Analysis of Electrocardiogram Characteristics and Related Factors after Breast Cancer Surgery
Received Date:January 21, 2023 Accepted Date: February 21, 2023 Published Date:February 24, 2023
doi: 10.17303/jocr.2023.4.101
Citation: Xinyu Li, Caixia Li (2023) Analysis of Electrocardiogram Characteristics and Related Factors after Breast Cancer Surgery. JJ Oncol Clin Res 1-13.
Abstract
Objective: To analyze the electrocardiogram characteristics as well as related factors after breast cancer surgery
Methods: A total of 128 breast cancer patients admitted to the Oncology Department of our hospital from January 2020 to June 2022 were selected, including 64 cases of chemoradiotherapy (observation group, OG) and 64 cases of simple surgery (control group, CG). The differences of myocardial enzyme index including creatine kinase (CK), creatine kinase isoenzyme (CK-MB), lactate dehydrogenase (LDH) and blood deficiency modified albumin (IMA), cardiac function index including left ventricular ejection fraction (LVEF), shortening rate of left ventricular short axis (LVFS), left atrial ventricular diastolic early peak E/ peak A (E/A), end diastolic diameter of left ventricle (LVEDd) and end-systolic diameter of left ventricle (LVESd), as well as ECG indicators including heart rate, corrected QT (QTc) time, abnormal T wave rate, and abnormal ST-segment rate were compared between the two groups before, during and after treatment.
Results: Compared to the CG, serum CK, CK-MB, LDH as well as IMA levels in the OG were promoted during and after treatment (P < 0.05). In contrast to the CG, LVEF of the OG was declined during and after treatment, and the E/A of the OG was reduced during treatment (P < 0.05). In comparison with the CG, the QTc time and the incidence of abnormal T wave in the OG were enhanced (P < 0.05). The time of menarche (age at menarche less than 12 years old) and history of diabetes (no history of diabetes) were two related factors significantly shorter than those before surgery (P=0.005 and P=0.028).
Conclusion: Compared with radical surgery alone, breast cancer patients receiving radiotherapy at the same time have a more obvious impact on cardiac function and myocardial injury, so echocardiography and electrocardiogram monitoring can be strengthened for these patients.
Keywords: Breast Cancer, Electrocardiogram, Cardiac Function, Surgery
Introduction
Breast cancer belongs to one of the malignant tumors with the highest incidence in female population. The current clinical treatment of breast cancer has developed from simple surgical resection to surgery, chemotherapy, radiotherapy and endocrine therapy [1,2]. Targeted therapy, such as gene therapy, is the principle of comprehensive treatment. However, while treating this disease, chemotherapy drugs also have certain toxicity to the patient’s heart, and perioperative cardiovascular events (CEs) are also a hidden danger to the health of patients, which can influence the quality of life together with prognosis of patients during the perioperative period. Electrocardiogram (ECG), as a means of detecting cardiac toxicity in clinical treatment, has been widely recognized and studied in the world [3].
Patients can now receive chemotherapy for longer periods of time and live longer as a result of improved treatment efficacy. Consequently, long-term management of chemo-related morbidities is becoming more and more necessary for cancer patients. In order to prevent the occurrence of medical heart failure with the aid of early pharmacologic intervention, it is crucial to identify chemotherapy-precipitated cardiac damage in the early stages. It has been proposed that the popular 12-lead electrocardiogram (ECG) enables the detection of various cardiotoxic findings, including sinus tachycardia, ST-T wave abnormalities, cardiac conduction problems, QT prolongation, fragmented QRS, and cardiac arrhythmia, during chemotherapies in cancer patients. Therefore, we aimed to assess the presence of ECG abnormalities in patients newly diagnosed with breast cancer after chemotherapy. However, in addition to chemotherapy, the effects of surgery and other related indicators on ECG changes in breast cancer patients are rarely reported.
Material and Methods
Clinical dataA total of 128 patients with breast cancer admitted to the Oncology Department of our hospital from January 2020 to June 2022 were selected, all female, including 64 patients in the observation group (OG) with radiotherapy and chemotherapy, aged 34-58 (43.9±7.4) years. There were 64 patients who underwent surgery alone (control group, CG), aged 30-65 (45.0±6.9) years. As displayed in Table 1, no significance was observed in the general data of the two groups (P > 0.05). Inclusion criteria: (1) Breast cancer was confirmed by ultrasound and pathological diagnosis, and all of them were left atrial tumors; (2) All patients underwent modified radical mastectomy in our hospital and were willing to undergo postoperative chemoradiotherapy and other related examinations; (3) Karnofsky (KPS) score ≥ 70 before chemoradiotherapy. Exclusion criteria: (1) Patients with thoracic, pulmonary or esophageal malignancies; (2) Patients with arrhythmia (atrial fibrillation and atrioventricular block), history of myocardial infarction, congenital heart disease and heart valve disease; (3) Pulmonary fibrosis, emphysema, etc. (4) Serious diseases of other systems. This study was approved by the medical ethics committee of the hospital, and patients in both groups signed informed consent.
As seen in Table 1, there were no differences in BMI, lesion diameter, tumor node metastasis classification (TNM) staging, and lesion location of the two groups (P > 0.05).
Methods
Radiotherapy and Chemotherapy for Breast CancerThe CG received doxorubicin + cyclopshosphamide sequential paclitaxel + trastuzumab combined chemotherapy: on the first day, doxorubicin (60 mg/m2 ) together with cyclophosphamide (600 mg/m2 ) were given intravenously for a course of 3 weeks. After 4 consecutive courses of treatment, the drug was stopped, and paclitaxel (175 mg/m2 ) together with trastuzumab (6 mg/kg, the first dose was 8 mg/kg) were given intravenously. After 4 consecutive courses of treatment, the drug was stopped, and trastuzumab (6 mg/kg) was given intravenously, 3 weeks as a course, and the drug was continuously administered for 1 year. The OG received radiotherapy based on the treatment in the CG: the affected breast and the drainage area of the supraclavicular and inferior clavicular lymph nodes were used as the target area of irradiation, with a dose of 200 cGy each time, once a day, 5 times a week, a total of 25 times of radiotherapy, with a total dose of 5000 cGy.
Detection of Myocardial Enzyme Index3 mL of fasting venous blood was gathered before treatment, during treatment (the 13th to 15th times of radiotherapy in the OG, the end of 8 courses of chemotherapy in the CG) and after treatment (1 month after treatment in the two groups), centrifuged at 3000 r/min for 10 min, and the serum was separated in a refrigerator at -80C for further examination. Creatine kinase (CK), creatine kinase isoenzymes (CK-MB), lactate dehydrogenase (LDH), as well as ischemic modified albumin (IMA) were examined by automatic biochemical analyzer from BD Company.
EchocardiographyBefore, during and after treatment (examination time was the same as myocardial enzyme index), echocardiography was performed by Philips ultrasonic diagnostic instrument (IU22, probe frequency 2-4 MHz, phased array probe) in the two groups. The observation indicators were left ventricular ejection fraction (LVEF), shortening rate of left ventricular short axis (LVFS), left atrial ventricular diastolic early peak E/ peak A (E/A), end diastolic diameter of left ventricle (LVEDd), as well as endsystolic diameter of left ventricle (LVESd).
ElectrocardiographyBefore, during and after treatment (the examination time was the same as myocardial enzyme indexes), electrocardiogram was detected by GE/MAC-5000 12-lead electrocardiogram in the two groups. The observation indexes were heart rate, corrected QT (QTc) time, abnormal T-wave rate and abnormal ST-segment rate.
Statistical AnalysisStatistical software SPSS 21.0 was used to express measurement data, and t-test was adopted for comparison between groups. Enumeration data were compared by word 2 test. P < 0.05 was significant.
Results
Comparison of myocardial enzyme indexes of both groupsAs shown in Figure 1, before treatment (T0), no significant differences were discovered in serum CK, CKMB, LDH and IMA levels of the two groups (P > 0.05). In comparison with the CG, the levels of these enzyme indexes in the OG during (T1) and after (T2) treatment were increased (P < 0.05). The levels of these enzyme indexes in the OG during (T1) and after (T2) treatment were elevated relative to those before treatment, and the above indexes after treatment were declined relative to those in the treatment (P < 0.05).
Comparison of Echocardiographic Indexes between both GroupsAs unveiled in Figure 2, no differences were found in these echocardiographic indexes of the both groups before treatment (P > 0.05). During and after treatment, LVEF and E/A in the OG were declined compared to the CG and before treatment (P < 0.05). LVFS, LVEDd and LVESd in the OG during and after treatment were elevated relative to the CG and before treatment (P < 0.05).
Comparison of Electrocardiogram Indexes between the Two GroupsAs indicated in Figure 3, before treatment, no significant differences were found in heart rate, QTc time, T wave abnormality and incidence of ST segment abnormality of both groups (P > 0.05). In comparison with the CG, the incidence of QTc time, T wave abnormality and ST segment abnormality in the OG was promoted. Compared with before treatment, the incidence of QTc time, T wave abnormality and ST segment abnormality in the OG was enhanced in the treatment (P < 0.05). After treatment, the incidence of QTc time, T wave abnormality and ST segment abnormality in the OG were declined compared to those in the treatment (P < 0.05).
Analysis of Related Factors of Electrocardiogram changes after Adenocarcinoma SurgeryAs shown in Table 2, among the 64 breast cancer patients in the CG, 8 had menarche less than or equal to 12 years old, the youngest was 11 years old, with a mean age of 11.63 years old, accounting for 12.50%; 47 were older than 12 years old and younger than 17 years old, with a mean age of 14.48 years old, accounting for 73.44%; 9 were older than or equal to 17 years old, with a mean age of 21 years old. The mean age was 17.68 years, accounting for 14.06%, and the three groups of samples were independent of each other. All the samples were divided into three groups according to the three indicators that had significant differences before and after surgery: QT interval shortening or prolongation, wave abnormality and ST segment abnormality. The above counts were analyzed by chi-square test. The outcomes of chi-square test manifested obvious differences between the time of menarche and the change of QT interval in postoperative electrocardiogram (P< 0.05).
The patients were divided into “yes” group (n = 12) and “no” group (n = 52) according to their preoperative history of diabetes. No correlation was discovered of the two groups, and the chi-square test was continued according to the above method. The statistical results indicated no significant difference was discovered between the preoperative and postoperative changes of T wave abnormalities and ST segment abnormalities and whether the patients had a history of diabetes before surgery (P>0.05). Nevertheless, a significant difference was observed betwen the postoperative changes of QT interval and whether the patients had a history of diabetes before surgery (P< 0.05). In other words, patients without a history of diabetes before surgery were more likely to have a shortened QT interval after breast cancer surgery (Table 3).
Discussion
Breast cancer is a common malignant tumor. It has been reported that breast cancer has become one of the most serious malignant diseases threatening women’s health in China, and young people represented by urban white-collar workers are at high risk of this disease [4-6]. More than 10% of the patients have multiple metastases at the time of diagnosis and miss the best opportunity for surgical treatment, which requires further treatment such as radiotherapy and chemotherapy.
As a common clinical treatment for malignant tumors, chemotherapy is often combined with radiotherapy, but it has a variety of toxicity, including extensive myocardial damage and vascular occlusion. Some studies have suggested that the combination of chemoradiotherapy is more significant to the heart injury of patients than radiotherapy or chemotherapy alone [7-9]. The results of this study demonstrated that, compared to the CG, serum CK, CK-MB, LDH and IMA levels in the OG were promoted during and after treatment. This result suggested that the myocardial injury of breast cancer patients undergoing chemotherapy combined with radiotherapy is more serious, which was also in line with the results of former studies [10]. The volume and dose of cardiac irradiation are important factors causing cardiac injury, and radiation can damage human capillary endothelial cells, and then damage the patients’ cardiac microcirculation. Functional diseases such as myocardial ischemia and hypoxia are more likely to occur under the influence of cardiac microcirculation disorders.
Echocardiography uses the special physical characteristics of ultrasonic shortwave to detect the anatomical structure and functional status of the heart and large blood vessels, and then evaluate the cardiac function of patients, with high sensitivity [11-13]. In this study, the changes of echocardiographic indexes of the two groups of patients showed that, compared to the CG, LVEF in the OG was declined during and after treatment, and the measured value of E/A during treatment was reduced. LVEF is a commonly used indicator to monitor the cardiotoxicity of anthracyclines in clinical practice. Relevant studies have suggested that the transient decrease of LVEF in the early stage of chemotherapy treatment may be a sensitive predictor for the occurrence of doxorubicin cardiotoxicity [14,15]. In this study, in comparison with the CG, E/A values of patients in the OG during treatment were declined, implying that echocardiography had certain specificity for detecting early cardiotoxicity of chemoradiotherapy, which could be considered for further study and application.
The outcomes of this research also proved that, in comparison with the CG, QTc time in the OG was longer. Meanwhile, the incidence of T wave abnormalities together with ST segment abnormalities in the OG was greater. These outcomes suggested compared with chemotherapy alone, cardiac injury in breast cancer patients treated with radiotherapy can be noninvasively monitored by electrocardiogram. QTc time is related to specific ventricular arrhythmias, namely tip torsion ventricular tachycardia, which is of great value in judging the degree of myocardial ischemia and predicting the risk of arrhythmia events. The prolonged QTc time is more serious in patients with abnormal electrocardiogram, suggesting that the possibility of triggering ventricular fibrillation is higher [16,17]. Radiation and anthracyclines can induce cardiomyocyte death and myocardial interstitial fibrosis by mediating related mechanisms after dose accumulation in patients, which shows T and ST segment changes in electrocardiogram.
In addition to the above findings, this study also found that the time of menarche (12>n>17) (P=0.005) and history of diabetes (no history of diabetes) (P=0.028) were associated with electrocardiogram changes. Through analyzing the clinical features of breast cancer patients in this study and using the chi-square test, we found there were two factors related to the significantly shorter QT interval in electrocardiogram of breast cancer patients after surgery: menarche time and history of diabetes, and both related factors had significant statistical differences in the changes of QT interval in electrocardiogram between breast cancer patients after surgery and before surgery. However, considering that the above two types of cases accounted for a large proportion in all the statistical cases (73.44% and 81.25%, respectively), and this research was a single-center study, the selection of cases was narrow, and the conclusion of the above two related factors was biased. Therefore, for patients who meet the above two related factors, clinicians need to make corresponding judgments based on the patient’s own condition and clinical actual situation.
In conclusion, compared with radical surgery alone, breast cancer patients receiving radiotherapy at the same time have a more obvious impact on cardiac function and myocardial injury, so echocardiography and electrocardiogram indicators can be strengthened for these patients.
Acknowledgement
None
Conflict of interest
None
- Yood MU, Wells KE, Alford SH, Dakki H, Beiderbeck AB et al. (2012) Cardiovascular outcomes in women with advanced breast cancer exposed to chemotherapy. Pharmacoepidemiol Drug Saf 21: 818-27.
- Zamorano JL, Lancellotti P, Rodriguez Muñoz D, Aboyans V, Asteggiano R et al. (2016) ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur Heart J 37: 2768-801.
- Liang X, Wang Y, Yin X, Gong X, Pan S et al. (2020) Electrocardiographic Characteristics of Breast Cancer Patients Treated with Chemotherapy. Cardiol Res Pract 6678503.
- Long HD, Lin YE, Zhang JJ, Zhong WZ, Zheng RN (2016) Risk of Congestive Heart Failure in Early Breast Cancer Patients Undergoing Adjuvant Treatment with Trastuzumab: A Meta-Analysis. Oncologist 21: 547-54.
- Gurdogan M, Ozkan U (2019) A Novel Predictor of Chemotherapeutic Cardiotoxicity in Patients with NonHodgkin Lymphoma. Oncol Res Treat 42: 375-81.
- Chen Q, Gasperetti A, Della Rocca DG, Mohanty S, Gedikli O et al. (2019) The Value of Baseline and Arrhythmic ECG in the Interpretation of Arrhythmic Mechanisms. Card Electrophysiol Clin 11: 219-38.
- Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E et al. (2005) Recommendations for chamber quantification: a report from the American Society of Echocardiography's Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr 18: 1440-63.
- Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A et al. (2015) Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 28: 1-39.e14.
- Galderisi M, Cosyns B, Edvardsen T, Cardim N, Delgado V et al. (2017) Standardization of adult transthoracic echocardiography reporting in agreement with recent chamber quantification, diastolic function, and heart valve disease recommendations: an expert consensus document of the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging 18: 1301-10.
- Rautaharju PM, Surawicz B, Gettes LS, Bailey JJ, Childers R et al. (2009) AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: part IV: the ST segment, T and U waves, and the QT interval: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society. Endorsed by the International Society for Computerized Electrocardiology. J Am Coll Cardiol 53: 982-91.
- Das MK, Suradi H, Maskoun W, Michael MA, Shen C et al. (2008) Fragmented wide QRS on a 12-lead ECG: a sign of myocardial scar and poor prognosis. Circ Arrhythm Electrophysiol 1: 258-68.
- Narayanan K, Zhang L, Kim C, Uy-Evanado A, Teodorescu C et al. (2015) QRS fragmentation and sudden cardiac death in the obese and overweight. J Am Heart Assoc 4: e001654.
- Das MK, Khan B, Jacob S, Kumar A, Mahenthiran J (2006) Significance of a fragmented QRS complex versus a Q wave in patients with coronary artery disease. Circulation 113: 2495-501.
- Flowers NC, Horan LG, Thomas JR, Tolleson WJ (1969) The anatomic basis for high-frequency components in the electrocardiogram. Circulation 39: 531-9.
- Dural M, Demir L, Babayiğit E, Junushova B, Mert KU et al. (2019) Fragmented QRS formation and its predictors in patients with breast cancer receiving anthracycline-based chemotherapy. J Electrocardiol 54: 5-9.
- Adar A, Canyılmaz E, Kiris A, Ilter A, Serdar L et al. (2015) Radiotherapy Induces Development of Fragmented QRS in Patients with Breast Cancer. Breast Care (Basel) 10: 277-80.
- Chen Z, Lu K, Zhou L, Liu D, Li X et al. (2020) Electrocardiographic characteristics of diffuse large B-cell lymphoma patients treated with anthracycline-based chemotherapy. J Electrocardiol 60: 195-9.
FIGURE1
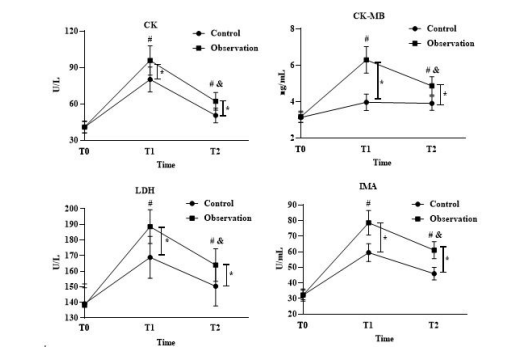
Figure 1: Comparison of myocardial enzyme indexes of both groups. * P < 0.05, compared with the CG; # P < 0.05, compared with T0; & P < 0.05, compared to T1
FIGURE2
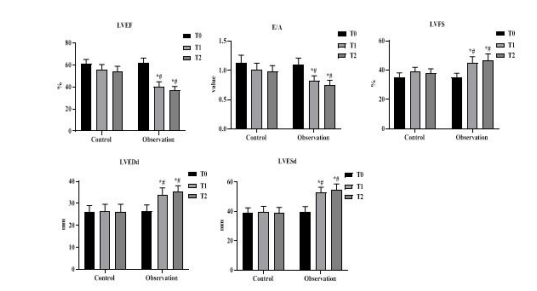
Figure 2: Comparison of echocardiographic indicators between the two groups. * P < 0.05, compared with the CG; # P < 0.05, compared to T0
FIGURE3a
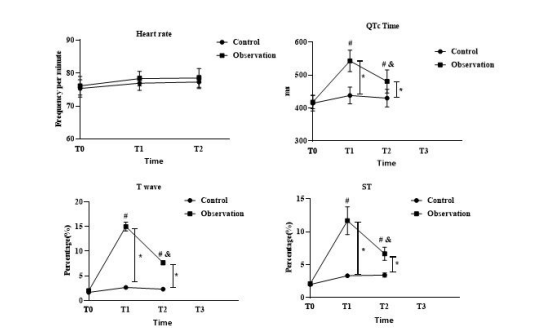
Figure 3: Comparison of electrocardiogram indexes between the two groups. *P < 0.05, compared with the CG; # P < 0.05, compared with T0; & P < 0.05, compared to T1
Tables at a glance
Figures at a glance