches within a given region, a certain mechanical strength need, and a suitable biocompatible material.
- The micro needle patch method may have an impact on dosage settings and may result in undesirable side effects.
The kinetic effectiveness of the MN device is also dependent on it being perpendicular to the skin surface; otherwise, the medication dosage may escape or the needles may struggle to enter the skin at non-conformal angles. Furthermore, repeated use of microneedles may cause scarring on the skin's surface. There may also be flaws in the geometries and shapes of needle formations that limit their efficacy. Hollow MNs, for example, may have their micropores blocked due to compressed tissue in particular skin types, altering their delivery kinetics and penetrability. However, there are inherent limitations to adopting TDD technologies in general that are not unique to MNs. Examples include skin irritation, redness, pain, edoema, and infection at the application site [38].
Nanoparticle-Based Drug DeliveryNPs used to transport medications across the BBB range in size from 1-100 nm. Nanoparticles who can target Alzheimer disease should have these properties: (A) Liposomes containing AchE inhibitors that target cholinergic system dysfunction.
(B) 1. Anti-tau medication including SLNPs and functionalized phosphatidylserine that targets hyperphosphorylated tau proteins.
2. PLGA-PEG with anti-A antibody aids in the targeting, solubilization, and clearance of A fibrils
(C) AuNP modified with capture antibody targeting A and tau proteins, forming a sandwich with secondary antibody for identifying AD hallmarks. AchE is for acetyl-cholinesterase; NMDA stands for N-methyl D-aspartate antagonist; A stands for amyloid beta fragment; PEG stands for polyethylene glycol; SLNP stands for solid lipid nanoparticle; NP stands for nanoparticle; PLGA stands for poly D,Llactic-co-glycolic acid; AuNP stands for gold nanoparticle [40].
Types of Nanoparticle- Liposomes: Liposomes are tiny vesicles with spherical, double-layered phospholipid bilayer membranes. The liposomes' interior compartment can be employed to transport hydrophilic payloads. When incorporated into liposomes, commercially available AD treatments such as galantamine, rivastigmine, and donepezil demonstrated effective penetration and increased bioavailability.
- Micelles: Micelles are spherical amphiphilic drug carriers with particle sizes ranging from 5 to 50 nm, each with a unique hydrophilic shell and hydrophobic centre. The hydrophilic shell makes micelles water soluble, allowing for intravenous delivery, while the hydrophobic centre delivers medicinal drugs.
- Solid Lipid NPs (SLNs): At room and physiological temperatures, SLNs are solid-state lipid-based network structures 50-1000 nm in diameter with a lipid-forming core. These SLNs allow for high trapping and regulated release of hydrophobic medicines. SLN has now established itself as a reputable drug carrier system capable of transporting active medicinal cargo across the BBB to particular target locations in the brain.
- Polymeric NPs (PNPs): PNPs are solid carriers made of natural or manmade polymeric polymers containing nanosized colloidal organic molecules. Recently, a wide range of polymers have been studied with the objective of developing PNPs capable of targeted drug delivery for the treatment of Alzheimer's disease.
- Dendrimers: Dendrimers are molecules that are regularly branched and have a well-defined and multivalent 3D shape. A dendron is the sole functional unit of a dendrimer that germinates branches. The cargo medications are either connected to the dendrimer's surface or encapsulated within its branches.
- Nanoemulsions (NEs): Es are nanosized isometric mixes of oil and aqueous phases that have been stabilised by surfactant or co-surfactant molecules to create a single phase. High-pressure homogenization, ultrasonication, and an emulsion inversion point are used to prepare them
- Inorganic NPs: Organic nanoparticles are made up of a wide variety of materials, including gold, silver, aluminium, and silicon dioxide. They are non-toxic, hydrophilic, biocompatible, and extremely stable in comparison to organic materials. They have received significant attention in preclinical research as prospective diagnostic and therapeutic systems for a wide range of applications, including imaging, medication delivery, and radiation development [40].
- Smart Patches: A team of researchers developed a smart patch sensor technology in 2014 that uses microneedles to monitor intradermal glucose constantly and painlessly in diabetics. With the use of sensors and other technology, smart patches are able to monitor patient conditions and adjust the way that medications are administered [41].
- Dissolving/Degradable Patches: These patches don't need to be taken off or disposed of because they are meant to dissolve into the skin. Usually made of biodegradable materials, these patches are absorbed by the body after use. In a proof-of-concept paper published in 2019, researchers effectively administered the antibiotic gentamicin via a dissolving patch in a mouse model of bacterial disease [42].
- Three-Dimensional (3D)-Printed Patches: Researchers are employing 3D printing technology to develop customized transdermal patches that may be adjusted to each patient's specific needs. A 3D-printed patch for wound healing is a nice example. Jang et al. investigated gelatin methacrylate (GelMA) as a promising solution with customizable physical characteristics [43].
- High Loading/Release Patches: Precise drug release and high drug loading are required for long-acting transdermal drug administration. A novel pressure-sensitive adhesive (PSA) modified with hydroxyphenyl (HP) was created to improve drug-polymer miscibility and allow for controlled drug release [89]. The findings show that dual-ionic H- bonds between R(3)N and R(2)NH-type medications and HP-PSA are reversible and quite strong, in contrast to ionic and neutral H-bonds. This made it possible for patches to limit drug release rate by 1/5 to 1/2 while improving drug loading by 1.5–7 times, all without changing the release profile overall [44].
Transdermal patches may also be used for the following other purposes: Diseases That Are Infectious Hormonal Deficiencies, Transdermal Patches, and Contraception Transdermal Patches and Heart Conditions Stratum Transdermal, Gene Therapy Vaccination patches, transdermal patches [45].
Conclusions and Future Challenges
Transdermal patch technology related to Alzheimer disease is a valuable medication delivery system with several benefits over conventional methods of administration. Patches can avoid the digestive system and first-- pass metabolism, allowing for continuous medication dosage throughout time. It provides avoidance of gastro intestinal side effect that is specifically related to cholinesterase inhibitor. Many improvements in transdermal patch technology have occurred in recent years, including the Nano particle and microneedle based transdermal patch formulation that help to overcome the problem related to dose dumping. There is some resent advancement in transdermal patch manufacturing for the treatment of disease like diabetes. Transdermal patches have the potential to be a convenient and effective way of drug delivery for a number of conditions, but there are still some obstacles to overcome, like the risk of self-inflicted toxicity due to improper dosing, poor adhesion, low drug penetration, potential trigger for skin irritation, or patch failure. Therefore, we need to create smart, dissolving/biodegradable, high-loading/release, and 3D-printed patches. All of these point to the need for more study and development to raise the delivery technology's level of safety and effectiveness.
- Wong WF, Ang KP, Sethi G, Looi CY (2023a) Recent Advancement of Medical Patch for Transdermal Drug Delivery. In Medicina (Lithuania) 59: 4.
- Chien YW, Liu J (n.d.) Transdermal Drug Delivery Systems.
- Lasagna L, Greenblatt DJ (1986) More Than Skin Deep: Transdermal Drug-Delivery Systems. New England Journal of Medicine 314.
- Berner B, John VA (1994) Pharmacokinetic Characterisation of Transdermal Delivery Systems. In Clinical Pharmacokinetics 26: 2.
- Kearney MC, Caffarel-Salvador E, Fallows SJ, McCarthy HO, Donnelly RF (2016) Microneedle- mediated delivery of donepezil: Potential for improved treatment options in Alzheimer’s disease. European Journal of Pharmaceutics and Biopharmaceutics, 103: 43-50.
- Larkin HD (2022) First Donepezil Transdermal Patch Approved for Alzheimer Disease. JAMA, 327.
- Saluja S, Kasha PC, Paturi J, Anderson C, Morris R, Banga AK (2013) A novel electronic skin patch for delivery and pharmacokinetic evaluation of donepezil following transdermal iontophoresis. International Journal of Pharmaceutics, 453: 395-9.
- Kurz A, Farlow M, Lefèvre G (2009) Pharmacokinetics of a novel transdermal rivastigmine patch for the treatment of Alzheimer’s disease: A review. International Journal of Clinical Practice, 63: 799-805.
- Lefèvre G, Pommier F, Sȩdek G, Allison M, Huang HLA, Kiese B, Ho YY, Appel-Dingemanse S (2008) Pharmacokinetics and bioavailability of the novel rivastigmine transdermal patch versus rivastigmine oral solution in healthy elderly subjects. Journal of Clinical Pharmacology, 48.
- Cai Y, Tian Q, Liu C, Fang L (2021) Development of long-acting rivastigmine drug-in-adhesive patch utilizing ion-pair strategy and characterization of controlled release mechanism. European Journal of Pharmaceutical Sciences, 161.
- Woo FY, Basri M, Masoumi HRF, Ahmad MB, Ismail M (2015) Formulation optimization of galantamine hydrobromide loaded gel drug reservoirs in transdermal patch for Alzheimer’s disease. International Journal of Nanomedicine, 10: 3879-86.
- Farlow MR, Somogyi M (2011) Transdermal patches for the treatment of neurologic conditions in elderly patients: A review. In Primary Care Companion to the Journal of Clinical Psychiatry 13: 6.
- Fong Yen W, Basri M, Ahmad M, Ismail M (2015) Formulation and evaluation of galantamine gel as drug reservoir in transdermal patch delivery system. Scientific World Journal.
- Kumar A, Sudevan ST, Nair AS, Singh AK, Kumar S, Jose J et al. (2023) Current and Future Nano-Carrier-Based Approaches in the Treatment of Alzheimer’s Disease. In Brain Sciences 13: 2.
- Levy D, Glikfeld P, Grunfeld Y, Grunwald J, Kushnir M, Levy A et al. (1986) A Novel Transdermal Therapeutic System as a Potential Treatment for Alzheimer’s Disease.
- Bioavailability of Oral Physostigmine (1985) New England Journal of Medicine, 313.
- Bongoni Rn (2020) Formulation and Evaluation of Physostigmine-Transdermal Patch. World Journal of Current Medical and Pharmaceutical Research, 02.
- Guy RH, Kalia YN, Delgado-Charro MB, Merino V, López A, Marro D (2000) Iontophoresis: Electrorepulsion and electroosmosis. Journal of Controlled Release, 64: 1-3.
- Kanakagiri D, Chettupalli AK (2022) Development of a Transdermal Delivery System for Tacrine. South Asian Research Journal of Pharmaceutical Sciences, 4.
- Venkatraman S, Gale R (1998) Skin adhesives and skin adhesion. 1. Transdermal drug delivery systems. Biomaterials, 19.
- Nguyen TT, Giau V Van, Vo TK (2017) Current advances in transdermal delivery of drugs for Alzheimer’s disease. In Indian Journal of Pharmacology 49: 2.
- Jaskari T, Vuorio M, Kontturi K, Urtti A, Manzanares JA, Hirvonen J (2000) Controlled transdermal iontophoresis by ion-exchange fiber. Journal of Controlled Release, 67: 2-3.
- Khanmohammadi M, Elmizadeh H, Ghasemi K (2015) Investigation of size and morphology of chitosan nanoparticles used in drug delivery system employing chemometric technique. Iranian Journal of Pharmaceutical Research, 14.
- Heydorn WE (1997) Donepezil (E2020): A new acetylcholinesterase inhibitor. Review of its pharmacology, pharmacokinetics, and utility in the treatment of Alzheimer’s disease. In Expert Opinion on Investigational Drugs 6: 10
- Dinh L, Lee S, Abuzar SM, Park H, Hwang SJ (2022) Formulation, Preparation, Characterization, and Evaluation of Dicarboxylic Ionic Liquid Donepezil Transdermal Patches. Pharmaceutics, 14.
- Klein J (2007) Phenserine. Expert Opinion on Investigational Drugs, 16.
- Scott LJ, Goa KL (2000) Galantamine: A review of its use in Alzheimer’s disease. In Drugs 60: 5.
- Park CW, Son DD, Kim JY, Oh TO, Ha JM, Rhee YS, Park ES (2012) Investigation of formulation factors affecting in vitro and in vivo characteristics of a galantamine transdermal system. International Journal of Pharmaceutics, 436: 1-2
- Ameen D, Michniak-Kohn B (2019) Development and in vitro evaluation of pressure sensitive adhesive patch for the transdermal delivery of galantamine: Effect of penetration enhancers and crystallization inhibition. European Journal of Pharmaceutics and Biopharmaceutics, 139.
- McKeage, K. (2010). Spotlight on memantine in moderate to severe alzheimers disease. In Drugs and Aging 27: 2.
- Valeveti SK, Pashikanti S (2023) Design, Development, and Evaluation of Transdermal Patches Containing Memantine Hydrochloride. International Journal of Applied Pharmaceutics, 15.
- Qian ZM, Ke Y (2014) Huperzine A: Is it an effective disease-modifying drug for Alzheimer’s disease? In Frontiers in Aging Neuroscience 6.
- Ghosh P, Brogden NK, Stinchcomb AL (2013) Effect of formulation pH on transport of naltrexone species and pore closure in microneedle-enhanced transdermal drug delivery. Molecular Pharmaceutics, 10.
- Arora A, Prausnitz MR, Mitragotri S (2008) Micro-scale devices for transdermal drug delivery. In International Journal of Pharmaceutics 364: 2
- Tröls A, Hintermüller MA, Saeedipour M, Pirker S, Jakoby B (2019) Drug dosage for microneedle- based transdermal drug delivery systems utilizing evaporation-induced droplet transport. Microfluidics and Nanofluidics, 23.
- Lee BY, Bartsch SM, Mvundura M, Jarrahian C, Zapf KM, Marinan K et al, (2015) An economic model assessing the value of microneedle patch delivery of the seasonal influenza vaccine. Vaccine, 33.
- Azmana M, Mahmood S, Hilles AR, Mandal UK, Saeed Al-Japairai KA, Raman S (2020) Transdermal drug delivery system through polymeric microneedle: A recent update. In Journal of Drug Delivery Science and Technology 60.
- Aldawood FK, Andar A, Desai S (2021) A comprehensive review of microneedles: Types, materials, processes, characterizations and applications. In Polymers 13: 16.
- Olowe M, Parupelli SK, Desai S (2022) A Review of 3D-Printing of Microneedles. In Pharmaceutics 14: 12
- Poudel P, Park S (2022) Recent Advances in the Treatment of Alzheimer’s Disease Using Nanoparticle-Based Drug Delivery Systems. In Pharmaceutics 14: 4.
- Invernale MA, Tang BC, York RL, Le L, Hou DY, Anderson DG (2014) Microneedle Electrodes Toward an Amperometric Glucose-Sensing Smart Patch. Advanced Healthcare Materials 3.
- Rodgers AM, McCrudden MTC, Courtenay AJ, Kearney MC, Edwards KL et al. (2019) Control of Klebsiella pneumoniae Infection in Mice by Using Dissolving Microarray Patches Containing Gentamicin. Antimicrobial Agents and Chemotherapy 63.
- Jang MJ, Bae SK, Jung YS, Kim JC, Kim JS et al. (2021). Enhanced wound healing using a 3D printed VEGF-mimicking peptide incorporated hydrogel patch in a pig model. Biomedical Materials (Bristol), 16.
- Zhang S, Liu C, Song Y, Ruan J, Quan P, Fang L (2023) High drug-loading and controlled-release hydroxyphenyl-polyacrylate adhesive for transdermal patch. Journal of Controlled Release, 353.
- Wong WF, Ang KP, Sethi G, Looi CY (2023b) Recent Advancement of Medical Patch for Transdermal Drug Delivery. In Medicina (Lithuania) 59: 4.
- Robinson DM, Keating GM (2006) Memantine: A review of its use in Alzheimer’s disease. In Drugs 66: 11.
FIGURE 1
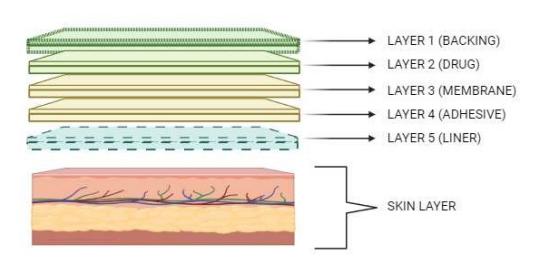
Figure 1: Basic Component of Transdermal Patch
FIGURE 2
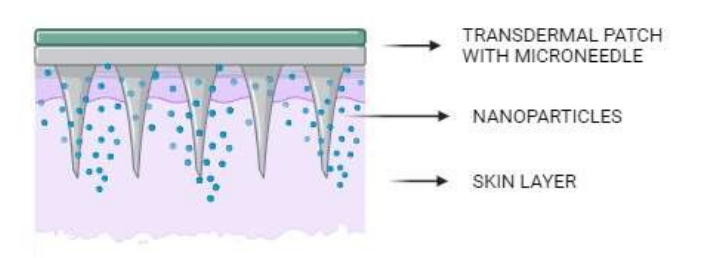
Figure 2: Microneedle-Based Patch
Tables at a glance
Figures at a glance