Bilateral Commissuroplasty and Primary Repair for lower lip Gefect (30-80%)after Cancer Excision
Received Date:October 19, 2022 Accepted Date:November 19, 2022 Published Date:November 21, 2022
doi: 10.17303/jocr.2022.3.205
Citation: SJ Khoshnevis, M Yousefi, M Seraj, F Abbasvandi, P Sadeghi, Z Khoshnevis, ME Akbari (2022) Bilateral Commissuroplasty and Primary Repair for lower lip Gefect (30-80%) after Cancer Excision. JJ Oncol Clin Res 3: 1-8
Abstract
Introduction: Lip reconstruction is an essential step in lip tumors. In this regard, there are many procedures with good outcomes. Flap problems are the possibility of necrosis and an extensive suture line that wrecks aesthetics. Our technique has no flaps for defects of more than 30% of the lip, and the suture line is minimal.
Methods: This study is a surgical technique report from a single center. The original technique was based on our experience with about 100 patients in 25 years. But in this study, ten patients were included. After excising the tumor, a bilateral 10-15 mm horizontal skin incision beginning from the commissures to the lateral sides was made. The skin and mucosa were dissected from the underlying orbicularis muscle, and the muscle was partially cut about 15 mm from each side. Then the remaining sides of the lip were advanced and repaid in four layers. Finally, the released mucosa was sutured to the angle of incised skin.
Results: The patients were followed for at least three years. Oral competence was good, mobility and sensation were well preserved,the scars were less than other flaps, and the aesthetic was satisfying. The patients did not have drooling, flap edema, and pin cushioning
Conclusions: Among various techniques for lower lip reconstruction, the presented process in this study seems to be safe andstraightforward, but to measure all aspects of it, other surgeons need to use this method and express their opinions.
Keywords: Lip Neoplasms; Reconstruction; Lower lip; Primary repair
Introduction
The lips have essential and diverse functions, including oral competence, deglutition, articulation, and expression of emotion. The lips are brought together to close the mouth by the role of the orbicularis oris, a complex sphincter muscle [1]. Some of the muscle fibers of the orbicularis oris derive from intrinsic fibers of the lips, whereas others derive from other facial muscles that insert into the lips [2-3]. The platysma, depressor labii inferioris, and depressor anguli oris muscles mainly control depression and retraction of the lower lip. The primary motor nerves of the lips are the facial nerve's buccal and marginal mandibular rami. The marginal mandibular supplies the lower lip depressors. Sensory innervation of the lips is via the infraorbital and mental branches of the trigeminal nerve [2-4] and supplies from superior and inferior labial arteries, with venous drainage to the anterior facial vein [2-4] lymphatic drainage is through submental and submandibular lymph nodes [2-4]. Researchers have described many reconstructive techniques to overcome significant defects, such as "cross-flap" developed by Abbé and Estlander [5-6], using the opposite lip with the various modifications suggested [7-8], and Karapandzic technique [9]. This technique provides the excellent advantage of preserving the nerves and blood vessels of the flaps and allows an excellent sphincteric function to be maintained [10-11]. Bernard- Burow's method and other versions (fan-flap procedure) are also helpful in cases with more lip loss [12]. Also, new flaps have been introduced, each of which has advantages and disadvantages [13-17].
Lip reconstruction aims to maintain oral competence, mobility, and sensation and obtain the best aesthetic results. When the size of the stoma becomes less than 50% after reconstruction, it can be problematic for those who wear dentures. Maintaining harmony, symmetry, and adequate size is critical for cosmesis [18]. After excision, it is necessary to repair the sphincter ring using all four layers (mucosa, muscle, subcutaneous tissue, and skin) simultaneously [19]. Reconstruction should provide an adequate oral opening and mucosa adjacent to the commissure to avoid contracture [20-21]. The present study aimed to investigate a new technique for lower lip reconstruction after tumor excision resulting in a medium-sized defect.
Methods
This study is a surgical technique report from a single center. The original technique was based on our experience with about 100 patients in 25 years. A total of 10 patients referred to our hospital from 2105 to 2018 participated in this study and were followed up for three years. Informed consent was obtained from patients before participation in the study. Lower lip defects occurred in all patients following squamous cell carcinoma excision. The patients were in stage 3 of TNM classification, and none of them had positive lymph nodes. No antibiotics were given before surgery.
Surgical technique
Wide local excision of the lower lip tumors was performed under general anesthesia. Reconstruction was undertaken after the margins were shown to be free of cancer by frozen sections. In this technique, the lower lip defect will primarily be repaired even if the defect is more than 30% of the lip. After excising the tumor, A bilateral 10mm to 15mm horizontal skin incision begins from the commissures to the lateral sides (Figure 1A). Then the skin and mucosa will be dissected from the underlying orbicularis muscle, and the muscle will be cut partially about 15 mm on each side (Figure 1B). Commonly no vessels needed to be ligated and back cut. Two sides of the lip (tumor site defect) will be advanced and sutured in four layers separately, and a vertical suture line will be created (Figure 1C). Finally, the median of the dissected mucosa in the commissures will be sutured to the angle of incised skin. Then complete mucosa to skin suturing (Figure 1C).
Results
The technique used in this study has a history of 25 years of experience and has almost not any complications in these few years. Since our data during those 25 years is incomplete, we have conducted the study on ten patients. The patients included two females and eight males with a mean age of 61. The defect size was all above 50% except in one case. Five patients had hypertension, and 5 had diabetes mellitus (Table 1). The average operation time was about 70 minutes. Sutures were drawn between 5 and 7 days. Early and late postoperative results were satisfactory. No second surgery for modification was needed. At a 3-year follow-up, the patients were doing well with excellent functional and aesthetic outcomes, and there was no recurrence. Lip apertures and movements were normal, with sufficient mouth opening and oral competence and good volume and quality of the vermillion. The patients have no complaints of drooling. Speech and sensation were preserved, and highly pleased with the outcome. Figure 2 shows a case in pre-surgical and post-surgical (Figure 2).
Discussion
There are many surgical techniques for the reconstruction of the lower lip. The results of the traditional methods have been adequate and sometimes excellent, especially in elderly patients with thin lips. However, the patients, especially young patients, have suboptimal aesthetic problems. For defects less than 30%, a primary repair is an acceptable option, and it's not challenging. For defects of more than 30% of the lower lip, which is the most challenging among surgeons, several flaps are proposed: the Abbe flap [20], the neurovascular Karapandzic flap [9], and the Bernard-Webster flap [22]. For more significant defects, not including the angles of the mouth, Gillies's fan is a good choice [23]. One of the choices for Defects involving the commissure is the Estlander flap [5]. All of them have advantages and disadvantages. In the case of local flaps, flap loss, blunting of the repaired commissure, lip asymmetry, sensory loss, hypersensitivity, edema, microstomia, poor oral competence with drooling, undesirable scarring, and flap necrosis must be considered. The Karapandzic flap has the potential risk of microstomia and blunting of the oral commissure [24]. With the Karapandzic flap, we have to maintain lip mobility with preserved sensation and competence, but reconstruction of significant defects inevitably results in microstomia, necessitating secondary commissuroplasty [25]. The Webster-Bernard procedure using cheek advancement flaps can give an appropriate lip reconstruction but involves a sizeable perioral tissue loss. Also, it has significant perioral scarring with contour deformity [26]. In addition, effacement of gingivo-buccal sulcus and notching of the central lip has been described as common aesthetic disadvantages [27].
In the Estlander flap, rotation of a lateral area of the upper lip to the commissure is done first, and a second surgery is necessary to reconstruct the commissure angle. Therefore, it needs two operations. The Gillies fan flap has enough tissue to repair with no tension, but the commissure is distorted and blunted, and the lower lip gets short [28]. Also, it has a long suture line, distorting the cosmesis. Analysis for aesthetic results was based on those with pre-and postoperative photographs. Oral competence was measured by muscular integrity and aperture. The orbicularis muscle was partially cut and correctly functioned, and the muscular integrity was preserved. . The aperture and mobility were patient-reporting and asked by dentures and eating problem when eating by spoons or big morsels No drooling was reported, and the severity of drooling was measured by the Blasco index [29]. Fortunately, none of the above problems were reported by patients. And overall the oral competence was good.
Among various techniques for lower lip reconstruction,this technique seems safe and straightforward. Still, other surgeons need to use this method to measure all aspects of it and express their opinions.
Authors'contributions
This work was carried out in collaboration between all authors, and all authors read and approved the final manuscript.
Conflict of interest
Authors have declared that no conflict of interest exists.
- Zide B (1990) Deformities of the lips and cheeks in McCarthy JG (Ed), Plastic Surgery. Philadephia. WB Saunders.
- Bradley C, Leake JE (1984) Compensatory reconstruction of the lips and mouth after major tissue loss. Clinics in plastic surgery 11: 637-53.
- Jabaley ME, Orcutt TW, Clement RL (1976) Applications of the Karapandzic principle of lip reconstruction after excision of lip cancer. The American Journal of Surgery 132: 529-32.
- Boukovalas S, Boson AL, Hays JP, Malone CH, Cole EL et al. (2017) A Systematic Review of Lower Lip Anatomy, Mechanics of Local Flaps, and Special Considerations for Lower Lip Reconstruction. J Drugs Dermatol 16: 1254-61.
- Abbe R (1968) A new plastic operation for the relief of deformity due to double harelip. Plastic and reconstructive surgery 42: 481-3.
- Estlander J (1872) Eine Methode aus der einen Lippe Substanzverluste der anderen zu ersetzen. Arch klin Chir 14: 622-31.
- Bucur A, Stefanescu L (2004) Management of patients with squamous cell carcinoma of the lower lip and N0-neck. Journal of Cranio-Maxillofacial Surgery 32: 16-8.
- Zitsch III RP (1993) Carcinoma of the lip. Otolaryngologic Clinics of North America 26: 265-77.
- Karapandzic M (1974) Reconstruction of lip defects by local arterial flaps. British journal of plastic surgery 27: 93-7.
- Gooris PJ, Vermey A, de Visscher JG, Burlage FR, Roodenburg JL (2002) Supraomohyoid neck dissection in the management of cervical lymph node metastases of squamous cell carcinoma of the lower lip. Head & Neck: Journal for the Sciences and Specialties of the Head and Neck 24: 678-83.
- Raskob GE, Zitsch III RP, Park CW, Renner GJ, Rea JR JL (1995) Outcome analysis for lip carcinoma. Otolaryngology– Head and Neck Surgery 113: 589-96.
- Bernard C (1853) Cancer de la levre inferieure opere par un procede nouveau. Bull Mem Soc Chir Paris 3: 357-64.
- Bali ZU, Ozkan B, Parspancı A, Kececi Y, Yoleri L (2021) Reconstruction of lower lip defects with free super-thin anterolateral thigh flap. Microsurgery 41: 216-22.
- Costa-Gonzalez JM, Sumarroca A, Aguilera-Saez J, Martel-Martin M, Leidinger A et al. (2021) Reconstruction of the lower lip after broad oncologic resection by Colmenero flap: a reliable option. Acta Otorhinolaryngol Ital 41: 507-13.
- Dewey EH, Roche AM, Lazarus CL, Urken ML (2017) Total lower lip and chin reconstruction with radial forearm free flap: A novel approach. Am J Otolaryngol 38: 618-25.
- Madorsky S, Meltzer O (2020) Myomucosal Lip Island Flap for Reconstruction of Small to Medium Lower Lip Defects. Facial Plast Surg Aesthet Med 22: 200-6.
- Tourrier M, Honeyman CS, Lopez MA, Casanova D, Grandpierre X et al. (2021) [Total reconstruction of the lower lip: Lip suspension technique by double nasolabial rigging and review of the literature]. Ann Chir Plast Esthet 66: 167-73.
- Neligan PC (2009) Strategies in lip reconstruction. Clin Plast Surg 36: 477-85.
- Moretti A, Vitullo F, Augurio A, Pacella A, Croce A (2011) Surgical management of lip cancer. Acta Otorhinolaryngologica Italica 31:5.
- Abbe R (1898) A NEW PLASTIC OPERATION FOR THE RELIEF OF DEFORMITY DUE TO DOUBLF HARELIP. Medical Record (1866-1922) 53:477.
- Vukadinovic M, Jezdic Z, Petrovic M, Medenica LM, Lens M (2007) Surgical management of squamous cell carcinoma of the lip: analysis of a 10-year experience in 223 patients. Journal of oral and maxillofacial surgery 65: 675-9.
- WEBSTER RC, COFFEY RJ, KELLEHER RE (1960) Total and partial reconstruction of the lower lip with innervated muscle-bearing flaps. Plastic and reconstructive Surgery 25: 360-71.
- Gillies H, Millard DR (1957) The principles and art of plastic surgery: Butterworth.
- Brougham ND, Adams BM (2020) A Modification of the Webster-Bernard Lip Reconstruction. Plastic and Reconstructive Surgery Global Open 8.
- Zide B (1990) Deformities of the lips and cheeks. Plastic surgery 3: 2009-56.
- El-Din SAS (2003) Lower lip reconstruction with Fujimori gate flaps. Egypt J Plast Reconstr Surg27: 319-24.
- Langstein HN, Robb GL (2005) Lip and perioral reconstruction. Clinics in plastic surgery 32: 431-45.
- Jackson IT, Disa JJ (2008) Local flaps in head and neck reconstruction. Plastic and Reconstructive Surgery 121: 2172.
- Blasco PA, Allaire JH (1992) Drooling in the developmentally disabled: management practices and recommendations. Consortium on Drooling. Dev Med Child Neurol 34: 849-62.
FIGURE 1
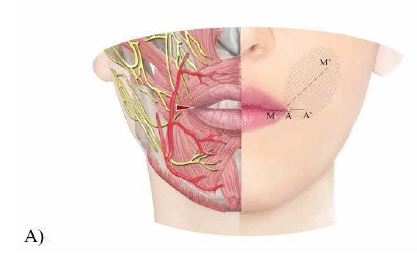
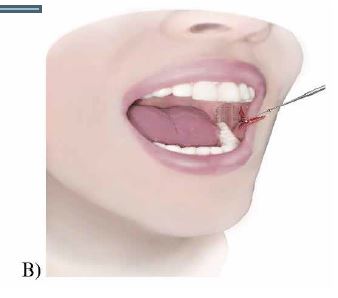
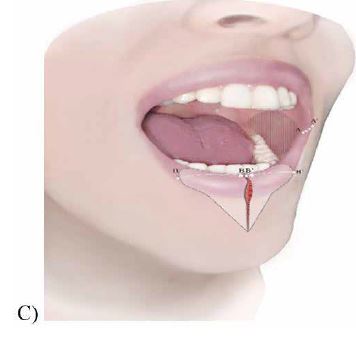
Figure 1: Surgery steps. All the incisions were bilaterally, but we made the incisions on one side to show the inside of the mouth in the pictures. A) First, an incision is made from A to A1. Then, an M to M1 incision will be made in the mouth. B) The muscle has been excised from the skin and mucosa and then back cut. C) B to B1 is the tumor site that has been removed, and B is sutured to B1 in the midline, resulting in a vertical suture line. The median of the dissected mucosa in the commissures sutured to the angle of incised skin from A to A1
FIGURE 2
.JPG)
.JPG)
.JPG)
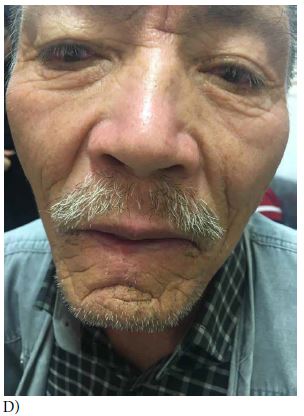
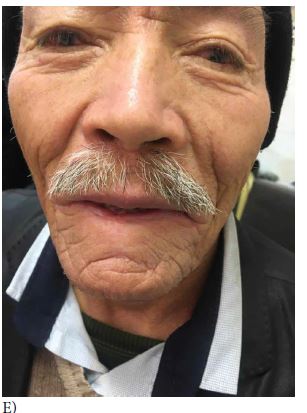
Figure 2: Case 6. A) before surgery. B) in operation, the tumor is resected. C) Early post-operation. D) Post-operation year 2. E) Post-operation year 3
Tables at a glance
Figures at a glance