Accuracy of Visual Inspection Methods for the Diagnosis of Cervical Precancerous Lesions
Received Date: January 01, 2022 Accepted Date: February 02, 2022 Published Date: February 04, 2022
doi: 10.17303/jocr.2022.3.101
Citation:Elie NKWABONG (2022) Accuracy of Visual Inspection Methods for the Diagnosis of Cervical Precancerous Lesions. JJ Oncol Clin Res 3: 1-10.
Abstract
Objective: To access the accuracy of visual inspection methods for diagnosing cervical dysplasia.
Methods:This cross-sectional study was carried out between 1st December 2016 and 30th April 2017. All cases positive to Visual Inspections with Acetic acid (VIA) or with Lugol’s Iodine (VILI) as well as cases of macroscopic abnormal cervices,.irrespective of the results of visual inspection, had a colposcopy-directed biopsy
Results: A total of 109 women out of 1127 screened for cervical dysplasia had both visual inspection and biopsy done. he Sensitivity, Specificity, Positive predictive and Negative predictive values were 44.6%, 52.2%, 75% and 22.6% for VIA and.90.5%, 13.0%, 77.0% and 30% for VILI respectively
Conclusion: In our setting, the sensitivity of VILI in diagnosing cervical dysplasia is higher than that of VIA. Therefore, to reduce the rate of undiagnosed cervical dysplasia that might evolve to cancer, VILI should always be used in combination.with VIA
Keywords:Visual inspection methods; Cervical precancerous lesions; Sensitivity; Specificity; Positive predictive values; Negative predictive values; Likehood ratios
Introduction
Cervical cancer is the second most frequently diagnosed gynecological cancer worldwide after breast cancer [1]. In 2018, approximately 570,000 new cases of cervical cancer were diagnosed worldwide with 311,000 deaths [2]. Approximately 90% of cervical cancer deaths occurred in developing parts of the world. In less developed countries, it is the third leading cause of cancer death amongst females after breast and lung cancers. The highest incidence and mortality rate are reported in Africa [2].
The main risk factor for cancer of the cervix is HPV infection. HPV can induce dysplasia of most squamous epithelia. CIN 1 needs around 10 to 15 years to evolve to cervical cancer [3]. The timing from HPV infection to evidence of CIN-3 varies from 1 to 10 years.3 Immunosuppression can reduce this time interval.
Cervical precancerous lesions can be diagnosed at an early stage, given that the cervix is an organ easily accessible to clinical evaluation. Cervical cancer can be avoided if precancerous lesions are diagnosed and treated. This will lead to reduced mortality from cervical cancer.
Pap smear remains the method of choice for cervical dysplasia screening. In the developing world, there is frequent shortage of trained personnel that can interpret Pap smears. Moreover, some Pap smears or results get lost and some patients do not come back to collect their results. That is why visual inspection methods for the diagnosis of precancerous lesions are recommended.2 Visual inspection methods also have the advantage of allowing see-and-treat approach. Visual inspection methods include visual inspection with acetic acid (VIA) and visual inspection with Lugol’s iodine (VILI).
Both techniques are being used, but with more emphasis being put on VIA than on VILI, by WHO for its presumed superior sensitivity and specificity. The accuracy of these two techniques varies largely according to authors. VIA sensitivity ranges between 44% and 93.5% [4,5], and that of VILI may be as high as 82%.6 Hence, one technique might be more sensitive than other in a given area. No study in our unit has evaluated the reliability of these two methods for the diagnosis of cervical precancerous lesions, hence this study aimed at evaluating the accuracy of VIA and VILI for the diagnosis of cervical dysplasia.
Methods
This cross-sectional study was carried out in two University Teaching Hospitals in Yaoundé (Cameroon), between 1st December 2016 and 30th April 2017. All the women screened voluntarily for cervical dysplasia in the two screening units were included. For each woman, the cervix was cleaned with 0.9% saline solution and dried with a gauze, then colposcopy was performed. VIA was then done, followed by VILI three minutes later. Finally, colposcopy-directed biopsy was carried out when indicated.
Indeed, women who presented macroscopic architectural cervical changes, those with positive VIA (aceto-white colour after application of 5% acetic acid solution) or positive VILI (non-staining area after Lugol’s iodine application) had a colposcopy-directed cervical biopsy with pathologic examination. The positive VIA colposcopic appearance was the presence of sharp, well-defined, dense acetowhite areas on the cervix, with or without raised margins, close to the squamocolumnar junction in the transformation zone. The positive VILI colposcopic appearance was the absence of iodine staining.
The criteria for cervical biopsy were the presence of one of the following: polyp, mosaic (fine or coarse), punctation (fine or coarse), acetowhite epithelium (slow or rapid appearance), sharp borders, inner border sign, ridge sign, leucoplakia and lack of iodine staining. After biopsy, the specimen was included in a 10% formalin solution and sent to the pathology department. Women who refused biopsies and those with documented cervical cancer were excluded when analysing the accuracy of screening for cervical precancerous lesions. A written informed consent was obtained from each patient. This study received approval from the institutional ethics committee.
Our minimum sample size of 70 women with cervical dysplasia was calculated using the following formula7 for descriptive studies N=P(1-P) Zα2/D2 where Zα=1.96 corresponds to a confidence level of 0.05, D=0.06 is the degree of precision and the prevalence of cervical dysplasia (P) might be around 7% in our country.
The variables recorded on the questionnaire included patient’s age, the macroscopic appearance of the cervix, the result after application of acetic acid or Lugol’s iodine and the result of cervical biopsy. For each case of cervical dysplasia, the result obtained at VIA and VILI prior to biopsy was analysed.
Data were analysed using SPSS 21.0. The accuracies of VIA/VILI /cervical smear for diagnosing cervical dysplasia were accessed.
Results
A total of 1127 women were screened for cervical dysplasia using visual inspection methods. A total of 109 women had both visual inspection and biopsy done. VIA and/or VILI were positive in 102 cases (9.0%). Cervical biopsies were done amongst women (n=109) with only positive VIA (n=12), only positive VILI (n=55), amongst women with both tests positive (n=32), and amongst women with macroscopic cervical architectural changes negative to both VIA and VILI (n=10). Eight women refused biopsy (three with positive VIA/VILI and five with abnormal cervices).
Biopsy amongst the 109 women showed 74 dysplasia (6.6%), 16 non-dysplastic lesions, seven normal epithelia as well as 12 cases of either invasion (four or 0.4%) or microinvasion (eight or 0.7%) (Figure 1). These cases of cancer were excluded when analysing the accuracy of screening of cervical precancerous lesions.
The ages of women with cervical dysplasia ranged between 24 and 60 years with a mean of 41.0 ± 8.0 years.
On macroscopic examination, amongst women with dysplasia (n=74), the cervix was normal in 50 cases (67.6%) and abnormal in 24 cases (32.4%). Amongst the 23 women without dysplasia, the cervix was macroscopically normal in seven cases (30.4%) and abnormal in 16 cases (69.6%).
The results of non-dysplastic cervical anomalies are presented in Table 1. After excluding the 12 women with cervical cancer from the population under study, 97 women/1115 (8.7%) had both visual inspection methods and biopsy done. Only 31/97 women (31.9%) were previously screened negative with visual inspection methods while 66 had never been screened before (68.1%).
After application of 5% acetic acid solution, 44 cases out of the 97 women were positive (45.3%). After lugol application, 87 cases were positive (89.6%).
Amongst the 10 women with macroscopic cervical architectural changes negative to both VIA and VILI, biopsy revealed four cases of dysplasia (two CIN2 and two CIN3), three cases of cancer, two epidermoid papillomata and one Malpighian acanthosis.
The 74 cases of dysplasia included 30 CIN1, 36 CIN2 and eight CIN3/CIS on cervical biopsy.
The accuracies of VIA and VILI for the diagnosis of cervical dysplasia are reported in Tables 2, 3 and 4.
Discussion
Our data showed that the prevalence of cervical dysplasia in our units (6.6%) was slightly lower than that presumed (7%). As concerns patient’s age, the mean age observed in our study (41.0 years) was higher than that of 35.7 observed in Pakistan [5]. This can be explained by the fact that their youngest patient was 19, while the youngest patient in our study was 24 years old. According to some societies, screening should concern women aged between 25 and 65 to 69 [8,9]. Our patient aged 24 had the first sexual intercourse at age 11. She could even have had cervical dysplasia many months earlier, given that it was the first time she was being screened. Although there is no unanimity on age at first screening, we think that it should start earlier, for instance at 21 years as done by Ryu KJ et al in the Korea University Medical Center, Seoul (Korea) [10], especially amongst women whose first sexual intercourse occurred before age 12. Another patient in our study had first sexual intercourse at age 11. Age at first intercourse is decreasing, some adolescents having sexual intercourse, consented or not, at age 8 or 9 [11,12].
The presence of cervical invasion or micro-invasion in some women might be explained by the late diagnosis of cervical precancerous lesions, given that the majority of these women never performed previous cervical screening.
The sensitivity of VIA in our series was lower than the 93.5%, 68.7% and 59.4% found in Pakistan, India and Thailand respectively [5,6,13]. VIA sensitivity varies largely according to authors. The ability of dysplastic cells to synthetize high quantity of proteins might depend on the nutritional status, given that (essential) amino acids are needed for protein synthesis. Poor nutrition is usually observed in developing countries such as ours, due to low socioeconomic status. This might explain why VIA sensitivity was low in our setting. Moreover, the expression of the gene that codes for proteins synthesis might be reduced in those dysplastic cells. Further studies are needed to confirm these hypotheses.
This low sensitivity of VIA reveals that it is ineffective in reducing mortality from cancer of the cervix in our setting. The government should look for financial resources to put an emphasis on HPV vaccination rather than on screening.
The specificity of VIA was 52.2% in our study. This was also lower than the rates of 95.8%, 76.2% and 87% noticed in Pakistan, Thailand, and India respectively.5,13,14 The negative predictive value of VIA observed in our study (22.6%) was lower compared to 99% and 90.8% observed by some authors.5,13 These differences might be justified also by the difference in nutritional status, especially proteins intake, between those countries and ours.
The sensitivity of VILI noticed in our series (90.5%) was comparable to 81.8% noticed in India [6].
When VIA and VILI were used together in our study, the sensitivity was 94.6%. Using the two together decreases the rate of false negative because some lesions were positive to 5% acetic acid while others were so to iodine. The authors, therefore, suggest that both methods should be used in areas where the sensitivity of VIA is low, as our environment.
The presence of dysplasia and cancer amongst women with macroscopic cervical architectural changes negative to both VIA and VILI reminds us that biopsy should be directly carried out in such cases, i.e. when the cervix looks abnormal.
One limitation of our study was our inability to perform biopsy in some women because they refused, given that some of them could not contribute financially to both VIA/VILI and biopsy, as biopsies might have increased the size of our population with cervical dysplasia. Indeed, women with low socioeconomic status are at highest risk of cervical cancer. Moreover, for financial reasons, we could not carry out cytology and HPV tests. It should be reminded that although inspection methods have good accuracy for cervical cancer screening, pap smears and guided biopsies are the methods of choice
Conclusion
Cervical dysplasia can occur amongst women aged less than 25 years, especially those whose sexarche was before age 10. Therefore, screening should start earlier amongst these women, if enough resources are available. To reduce the rate of undiagnosed cervical dysplasia that might evolve to cancer, VILI should always be used in combination with VIA, especially in our environment where VILI has a higher sensitivity. Cervical biopsy should be performed in women with macroscopic cervical architectural changes, even when negative for VIA or VILI. Colposcopy-directed biopsies should be encouraged for suspicious cervices, as suggested by many. HPV vaccination might be the method of choice, especially in resource limited countries, as it will be more cost effective in preventing cervical precancerous lesions.
Conflict of interest
The authors have none to declare.
- Parkin DM, Bray F (2006) The burden of HPV related cancers. Vaccine 24: S11–S25.
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, et al. (2018) Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 68: 394–424.
- Moscicki AB, Schiffman M, Kjaer S, Villa LL (2006) Updating the natural history of HPV and anogenital cancer. Vaccine 24: S3/42–51.
- Omenge Orang'o E, Liu T, Christoffersen-Deb A, Itsura P, Oguda J, et al. (2017) Use of visual inspection with acetic acid, Pap smear, or high-risk human papillomavirus testing in women living with HIV/AIDS for posttreatment cervical cancer screening: same tests, different priorities. AIDS 31: 233-40.
- Khan M, Sultana SS, Jabeen N, Arain U, Khans S (2015) Visual inspection of cervix with acetic acid: a good alternative to pap smear for cervical cancer screening in resource-limited setting. J Pak Med Assoc 65: 192-5.
- Bobdey S, Balasubramanium G, Kumar A, Jain A (2015) Cancer Screening: Should Cancer Screening be Essential Component of Primary Health Care in Developing Countries? Int J Prev Med 6: 56.
- Kieser M, Friede T (2000) Re-calculating the sample size in internal pilot study designs with control of the type I error rate. Statist Med 19: 90111.
- Dumont A, Bessières N, Benbassa A, Razafindrafara G, Rabearison F, et al. (2017) J Gynecol Obstet Hum Reprod 46: 327-32.
- Nygård JF, Skare GB, Thoresen SØ (2000) The cervical cancer screening programme in Norway, 1992–2000: changes in Pap smear coverage and incidence of cervical cancer. J Med Screen 9: 86-91.
- Ryu KJ, Lee S, Min KJ, Hong JH, Song JY, et al. (2016) Management of atypical squamous cells of undetermined significance or low-grade squamous intraepithelial lesions of the uterine cervix with human papilloma virus infection among young women aged less than 25 years. Diagn Cytopathol 44: 959-63.
- Pitche P (2005) [Child sexual abuse and sexually transmitted infections in sub-saharan Africa] [Article in French]. Med Trop 65: 570-4.
- Kirkpatrick AW, Pelosi P, De Waele JJ, Malbrain ML, Ball CG, et al. (2010) Clinical review: Intra-abdominal hypertension: does it influence the physiology of prone ventilation? Critical care (London, England) 14: 232.
- Poomtavorn Y, Suwannarurk K (2015) Accuracy of visual inspection with acetic acid in detecting high-grade cervical intraepithelial neoplasia in pre- and post-menopausal Thai women with minor cervical cytological abnormalities. Asian Pac J Cancer Prev 16: 2327-31.
- Bhattacharyya AK, Nath JD, Deka H (2015) Comparative study between pap smear and visual inspection with acetic acid (via) in screening of CIN and early cervical cancer. J Midlife Health 6: 53-8.
FIGURE 1
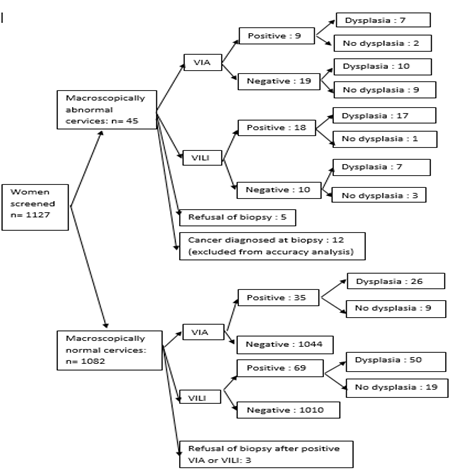
Figure 1:Flowchart showing screening sequences: Among women with macroscopic normal cervices, 34 cases of VIA negative were positive at VILI. Biopsies revealed 31 dysplasia and 3 normal results
Tables at a glance
Figures at a glance