End Versus Observation in CT1-T2 Oral Tongue Squamous Cell Carcinoma – A Meta-Analysis of 11973 Patients
Received Date: July 03, 2020 Accepted Date: July 23, 2020 Published Date: July 27, 2020
doi: 10.17303/jocr.2020.1.101
Citation: Akheel Mohammad (2020) End Versus Observation in CT1-T2 Oral Tongue Squamous Cell Carcinoma – A Meta-Analysis of 11973 Patients. JJ Oncol Clin Res 1: 1-11.
Abstract
Introduction: The surgical management of the clinical negative neck node in early oral tongue squamous cell carcinoma(OTSCC)has been the topic of debate for a few decades. As the occult cervical lymph node metastasis is considered to be the prime prognostic factor in early OTSCC, this meta-analysis has been carried out to find the risk of regional nodal recurrence, disease-specific survival, and overall survival rates in the outcome of Elective neck dissection (END) versus patients under observation.
Materials & Methods: The articles were electronically retrieved from Ovid Medline, Pub Med, Cochrane, and Scholar for comparison of END versus Observation in early OTSCC. The search strategy identified 37 relevant review articles from April 1979 to April 2020 from different search engines. A total of 11,973 patients from 32 retrospective analysis, 4 prospective and 1 randomized control trials were included in this meta-analysis.
Results: Statistical analysis revealed Overall test (OR: 5.31 95% CI: -2.132- 14.698) with t-test 1.919 and p-value 0.113 which is not statistically significant but the readings say that there is always better Disease-specific survival with END patients rather than patients kept on observation. The overall test revealed (OR: 13.02 95% CI: 1.360- 17.154) with t-test 2.382 and p-value 0.023 which is statistically significant and showed that End significantly reduced the risk of regional nodal recurrence. The overall test revealed (OR: 7.93 95% CI: -15.461- 4.238) with t-test -1.347 and p-value 0.220 which is statistically insignificant and but showed that to some extent Overall survival improves in a patient with END than the patients kept on observation
Conclusion: This meta-analysis finds that there is a statistically significant relationship when Elective neck dissection was performed which reduced the risk of regional nodal recurrence. This analysis didn’t statically find any significance in Disease- specific survival and with END patients but however showed good prognosis when compared to patients kept under observation.
Introduction
Cancer is being recognized as the leading cause of morbidity and mortality after cardiovascular disease [1,2]. The most common type of oral cavity cancers are squamous cell carcinoma which constitutes approximately 90% of all cancers [3,4]. The most frequent sub-site of the lip oral cavity cancer is the tongue cancer [5]. The etiology of the oral cavity cancer is attributed to the use of tobacco and its related products, alcohol use, sedentary lifestyle, diet and nutrition, dental irritation, genetic factors & HPV infections [6]. Cervical nodal metastasis is considered as the most important prognostic factor which solely determines the survival and prognosis of patient [7,9,10,16]. It is estimated that the involvement of the lymph node in oral cavity cancers reduces the survival by 50% and the presence of extranodal extension further decreases the survival by 50% [8].
The management of the N0 neck in early tongue cancer has been the topic of discussion since the last three decades and is still a controversial topic. Surgery is the mainstay treatment of early-stage oral tongue squamous cell carcinoma (OTSCC).The decision while performing the surgery is whether to address the neck at the time of excision of the primary tumor or to observe the neck till clinical positive neck nodes. Various studies have been reported in literature favoring observation as well as Elective neck dissection (END). Neck dissection along with the excision of primary is thought to be benefitted in cases of subclinical occult metastasis [9]. The presence of a higher incidence of occult metastasis in cases of early oral cancers is approximately 16 to 36% [10-12]. The logic lies in the fact that the subclinical occult metastasis plays a pivotal role in the early OTSCC and considered to be the key factor for the loco-regional failure in the cases where the only resection of the primary tumor has been performed. Meanwhile, the quality of life is compromised in the END because of the invasiveness of neck surgery [13]. Whereas,in the “Wait & Watch” group, the observed neck is benefitted in a truly negative clinical neck as those patients experience less extensive surgery.
The aim of this study is to systematically review the current literature to (1) find disease-specific survival patients after END versus patients kept on observation (2) find the neck nodal recurrence in END patients and patients kept on Observation (3) find the overall survival rate in END patients and patients kept on observation.
Materials and Methods
The data collected for this study was performed accordingto PRISMA guidelines. Electronic searches were performed using Ovid Medline, PubMed, Cochrane, Scopus, and Scholar from 1970 to April 2020. Search terms used to achieve maximum data were: (“squamous cell carcinoma” OR “Cancer” OR “Carcinoma” OR “SCC”) AND (“Tongue” OR “oral tongue” OR “mobile tongue”) AND (“T1” OR“ T2” OR “early stage”) AND (“elective neck dissection” OR “END”, “neck dissection” OR “ no neck treatment” OR “observation” OR “ wait and watch” ) AND (“node-negative neck” OR “N0 neck”) as either terms or MeSH terms. The data obtained from the above search results were reviewed and the relevant articles were selected based on the inclusion and exclusion criteria of our study.
Inclusion criteria: The articles with full text in the English language were included in the study. Only early-stage cancer as T1, T2, and N0 neck are included in the study. Randomized trials and matched Studies including the elective neck dissection versus observation were included. All patients included should be pathologically proven as Squamous cell carcinoma of the tongue without any clinically apparent lymphadenopathy or distant metastasis at the time of diagnosis. Exclusion criteria: T3 and T4 lesions of the tongue, medically compromised patients, the patient completed radiation therapy prior to surgery.
Data extraction
There were 2 reviewers in this study to discuss any difference in opinion. The first reviewer extracted all the data from the published articles. The information collected was the type of study design, year, patient characteristics (age and sex), country and period, tumor stage distribution, data on END versus observation, follow up period, and the outcome of the articles.All this information was reviewed by the second reviewer. Three parameters were chosen as endpoints for the systemic review and meta-analysis: occult cervical lymph node metastasis, neck nodal recurrence, and overall survival rate. (Table 1) shows the demographic table with a total of 37 articles was included in the study with 11,973 patients with all the data collected.
Statistics
To evaluate the heterogeneity of studies, the chi-square test (x2 ) was done. The level of significance was determined for heterogeneity at p=0.05. I2 value determined the percentage of variation across the studies. Values < 50% show less variability. For comparison between two parameters end and observed values, the t-test was applied and the level of significance was determined, along with confidence interval at 95% level.
Results
The search strategy identified 37 relevant review articles from April 1979 to April 2020 from different search engines. A total of 11,973 patients from 32 retrospective analysis, 4 prospective and 1 randomized control trials were included in this meta-analysis.
Out of 37articles, 11 articles (Table 2) were included in the meta-analysis to find Disease-specific survival for Elective neck dissection patients versus Observation. The HR test revealed that X2 IS 30.0, I2 is 42% with p-value 0.224. The overall test revealed (OR: 5.31 95% CI: -2.132- 14.698) with t-test 1.919 and p-value 0.113 which is not statistically significant but the readings say that there is always better Disease-specific survival with END patients rather than patients kept on observation (Figure 1).
All the 37 articles with 11,973 patients (Table 3) were included in the meta-analysis to find the nodal recurrence in END patients versus patients kept on observation. The HR test revealed that X2 IS 394.917, I2 is 40% with p-value 0.506. The overall test revealed (OR: 13.02 95% CI: 1.360- 17.154) with t-test 2.382 and p-value 0.023 which is statistically significant and nodal recurrence (Figure 2). Out of 37 articles, 16 articles (Table4) were included in the meta-analysis to find the overall survival in END patients versus patients kept on observation. The HR test revealed that X2 is 56, I2 is 43% with p-value 0.229. The overall test revealed (OR: 7.93 95% CI: -15.461- 4.238) with t-test-1.347 and p-value 0.220 which is statistically insignificant and but showed that to some extent Overall survival improves in a patient with END than the patients kept on observation. (Figure3).
Discussion
OTSCC is a challenging entity when compared to other subsites of the oral cavity because of its unpredictable nature of lymphatic involvement. The lymphatic spread of the OTSCC can be sub-clinical at the time of diagnosis and it can be presented unilateral or bilateral Involvement. The lymph node metastasis depends on various factors such as tumor growth type, size, differentiation, mode of Invasion, the pattern of Invasion, tumor thickness, histological grading, and stagin G [14,15]. All available preoperative and pre-surgical assessments that includes clinical neck examination by palpation and various imaging modalities like computed tomography (CT scan), magnetic resonance imaging (MRI scan), positron emission tomography–computed tomography (PET-CT scan), and ultrasonography) cannot justify the role of END as an accurate diagnostic procedure to stage the N0 neck clinically. Radiologic investigation modalities currently available have sensitivity ranging from 70 to 80% and have shown some improvements in the detection of neck nodal metastasis. Therefore, END may help in defining the status of the neck, removing subclinical or occult metastasis and determining the need for postoperative adjuvant therapy. It is clear that the incidence of delayed nodal metastases and recurrence will be comparatively higher if the nodal status was staged only by clinical palpation compared with staging by advanced imaging techniques.
The prime etiology of treatment failure and poor prognosis in early OTSCC is neck nodal recurrence [18]. According to various studies, it has been concluded that the recurrence rate of cervical lymph nodes is higher in tongue compared to other sub-site, because of the rich vascular supply, lymphatic drainage and frequent mechanical movement of the tongue [19,20]. After reviewing the literature the chances of neck node recurrence are less in END when compared with the observation. Yuen, etal. (2009) have concluded that elective neck dissection has significantly reduced neck nodal recurrence [15-17]. A study was carried out by Tsang et al suggesting that END is suitable for T2 lesions of tongue and patients kept under wait and watch policy was only considered when the tumor thickness is less than 4mm,G2 grading, and patients are ready to be in close follow up [21]. The concept of Elective neck dissection in early-stage OTSCC is followed worldwide and has gained popularity because of the increased rate of nodal recurrence in cases of the observed neck.Although, END gives more morbidity such as shoulder dysfunction, neck pain, and keloids. The disadvantage of END occurs in the case of true N0 neck which comprises approximately 70% has to undergo morbidity to prevent neck node recurrence. The benefit of observation over END is that the patients with truly subclinical nodal metastasis (30-40%) have to undergo surgery but with an increased risk of morbidity [17]. Wong. et al, described the effectiveness of salvage surgery in neck nodal recurrence to be only moderately effectively with 32% of 5-year survival rate [22]. In cases of cervical metastasis, early diagnosis and management is of utmost importance, as in delayed cases the risk of extra capsular spread and multiple involvements of nodes is increased.So, it can be said that the reduced survival rate could be seen in cases of observation group [23]. Van den Berkel et al,showed that the occurrence of the neck nodal recurrence arises in less than 18 months after the first treatment. He suggested that the reason to neck nodal recurrence is the previous presence of micro-metastasis of the lymph node which went undetected clinically. With the improvement in the technology, USG-guided FNAC has high positive and negative predictive values which are proved to be better diagnostic aids in detecting the lymph node metastasis [23]. Similarly, Sentinel lymph node biopsy is also considered to be an alternative for detecting nodal metastasis [25]. A study carried out on 10 patients with early OTSCC by Sagheb et al, comparing the histopathological findings from END group to the SLNB specimen. His results showed the sensitivity and specificity rates of 75% and 100% respectively [26]. Many surgeons believe that SLNB is an alternative option for END. In present meta-analysis p-value 0.023 which is statistically significant and showed that END significantly reduced the risk of regional nodal recurrence.-
In our study, we have calculated the overall survival rate of patients undergoing END and kept under observation.Our meta-analysis shows p-value 0.220 which is statistically insignificant and but showed that to some extent Overall survival improves in patients with END than the patients kept on observation. The overall survival rate is stated as a five-year survival rate, which is the percentage of people in a study or treatment group who are alive 5 years after their diagnosis. D’Cruz and his colleagues conducted a randomized trial in 2015 comparing the rates of overall survival and disease-free survival of END versus therapeutic neck dissection in node-negative oral cancer patients. His study included 596 patients of oral cavity cancer with a maximum of 85.3% cases of tongue cancer. He suggested that END showed a significantly better overall survival rate by 12.5%. They also reported more advanced nodal disease in cases of observed neck cases [27]. Ren et al, conducted a meta-analysis comparing the results END and observation with therapeutic neck dissection for nodal repalse including 5 randomized trials.4 studies had reported on Overall survival rate. The result showed higher OS in the END group as compared to observation with a significant inter-group difference [28]. In a meta-analysis done by Abu Ghanem et al, he demonstrated less recurrence and better disease-specific survival rate in the END group compared to observation. However, they reported no significant improvement in overall survival rates [16]. Keski- Santti et al, in his study, included 80 patients of early OTSCC with clinically N0 neck demonstrated that there is no significant improvement in the overall survival rate and disease-free survival rate after undergoing END [29]. In the study of Kligerman, he showed better 3-year survival rates from 49% to 72% in END group [23]. In 2006, Yu et al reported a 100% 5-year survival rate in the END group whereas only 68.7% in patients kept under observation [30]. Yuen et al, (2009) achieved an 89% survival rate after END and 87% survival rate in the observation group which is insignificant [17]. Fakih et al, also reported an insignificant difference in overall survival rate between the hemiglossectomy group and hemiglossectomy and radical neck dissection group [31].
In our study, we also found that p-value 0.113 which is not statistically significant but the readings say that there is always better Disease-specific survival (DSS) with END patients rather than patients kept on observation. There are many studies done in literature, the one from Yookyeong Carolyn Sim et al,[32] concluded that the survival rate is lower in poor-grade or advanced TNM stages. In their study, patients with stage I and II disease showed DSS of 100%. It could be concluded that early-stage OSCC is curable, and therefore early detection is critical.
This meta-analysis finds that there is a statistically significant relationship when the END was performed which reduced the risk of regional nodal recurrence. This analysis dint statically finds any significance in DSS and OS with Elective neck dissection patients rather than patients kept on observation but however showed good prognosis when END was performed.
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A (2018) Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians 68: 394-424.
- Global Health Estimates 2016: Deaths by Cause, Age,Sex, by Country and by Region, 2000-2016. Geneva, World Health Organization; 2018; Human Development Report 2016.New York, United Nations Development Programme.
- Bagan J, Sarrion G, Jimenez Y (2010) Oral cancer: clinical features. Oral Oncol 46: 414-417.
- Ow TJ, Myers JN (2011) Current management of advanced resectable oral cavity squamous cell carcinoma. Clin Exp Otorhinolaryngol 4:1-10.
- Funk GF, Karnell LH, Robinson RA, Zhen WK, et al.(2002) Presentation, treatment, and outcome of oral cavity cancer: a National Cancer Data Base report. Head Neck 24: 16580.
- Kumar M, Nanavati R, Modi TG, Dobariya C (2016) Oral cancer: Etiology and risk factors: A review. J Can Res Ther 12: 458-463.
- Ferlito A, Silver CE, Rinaldo A (2007) Neck dissection in the new era. J Am CollSurg 204: 466–468.
- Amin MB, Edge S, Greene F, et al. (2017) editors. AJCC cancer staging manual. 8th ed. Springer International Publishing.
- D’Cruz AK, Siddachari RC (2004) WalvekarEur Arch Otorhinolaryngol 261: 295303. RR, et al. Elective neck dissection for the management of the N0 neck in early cancer of the oral tongue: the need for a randomized controlled trial. Head Neck 2009; 31: 618-24.
- Dik EA, Willems SM, Ipenburg NA, et al. (2016) Watchful waiting of the neck in early-stage oral cancer is unfavorable for patients with occult nodal disease. Int J Oral Maxillofac Surg 45: 945.
- El-Naaj IA, Leiser Y, Shveis M, et al. (2011) Incidence of oral cancer occult metastasis and survival of T1-T2N0 oral cancer patients. J Oral Maxillofac Surg 69: 2674.
- Lim YC, Lee JS, Koo BS, et al. (2006) Treatment of contra lateral N0 neck in early squamous cell carcinoma of the oral tongue: Elective neck dissection versus observation. Laryngoscope 116: 461.
- Spalthoff S, Zimmerer R, Jehn P, et al. (2017) Neck dissection’s burden on the patient: Functional and psychosocial aspects in 1,652 patients with oral squamous cell carcinomas. J Oral Maxillofac Surg 75: 839.
- Kurokawa H, Yamashita Y, Takeda S, Zhang M, Fukuyama H, Takahashi T (2002) Risk factors for late cervical lymph node metastases in patients with stage I or II carcinoma of the tongue. Head Neck 24: 731–736.
- Akoğlu E, Dutipek M, Bekiş R, Değirmenci B, Ada E,Güneri A (2005) Assessment of cervical lymph node metastasis with different imaging methods in patients with head and neck squamous cell carcinoma. J Otolaryngol 34.
- Abu-Ghanem S, Yehuda M, Carmel NN, et al. (2016) Elective neck dissection vs observation in early-stage squamous cell carcinoma of the oral tongue with no clinically apparent lymph node metastasis in the neck: A systematic review and meta-Analysis. JAMA Otolaryngol Head Neck Surg 142: 857.
- Yuen AP, et al. (2009) Prospective randomized study of selective neck dissection versus observation for N0 neck of early tongue carcinoma. Head Neck 31: 765-772.
- Amin MB, Edge S, Greene F, et al. (2017) editors. AJCC cancer staging manual. 8th ed. Springer International Publishing.
- Dias FL, Kligerman J, Matos de Sá G, et al. (2001) Elective neck dissection versus observation in stage I squamous cell carcinomas of the tongue and floor of the mouth. Otolaryngology head and neck surgery: official journal of American Academy of Otolaryngology-Head and Neck Surgery 125: 23-29.
- Flach GB, Tenhagen M, De Bree R, et al. (2013) The outcome of patients with early-stage oral cancer managed by an observation strategy towards the N0 neck using ultrasoundguided fine-needle aspiration cytology: No survival difference as compared to elective neck dissection. Oral oncology 49: 157-164.
- Tsang RK, Chung JC, To VS, Chan JY, Ho WK, Wei WI (2011) Efficacy of salvage neck dissection for isolated nodal recurrences in early carcinoma of oral tongue with watchful waiting management of initial N0 neck. Head and Neck 33: 1482-1485.
- Wong LY, Wei WI, Lam LK, Yuen AP (2003) Salvage of recurrent head and neck squamous cell carcinoma after primary curative surgery. Head and Neck 25: 953–959.
- Kligerman J, Lima RA, Soares JR, Prado L, Dias FL,Freitas EQ, et al. (1994) Supraomohyoid neck dissection in the treatment of T1/T2 squamous cell carcinoma of the oral cavity.Am J Surg 168: 391-394.
- De Bree R, vandenBrekel MW (2015) Elective neck dissection versus observation in the clinically node-negative neck in early oral cancer: Do we have the answer yet? Oral Oncol 51:963-965.
- Melkane AE, Mamelle G, Wycisk G, Temam S, Janot F (2012) Sentinel node biopsy in early oral squamous cell carcinomas: a 10-year experience. Laryngoscope 122: 1782-1788.
- Sagheb K, Sagheb K, Rahimi-Nedjat R, Taylor K, Al-Nawas B, Walter C (2016) Sentinel lymph node biopsy in T1/T2 squamous cell carcinomas of the tongue: A prospective study.Oncol Lett. 11: 600-604.
- D'Cruz AK, Vaish R, Kapre N, et al. (2015) Elective versus Therapeutic Neck Dissection in Node-Negative Oral Cancer.N Engl J Med. 373: 5219.
- Ren ZH, Xu JL, Li B, Fan TF, Ji T, Zhang CP (2015) Elective versus therapeutic neck dissection in node-negative oral cancer: Evidence from five randomized controlled trials. Oral oncology 51: 976-981.
- Keski-Säntti H, Atula T, Törnwall J, Koivunen P, Mäkitie A (2006) Elective neck treatment versus observation in patients with T1/T2 N0 squamous cell carcinoma of oral tongue. Oral Oncol 42: 96101.
- Yu S, Li J, Li Z, Zhang W, Zhao J (2006) Efficacy of supraomohyoid neck dissection in patients with oral squamous cell carcinoma and negative neck. Am J Surg 191: 94–99.
- Fakih AR, Rao RS, Borges AM, Patel AR (1989) Elective versus therapeutic neck dissection in early carcinoma of the oral tongue. Am J Surg 158: 309-313.
- Sim YC, Hwang JH, Ahn KM (2019) Overall and disease- specific survival outcomes following primary surgery for oral squamous cell carcinoma: analysis of consecutive 67 patients. Journal of the Korean Association of Oral and Maxillofacial Surgeons. 45: 83-90.
Tablel 1
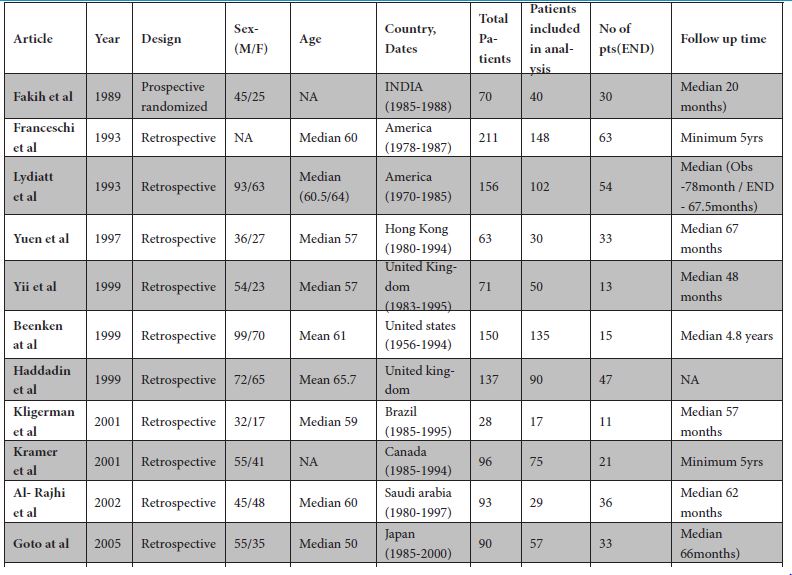
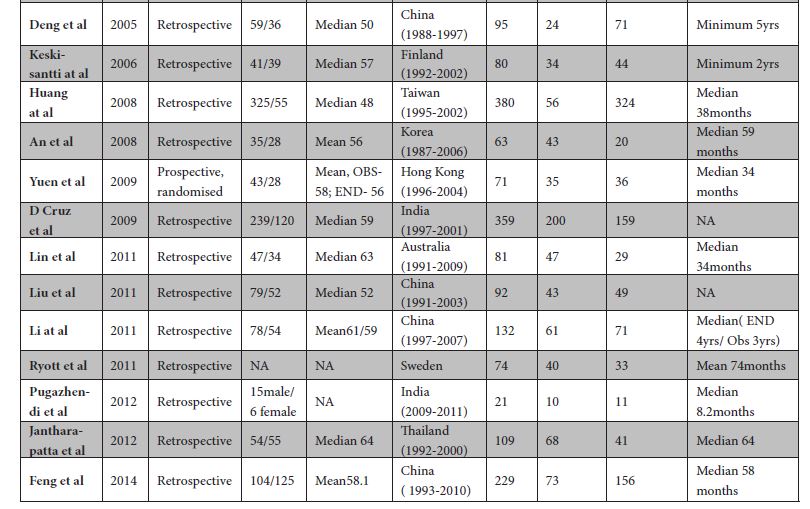
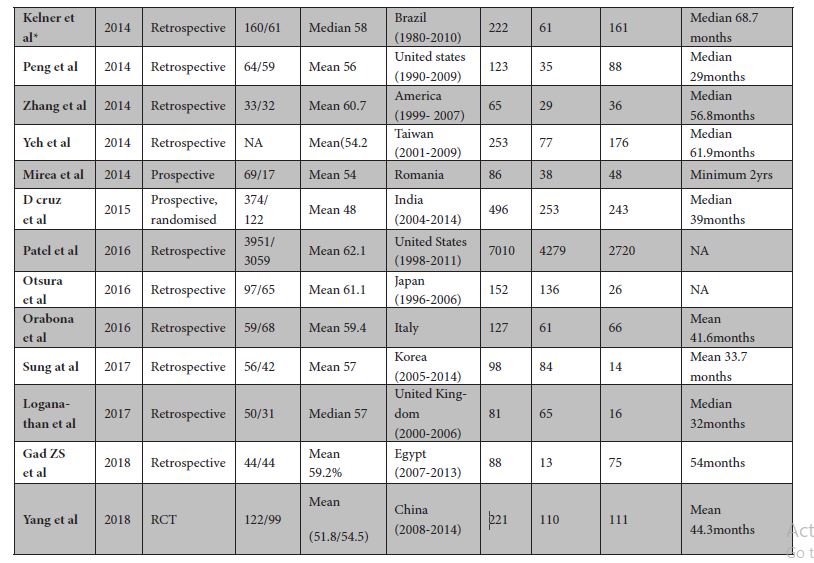
Table 1: Demographic
Table 2
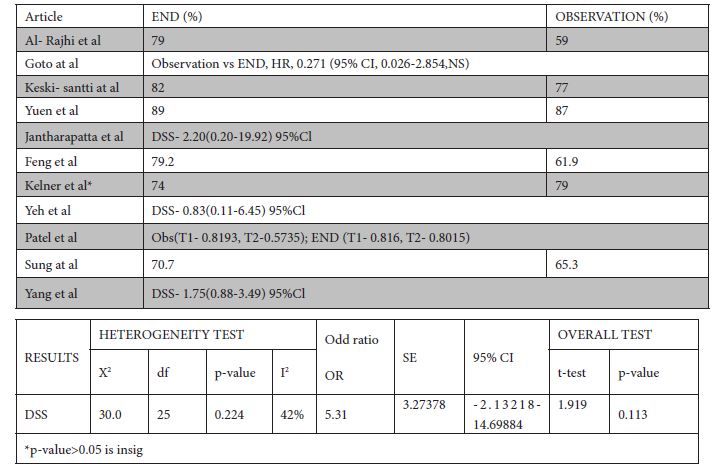
Table 2: Disease specific survival for END versus patients kept on observation.
Table 3
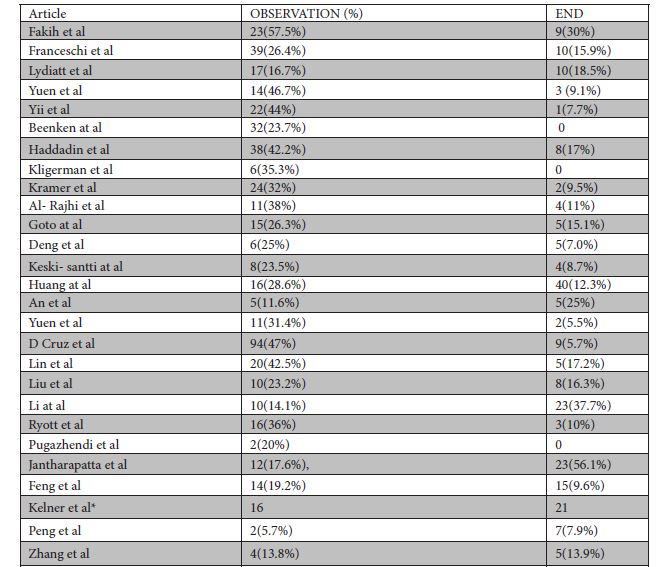
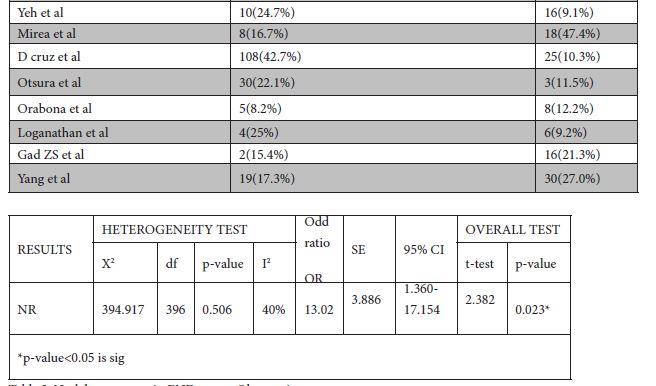
Table 3: Nodal recurrence in END versus Observation
Table 4
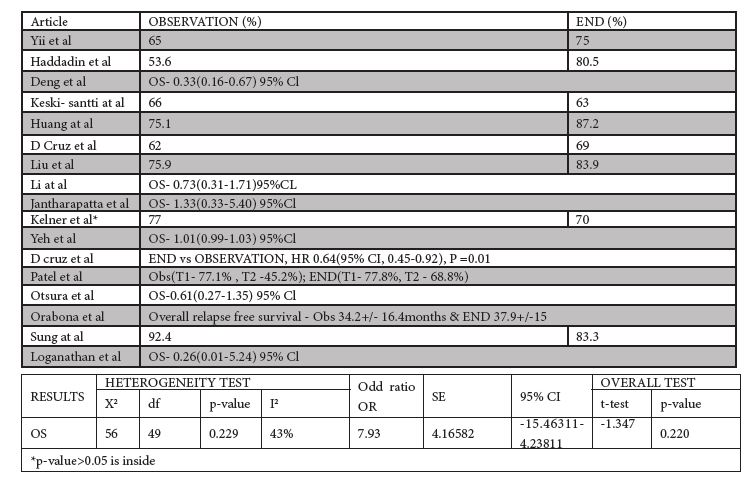
Table 4: Overall Survival for END and observation
FIGURE 1
Figure 1: Tabulation of HR of all 11 articles to find Disease-specific survival for END versus patients kept on observation.
FIGURE 2
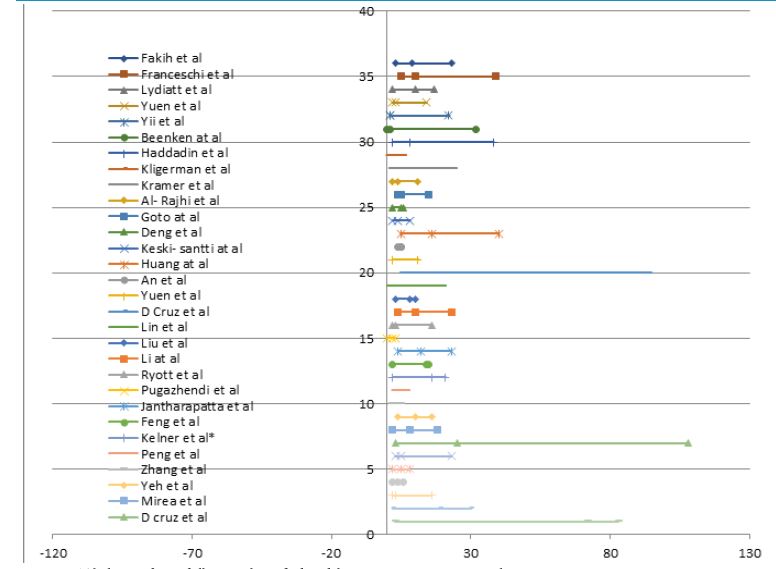
Figure 2: Tabulation of HR of all 37 articles to find Nodal recurrence in END versus Observation
FIGURE 3
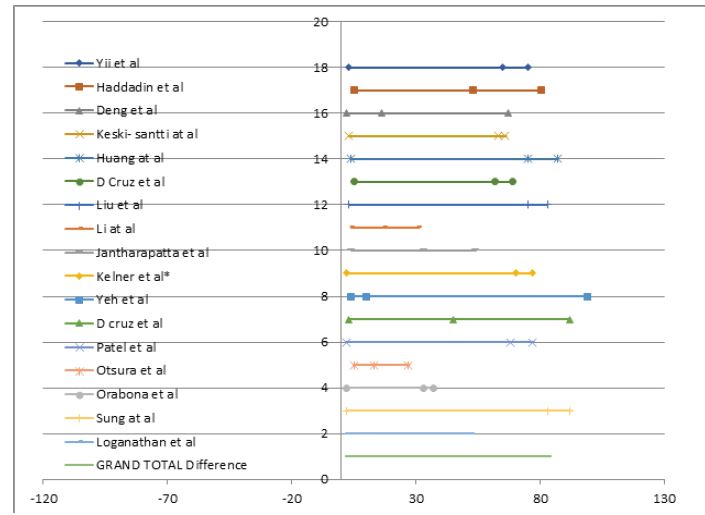
Figure 3: Tabulation of HR of all the 16 articles to find Overall Survival for END and observation
Tables at a glance
Figures at a glance