Dynamic Risk Assessment of Second Primary Malignancy Among Childhood and Adolescent Cancer Survivors
Received Date: March 08, 2021 Accepted Date: August 01, 2021 Published Date: August 03, 2021
doi: 10.17303/jocr.2021.2.102
Citation: Kaibin Yang (2021) Dynamic Risk Assessment of Second Primary Malignancy Among Childhood and Adolescent Cancer Survivors. JJ Oncol Clin Res 1: 1-14
Abstract
Background: Second primary malignancy (SPM) is the most severe treatment-related late effect in childhood and adolescent cancer survivors (CACS). Despite that the risk of SPM changes dynamically, limited data exist regarding risk assessment of SPM in CACS at different periods of follow-up that may provide valuable guidance for more efficient screening of SPM among CACS.
Methods: All CACS meeting the following criteria in SEER database were included: their primary malignancies (PM) were diagnosed between January 1975 and December 2015; age at PM diagnosis was ≤ 21 years old; survival time was >12 months. The relative risk of SPM was measured by standardized incidence ratio (SIR). The SIR and prognosis of SPM at different periods of follow-up was compared. The most common SPM subtypes and risk factors of SPM at different follow-up periods were explored.
Results: 49006 CACS were included in our study. 1819 of them developed SPM. The SIR of SPM in CACS was 3.10, larger than all the other groups. And it constantly decreased as the follow-up time and attained age increased. No significant disparities were detected in the overall survival of SPM detected at different periods of follow-up. Non-lymphocytic leukemia accounted for the largest proportion at the first 10 years of follow-up, while breast cancer accounted for the largest proportion at 11-20 (20%), 21-30 (23.87%) and 31+ years (17.99%) of follow-up consistently. The proportion of non-lymphocytic leukemia and brain tumors decreased while the proportion of lung cancer and colorectal cancer gradually increased as the follow-up time increased. The risk factors of SPM in CACS at different periods of follow-up were also identified to guide more precise screening of SPM in CACS.
Conclusions: More attention should be paid to surveillance of SPM in CACS, especially at the first 10 year after the primary malignancy. Specific SPM and specific population should be surveilled and prevented closely in CACS at specific period of follow-up.
Keywords: Second Primary Malignancy; Childhood and Adolescent Cancer Survivors; Risk; Risk Factors; Prognosis
Introduction
Over the past few decades, more than 80% of children and adolescents with cancer achieved long-term survival owing to advances in pediatric oncology in developed countries [1-3]. However, according to a report from Childhood Cancer Survivor Study cohort, up to 62.3% of survivors develop at least one treatment-associated life-threatening disease in their adulthood, which seriously affects their quality of life [4,5]. Second primary malignancy (SPM) is one of the most severe negative outcomes of cancer treatment that contributes to 18.5% of all causes of death in childhood and adolescent cancer survivors (CACS) within 30 years after diagnosis[6,7].
SPM is mainly induced by anti-cancer therapy[8]. Radiotherapy and some chemotherapeutics (e.g., alkylating agents and topoisomerase inhibitors) have been confirmed to be associated with SPM [9,10]. Theoretically, children and adolescents are more vulnerable to the side effects of these treatments owing to their immature organ functions and rapidly growing body [11]. Previous studies have shown that the risk of SPM in CACS ranges from 3.3-11.2 times higher than that of the general population[12-15], and it was reported that relative risks of SPM in CACS decreased with attained age[10,12,13,16]. Considering that the risk of SPM in CACS is high and changes dynamically, evaluating the risk, spectrum, and risk factors of SPM in CACS at different periods of follow-up dynamically may provide valuable guidance for more efficient screening of SPM among CACS. However, limited data exist regarding risk assessment of SPM in CACS at different periods of follow-up to our best knowledge.
Due to the low incidence rate of cancer in children and adolescents, it is of great difficulties to obtain a CACS cohort with enough sample size and follow-up time for research about SPM in CACS. Surveillance, Epidemiology, and End Results (SEER) is a large population-based database covering approximately 34.6% of the general population in the United State of America[17]. With detailed follow-up data and large sample size, SEER database provides valuable resources for research about SPM in CACS.
Thus, the risk, prognosis, spectrum, and risk factors of SPM in CACS at different periods of follow-up was explored using the SEER database in this study. Demonstrating the dynamic change of SPM in CACS in detail, this study may help clinicians to identify CACS at high risk of SPM and tell them which subtype of SPM should be especially prevented and surveilled at different periods of follow-up. Thus, our work fills the gap of the previous studies to informs dynamic surveillance guidelines for SPM in CACS.
Methods
Study Population
Our study population comprised all the CACS meeting the following inclusion and exclusion criteria from the SEER database. To ensure that the follow-up time was long enough for analysis, only patients from 9 (Connecticut, Detroit, Atlanta, San Francisco-Oakland, Hawaii, Iowa, New Mexico, Seattle-Puget Sound, and Utah) of the 21 registries in the SEER database were included. The inclusion criteria were: their primary malignancies (PM) were diagnosed between January 1975 and December 2015; age at PM diagnosis was ≤ 21 years old; survival time was >12 months. The exclusion criteria were: being a patient with unknown race; observing PM during autopsy; the diagnosis of PM recorded as “Miscellaneous”; and being a patient with SPM detected within one year after the diagnosis of PM (i.e., in order to avoid patients that could have had multiple primary tumors). The follow-up was considered to begin at one year after the diagnosis of PM for convenience. The SEER data are anonymized and publicly available, so there was no need to seek institutional ethics committee’s approval and consent from the participants for this study.
Study Variables
Common variables found in the SEER database were analyzed, including age at PM diagnosis, gender, race, and treatment-related variables. The race was stratified into 3 groups: white, black and others (including American Indian, AK Native, Asian and Pacific Islander). According to the age at PM diagnosis, the CACS were stratified into 2 groups: childhood cancer survivors (<14 years old) and adolescent cancer survivors (14~21 years old). The PM was divided into two groups: Solid and hematologic tumors. Treatment-related variables included surgery, radiotherapy, and chemotherapy.
Statistical Analysis
All statistical analyses were performed using the R software 3.6.3. Categorical variables were described by frequency and percentage and compared using the Pearson chi-square test; continuous variables were described by mean and standard deviation and compared using the Kruskal-Wallis rank sum test. In all analyses, differences were considered to be statistically significant at a two-sided P-value of 0.05.
The relative risk of patients suffering from the first SPM compared with the general population was measured by the standardized incidence ratio (SIR) obtained through the MP-SIR Session of SEER*Stat software, which was defined as the ratio of the number of SPM cases actually observed to the expected number of cancer cases in the matched standard population extracted from SEER database. The SIR of SPM at different periods of follow-up was compared to explore the trend of the relative risk of SPM during the follow-up period. Selected types of PM including germ cell tumors and acute lymphoblastic leukemia, and representative types of SPM including soft tissue tumor, testicular cancer, breast cancer, and leukemia were chosen to validate this trend at the level of single type of PM or SPM owing to relatively large numbers of these cases in the SEER database. To compare the trend of SIR of SPM in CACS to non-CACS’s, cancer survivors whose PM were diagnosed after 22 years old and met the inclusion and exclusion criteria above were also included in the SIR analysis and stratified into 3 groups: Group22-39 (22-39 years old), Group40-64 (40-64 years old), and Group65+(>65 years old). In CACS, the trend of the SIR of SPM at different attained ages was also investigated. The difference in standardized incidence ratio (SIR) was considered statistically significant when the 95% confidence interval (CI) was not intersected.
The overall survival (OS) rates of SPM diagnosed at different periods of follow-up were analyzed with the Kaplan-Meier method and compared using the log-rank test. Patients with the SPM detected in autopsy were excluded in the survival analysis due to the lack of the follow-up data.
To point out the most common subtypes of SPM at different periods of follow-up, the proportions of subtypes of SPM regarding different periods of follow-up since the PM diagnosis were obtained, and the top 15 of them were presented in wind rose diagrams.
Competing risk arises under the circumstance that there are more than one possible outcome and one can prevent the occurrence of the others. Since the presence of competing risk, the traditional Cox multivariate regression might lead to bias[18]. Therefore, proportional sub-distribution hazards regression was conducted to analyze the risk factors of SPM at different periods of follow-up[19]. Age, sex, race, and treatment-related variables were included in the regression models. The subdistribution hazard ratios (sHRs) and their 95% CI corresponding to the risk factors were estimated. The models of different time periods were fitting with the crprep function from the mstate package and the coxph function from survival package [20].
Results
Population characteristic and SPM incidence
In total, 49006 CACS met our including criteria. Demographic and clinical characteristics of CACS with and without SPM were displayed in Table 1. Compared with those without SPM, higher proportions of CACS with SPM were adolescent cancer survivors, female, diagnosed with hematopoietic PM, receiving radiotherapy and not receiving chemotherapy for their PM.
Additionally, 196438, 1221241 and 1319919 PM survivors in Group22-39, Group40-64, and Group65+ were also included for the comparison of the trend of SIR of SPM between CACS with non-CACS’s. Their demographic and clinical characteristics by age group were presented in Supplementary Table 1.
Among these PM survivors, 1819, 16410, 165962 and 183803 SPM cases were identified in CACS, Group22-39, Group40-64 and Group65+, respectively. The cumulative incidence rates, SIR, and latency of SPM in different age groups were presented in Table 2. The SIR of SPM in CACS was 3.10, larger than all the other groups. Among all groups, the longest latency between the diagnoses of PM and SPM was observed in CACS, with a median latency of 15.50 years (1.00-41.25 years). The median latencies in Group22-39, Group40-64 and Group65+ were 13.50 years, 8.67 years, and 5.25 years, respectively.
Risk and Prognosis of SPM at Different Periods of Follow-up
In survivors of various types of PM, the SIR of SPM constantly decreased as the follow-up time increased in CACS; notwithstanding, this trend was not as obvious in other age groups, particularly Group40-64 and Group65+ (Figure 1). Similar findings were also observed in the SIR of representative types of SPM in CACS (Supplementary Figure 1). Moreover, the SIR of SPM also decreased as the attain age increased in CACS (Supplementary Figure 2).
Besides the risk of SPM, the prognosis of SPM occurred at different periods of follow-up was also investigated. For both solid and hematologic SPM, no significant disparities were detected in the OS of SPM occurred at different periods of follow-up (Figure 2).
Spectrum of SPM at Different Periods of Follow-up
The top 15 SPM in CACS at 1-10, 11-20, 21-30 and 30+ years of follow-up were presented in wind rose diagrams (Figure 3). At 1-10 years of follow-up, non-lymphocytic leukemia accounted for the largest proportion (17.54%). Notably, the proportion of non-lymphocytic leukemia declined massively after the first 10 years of follow-up, which reached 1.73% at the second 10 years and dropped out of the top 15 afterwards. Whereas, the reduction in the proportion of brain tumors was gradual—at the 4 periods of follow-up, the proportion was 11.39%, 8.27%, 6.53% and 4.76%, respectively. Breast cancer accounted for the largest proportion at 11-20 (20%), 21-30 (23.87%) and 31+ years (17.99%) of follow-up consistently. The ranking of top 4 SPM at 11-20 years of follow-up was consistent with that at 21-30 years of follow-up. Remarkably, the proportion of lung cancer and colorectal cancer increased gradually as the follow-up time increased. At the first 10 years, lung cancer and colorectal cancer were out of the top 15 SPM; at the second 10 years, lung cancer ranked 13th (1.92%) and colorectal cancer ranked 8th (3.46%); at the third 10 years, lung cancer ranked 6th (4.5%) and colorectal cancer ranked 5th (4.95%); afterwards, lung cancer rose to No.2 (9.52%) and colorectal cancer rose to No.3 (8.99%). And the rankings of melanoma and thyroid cancer remained relatively stable at each period of follow-up.
Risk Factors of SPM at Different Periods of Follow up
Proportional sub-distribution hazards regression models were adopted to determine the risk factors of SPM in CACS at 1-10, 11-20, 21-30 and 31+ years of follow-up, respectively. As shown in Figure 4, at all periods of follow-up, being childhood cancer survivors was a protective factor for the occurrence of SPM in CACS with HR ranging from 0.555 to 0.735; and male CACS were less likely to be diagnosed with SPM with HR ranging from 0.508 to 0.654. Black race was a protective factor at 1-10 years (HR: 0.729; 95% CI: 0.623-0.854; P<0.001) and 11-20 years (HR: 0.757; 95% CI: 0.617-0.928; P=0.007) but not at other periods of follow-up. However, other race was a risk factor at 31+ years (HR: 2.136; 95% CI: 1.284-3.555; P=0.003) but not at other periods of follow-up. Receiving surgery was associated with higher likelihood of SPM only at 1-10 years (HR: 1.738; 95% CI: 1.518-1.989; P<0.001) and 11-20 years (HR: 1.241; 95% CI: 1.049-1.468; P=0.012) but not 21-30 and 31+ years of follow-up. Receiving radiotherapy was risk factor at 1-10 years (HR: 1.198; 95% CI: 1.092-1.315; P<0.001), 11-20 years (HR: 1.334; 95% CI: 1.187-1.498; P<0.001) and 21-30 years (HR: 1.182; 95% CI: 1.006-1.388; P=0.042) but not 31+ years of follow-up. Notably, receiving chemotherapy was a protective factor at 1-10 years (HR: 0.483; 95% CI: 0.435-0.537; P<0.001) but a risk factor at 11-20 years (HR: 1.150; 95% CI: 1.005-1.315; P=0.042) and 21-30 years (HR: 1.266; 95% CI: 1.052-1.523; P=0.013) of follow-up. In addition, the CACS with PM as hematopoietic tumors have higher odds of SPM at 1-10 years (HR: 2.135; 95% CI: 1.865-2.445; P<0.001), 11-20 years (HR: 1.597; 95% CI: 1.341-1.904; P<0.001) and 21-30 years (HR: 1.414; 95% CI: 1.112-1.799; P=0.005) but not 31+ years of follow-up.
Discussion
To provide theoretical basis for clinical guidelines for prevention and screening of SPM in CACS, we evaluated the risk and prognosis of SPM, and explored spectrum and risk factors of SPM dynamically at different periods of follow-up in our study. Suggesting which subtype of SPM in CACS and CACS with what characteristics should be especially surveilled at specific period of follow-up, our work gives guidance for the dynamic screening of SPM in CACS.
At whole period of follow-up, the SIR of SPM in CACS was 3.10, which indicated that the CACS develop another primary cancer 3.10-fold frequently compared with the reference population. The risk of SPM in CACS was also remarkably higher than that in other age groups. There are some possible mechanisms. First, young survivors tolerate anti-cancer therapy better, enabling them to receive more intensive anti-cancer therapy than adults[21]. Moreover, young survivors are more susceptible to carcinogenic factors owing to their rapidly growing bodies[11]. All aforementioned factors may lead to an increased risk of SPM in CACS.
Comparing the SIR of SPM at different periods of follow-up, we observed that SIR decreased as follow-up time increases among CACS. In addition, SIR of SPM in CACS also decreased with increasing attained age, which was consistent with the results of previous studies[10, 12, 13, 16]. These findings combinedly suggests that as survivors age, their relative risk of developing SPM reduced. Given that no significant disparities were detected in the OS of SPM at different periods of follow-up, indicating that the burden of SPM is mainly determined by its incidence, it is of great significance to prevent and monitor the occurrence of SPM in CACS at the first 10 year after PM.
The spectrum of SPM in CACS also changed dynamically. Our results suggested that special surveillance should be carried out for non-lymphocytic leukemia, brain and testicular cancers at the first 10 year after PM; for breast, thyroid and brain cancers at the second and third 10 year after PM; for breast, lung and colorectal cancers after the third 10 year after PM. Stanislaw Garwicz et al. reported the percent distribution of excess numbers of SPM in childhood cancer survivors[12]. He found that brain cancer accounts for the largest proportion at the age of 0-14 and 15-39 years and breast cancer accounts for the largest proportion at the age of 40-59 and ≥ 60 years. Another study showed the SPM with the largest proportion at the 4 age groups of 5-19, 20-29, 30-39 and ≥ 40 years was bone cancer, glioma, breast cancer and genitourinary cancer, respectively[13]. Despite the difference in SPM with the largest proportion, the change trend of brain, lung and colorectal cancers with increasing age in these two studies were in consistence with our results.
Although the risk factors of SPM in CACS during the entire follow-up period has been extensively investigated, few previous studies have attempted to explore the risk factors of SPM in CACS dynamically at different period of follow-up[16, 22-24]. Thus, the risk factors at different period of follow-up were analyzed in our study aiming at identifying CACS at high risk of SPM at specific follow-up periods. We found that being male were associated with lower odds of developing SPM at each period of follow-up. Similar association was reported in Joseph P. Neglia’s study [16]. He also found that radiotherapy was risk factors of SPM. However, our study suggested this association does not apply at each period of follow-up. Notably, our study revealed that the CACS who had undergone chemotherapy had less likelihood of developing SPM at follow-up of 1-10 years but more likelihood at other periods of follow-up. However, previous study reported that several types of chemotherapeutics are associated with the occurrence of myeloid neoplasms after PM, including alkylating agents, topoisomerase II inhibitors, and antimetabolites [25]. Additionally, acute myeloid leukemia after alkylating-agent exposure typically arises after a latency of 5 to 8 years, which matches the first period of follow-up in our study[26]. Our study only evaluated risk factors of the summary of SPM but not for specific subtype of SPM. So, the carcinogenic effect of chemotherapy on myeloid neoplasms might be masked by the protective effect of chemotherapy on other cancers at the first period of follow-up. More investigations are needed to elucidate the association between therapeutic exposures and occurrence of SPM in CACS.
There were still some limitations in our study. First, since some registries in the SEER database were not included before 1992, we only analyzed data from 9 of 21 registries. Second, data on treatments in the SEER database were not detailed enough; thus, we were unable to examine the relationship between SPM and treatment modality. Third, SPM risk may be underestimated as some cases might not be registered owing to various reasons. Large cohort studies of cancer survivors with detailed data on treatment are still needed to further validate our findings and explore the association between SPM and treatment exposure.
Concluding, the risk of SPM in CACS is higher than that in other age groups and thus more attention should be paid to surveillance of SPM in CACS. We found that the risk of SPM in CACS decreases over time, suggesting the necessities of intensively monitoring SPM in CACS at the first 10 year after PM. Moreover, the spectrum and risk factors of SPM also changes dynamically with follow-up time and our study demonstrated at specific period of follow-up, specific population of CACS and specific subtypes of SPM should be surveilled and prevented closely. Taken together, our study provides guidance for dynamic surveillance of SPM in CACS to decrease the onset and promote the early diagnosis of SPM.
Authors’ contributions
Zijun Zhen: Concept and design, Statistical analysis, Administrative, technical, or material support, Drafting of the manuscript, Supervision. Kaibin Yang: Concept and design, Statistical analysis, Administrative, technical, or material support, Drafting of the manuscript. Yuanzhe Zhang: Statistical analysis, Administrative, technical, or material support, Acquisition, analysis, or interpretation of data, Drafting of the manuscript. Zihang Chen: Statistical analysis, Administrative, technical, or material support, Acquisition, analysis, or interpretation of data, Drafting of the manuscript. Wei Chen: Statistical analysis, Administrative, technical, or material support, Acquisition, analysis, or interpretation of data, Drafting of the manuscript. Yuqing Liang: Acquisition, analysis, or interpretation of data. Tingting Chen: Acquisition, analysis, or interpretation of data. Dongwei Huang: Acquisition, analysis, or interpretation of data. Jinwei Chen: Acquisition, analysis, or interpretation of data. Sifan Qi: Acquisition, analysis, or interpretation of data
Ethics approval and consent to participate
The SEER data are anonymized and publicly available, so there was no need to seek institutional ethics committee’s approval and consent from the participants for this study.
Consent for publication
Not applicable.
Data availability
SEER database is publicly available. The data supporting the findings of this study are available in SEER database at https://seer.cancer.gov/.
Competing interests
The authors declare no conflict of interest.
Funding information
The author(s) received no specific funding for this work.
- Howlader N, NA Krapcho M, Garshell J, Neyman N, Altekruse SF, et al. (2020) SEER Cancer Statistics Review 1975-2010.
- Murphy SL, J Xu, KD Kochanek (2013) Deaths: final data for 2010. Natl Vital Stat Rep 61: 1-117.
- Siegel RL, KD Miller, A Jemal (2018) Cancer statistics, 2018. CA Cancer J Clin 68: 7-30.
- Oeffinger KC (2006) Chronic health conditions in adult survivors of childhood cancer. N Engl J Med 355: 1572-82.
- Bhatia S (2015) Collaborative Research in Childhood Cancer Survivorship: The Current Landscape. J Clin Oncol 33: 3055-64.
- Wasilewski-Masker K (2009) Late recurrence in pediatric cancer: a report from the Childhood Cancer Survivor Study. J Natl Cancer Inst 101: 1709-20.
- Armstrong GT (2009) Late mortality among 5-year survivors of childhood cancer: a summary from the Childhood Cancer Survivor Study. J Clin Oncol 27: 2328-38.
- Bhatia S, C Sklar (2002) Second cancers in survivors of childhood cancer. Nature reviews. Cancer 2: 124-32.
- Turcotte LM (2019) Chemotherapy and Risk of Subsequent Malignant Neoplasms in the Childhood Cancer Survivor Study Cohort. J Clin Oncol 37: 3310-9.
- Teepen JC (2017) Long-Term Risk of Subsequent Malignant Neoplasms After Treatment of Childhood Cancer in the DCOG LATER Study Cohort: Role of Chemotherapy. J Clin Oncol 35: 2288-98.
- Kattner P (2019) Compare and contrast: pediatric cancer versus adult malignancies. Cancer Metastasis Rev 38: 673-82.
- Olsen JH (2009) Lifelong cancer incidence in 47,697 patients treated for childhood cancer in the Nordic countries. J Natl Cancer Inst 101: 806-13.
- Reulen RC (2011) Long-term risks of subsequent primary neoplasms among survivors of childhood cancer. JAMA 305: 2311-9.
- Cardous-Ubbink MC (2007) Risk of second malignancies in long-term survivors of childhood cancer. European journal of cancer (Oxford, England: 1990) 43: 351-62.
- Friedman DL (2010) Subsequent neoplasms in 5-year survivors of childhood cancer: the Childhood Cancer Survivor Study. J Natl Cancer Inst 102: 1083-95.
- Turcotte LM (2015) Risk of Subsequent Neoplasms During the Fifth and Sixth Decades of Life in the Childhood Cancer Survivor Study Cohort. J Clin Oncol 33: 3568-75.
- Park HS (2012) Overview of the Surveillance, Epidemiology, and End Results database: evolution, data variables, and quality assurance. Current problems in cancer 36: 183-90.
- Dutz A, S Löck (2019) Competing risks in survival data analysis. Radiother Oncol, 2019. 130: 185-9.
- Zhang Z (2017) Survival analysis in the presence of competing risks. Ann Transl Med 5: 47.
- Zhang, Z (2017) Nomogram for survival analysis in the presence of competing risks. Ann Transl Med 5: 403.
- Mukhtar F (2017) Survival predictors of Burkitt’s lymphoma in children, adults and elderly in the United States during 2000-2013. International journal of cancer 140: 1494-1502.
- Turcotte LM (2018) Risk, Risk Factors, and Surveillance of Subsequent Malignant Neoplasms in Survivors of Childhood Cancer: A Review. J Clin Oncol 36: 2145-52.
- Henderson TO (2012) Risk factors associated with secondary sarcomas in childhood cancer survivors: a report from the childhood cancer survivor study. Int J Radiat Oncol Biol Phys 84: 224-30.
- Kim H (2017) Risk Factor Analysis for Secondary Malignancy in Dexrazoxane-Treated Pediatric Cancer Patients. Cancer Res Treat 51: 357-67.
- Sill H (2011) Therapy-related myeloid neoplasms: pathobiology and clinical characteristics. Br J Pharmacol 162: 792-805.
- Travis LB (2013) Aetiology, genetics and prevention of secondary neoplasms in adult cancer survivors. Nat Rev Clin Oncol 10: 289-301.
FIGURE 1
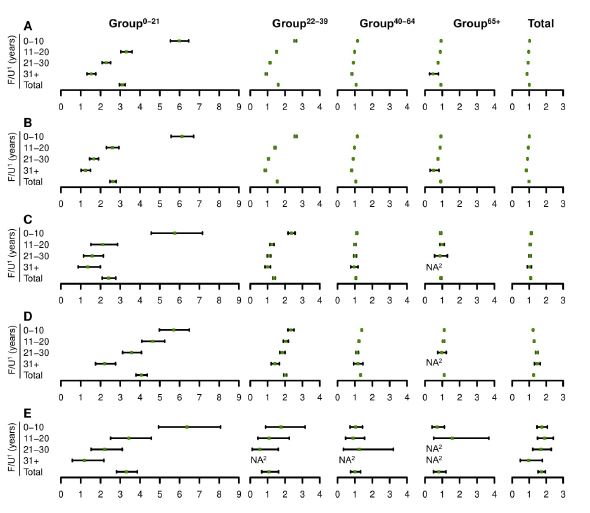
(A) All survivors with PM; (B) Survivors with solid PM; (C) Survivors with germ cell tumors as PM; (D) Survivors with hematologic PM; (E) Survivors with acute lymphoblastic leukemia as PM.
1F/U: follow-up; 2NA: No case of SPM was observed due to limited number of PM cases.
Figure 1: Forest plot of the SIR of all SPM in survivors of various PM by age at diagnosis and follow-up time
FIGURE 2
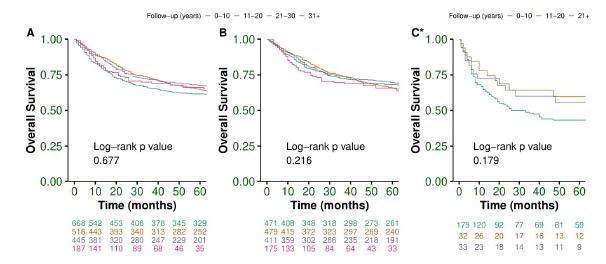
(A) OS of all SPM in CACS; (B) OS of solid SPM in CACS; (C) OS of hematologic SPM in CACS.
*For hematologic SPM, cases diagnosed at 21-30 and 30+ years of follow-up were pooled together due to the limited number of cases
Figure 2: OS of SPM in CACS diagnosed at different periods of follow-up.
FIGURE 3
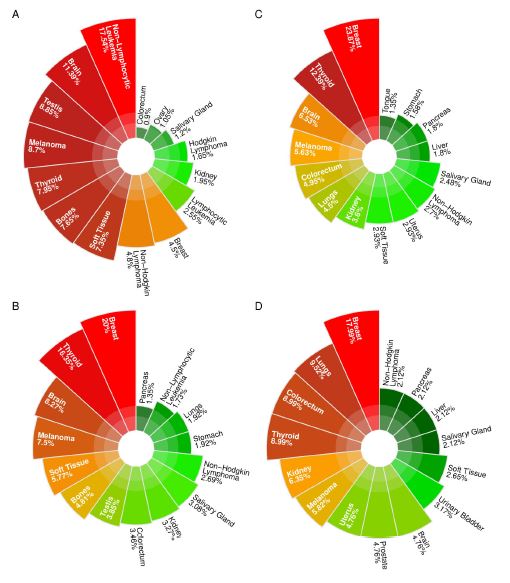
(A) 1-10 years; (B) 11-20 years; (C) 21-30 years; (D) 30+ years
Figure 3: Wind rose diagrams of the top 15 SPM in CACS at different periods of follow-up.
FIGURE 4
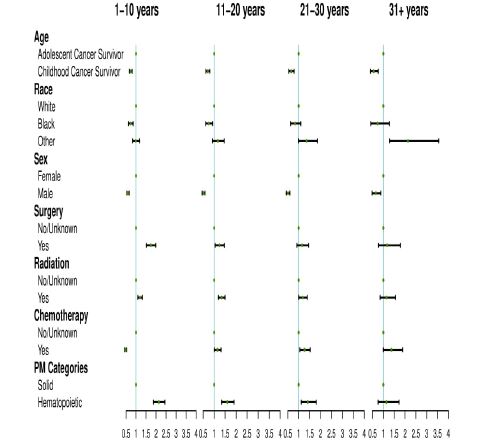
Figure 4: Risk factors of SPM in CACS at different periods of follow-up
FIGURE 5
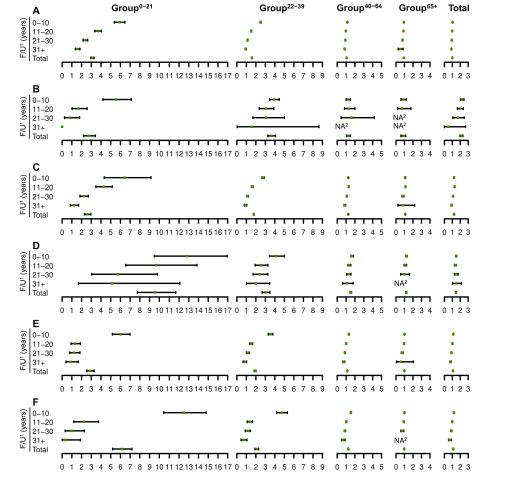
(A) Solid tumors as SPM in survivors of all types of PM; (B) Testicular cancer as SPM in survivors of all types of PM; (C) Breast cancer as SPM in survivors of all types of PM; (D) Soft tissue cancer as SPM in survivors of all types of PM; (E) Hematologic malignancy as SPM in survivors of all types of PM; (F) Leukemia as SPM in survivors of all types of PM.
1F/U: follow-up; 2NA: No case of SPM was observed due to limited number of PM cases.
Figure 5: Forest plot of SIR of selected SPM in survivors of all PM by age at diagnosis and follow-up time.
Tables at a glance
Figures at a glance