Efficacy of Epigallocatechin-3-Gallate in Treating Radiation Recall Pneumonitis after COVID-19 Infection for a Patient with Esophageal Cancer
Received Date:May 14, 2023 Accepted Date: June 14, 2023 Published Date:June 17, 2023
doi: 10.17303/jocr.2023.4.105
Citation: Hanxi Zhao, Xiaolin Li, Fang Gao, Hong Zhao, Ligang Xing, Peng Xie (2023) Efficacy of Epigallocatechin-3-Gallate in Treating Radiation Recall Pneumonitis after COVID-19 Infection for a Patient with Esophageal Cancer. JJ Oncol Clin Res 4:1-5
Abstract
A tumor patient with recurrent esophageal cancer 9 years after radiation therapy was admitted to our oncology center. This patient was also diagnosed with COVID-19 infection without symptoms such as chest tightness. A CT scan showed that the patient had pneumonia in the lung that was consistent with the shape of the radiation field 9 years earlier. A diagnosis of radiation recall pneumonia was considered.
Esophageal squamous cell carcinoma is still a lethal disease with high incidence in Asian countries [1]. Its pathogenesis is relatively complex, mainly including smoking, heavy drinking, nitrosamines, mycotoxins, gastroesophageal reflux, Barrett's esophagus diseases [1], etc. At present, the standard treatment for cervical and upper thoracic esophageal squamous cell carcinoma is still synchronous radiotherapy and chemotherapy, but its 3-year survival rate is still only about 40% [2]. Radiation pneumonitis may occur after radiotherapy, and what is more peculiar is that some patients will develop radiation recall pneumonia [3] (RRP). The term RRP is an ancient concept, which was first reported by D’Angio [4]. RRP is described as an unpredictable acute inflammatory reaction within the previously irradiated lung site during the administration of systematic therapy after radiotherapy. Since the recognition of the existence of RRP, multiple studies have reported RRP caused by chemotherapy, target therapy and even immunotherapy [3]. Typical symptoms of RRP include a dry cough, shortness of breath (with or without hypoxemia), chest tightness, chest pain, and low fever [3]. CT scan findings of RRP are ground glass opacities, diffuse infiltration, or patchy consolidation, and the extent of the lesion usually corresponds to the shape and size of the radiation field for radiotherapy treatment [3]. RRP may occurred months to years after radiation therapy. The COVID-19 pandemic has brought new challenges to cancer patients. Because these patients are usually accompanied by decreased immunity and may have undergone a variety of anti-tumor treatments.
Keywords: EGCG; Radiation Recall Pneumonitis; COVID-19
Introduction
Here we reported a 75-year-old man who had not been previously vaccinated against COVID-19. Nine years after the previous radiotherapy, the patient was infected with COVID-19 (diagnosed by antigen positive), and now the follow-up CT showed pneumonitis, which was suspected as radiation recall pneumonitis (RRP).
The patient was admitted to the hospital due to "back pain" in March 2014. Gastroscopy showed "rough erosion of the esophagus 21-25cm from the incisors, and a large sheet of staining area after iodine staining. The biopsy was taken, and the texture was soft.” Endoscopic ultrasonography: "21-25cm esophageal lesions with thickened mucosa, the thickest was 3.1cm, and the boundary between the lesion and the submucosa was not clear, and the boundary between the lesion and the muscularis propria was clear. Microscopic diagnosis: early esophageal cancer". Pathological showed: "(21-25cm esophagus) squamous cell carcinoma in situ, focal early invasion and lamina propria ". CT scan on March 11, 2014 showed that there was no clear thickening and abnormal enhancement of the wall of each segment of the esophagus. No enlarged lymph nodes were found bilaterally in the hilum and mediastinum. Small lymph nodes, less than 0.5cm in short diameter, were seen on the left supraclavicular region. There was no thickening of the pleura bilaterally. No pleural effusions were found bilaterally. CT scan showed: No definite thickening of the wall of each segment of the esophagus. Radiotherapy was given to the upper thoracic esophageal cancer on March, 2014, 1.8Gy/ fraction, a total of 33 fractions, DT=59.4 Gy. There was no disease recurrence or progression or pneumonitis during routine follow-up CT scan from the end of radiotherapy to February 16, 2023.
In December 2022, the patient tested positive for COVID-19 nucleic acid. No fever, chest tightness, suffocation, chills, palpitation and other symptoms. In January 2023, the patient developed abdominal fullness and discomfort, and the gastroscope showed: "The mucosa showed granular changes with slight eminence 25cm of esophagus, and biopsy was taken". Microscopic diagnosis: esophageal carcinoma. Biopsy pathology showed "esophageal squamous cell carcinoma". CT scan on February 16, 2023 showed: "1. The esophageal wall in the middle and upper part of the chest is slightly thick, please combine with endoscopic pathological examination; Inflammation of the upper lobe of the left lung; 3. Right superior apical segment fibrous foci." The patient was hospitalized in our Radiation Therapy Center. The data of radiotherapy plan on March 12, 2014 were retrieved from the computer and compared with the CT scan images of the patient on February 16, 2023. After comparative analysis, we found that the distribution of pneumonia in the patient was basically consistent with the shape of the radiation field after previous radiotherapy. IL-6, Ferritin, hsCRP and PCT were all negative. The patient was diagnosed with pneumonia, especially suspected RRP.
His pneumonia was improved with an aerosol EGCG saline solution and oxygen therapy for 7 days. Epigallocatechin-3-gallate (EGCG), the major and most highly bioactive constituent in green tea, is responsible for its biochemical and pharmacological effects. We performed a double-blind, placebo-controlled, Phase 2 randomized clinical trial of EGCG in preventing dermatitis in patients with breast cancer receiving postoperative radiotherapy [5]. In this randomized clinical trial, prophylactic use of EGCG solution significantly reduced the incidence and severity of RID in patients receiving adjuvant radiotherapy for breast cancer [5]. It has the potential to become a new choice of skin care for patients receiving radiotherapy [5]. Thus, based on the potent anti-inflammatory antioxidant effect of EGCG, we applied for a clinical trial of EGCG in the treatment of covid-19-induced pneumonia, which is still enrolling. This patient, who was also treated with nebulization of EGCG, was pre-experimental in the study, and this patient gave written informed consent, which was approved by the ethics committee of our study center.
CT scan on February 27, 2023: “local esophageal wall thickened slightly in the middle and upper chest, and the outer membrane surface was clear, which was considered esophageal cancer. No obvious enlarged lymph nodes were observed in mediastinum, hilum of lung and bilateral clavicle. There was a little inflammation in the upper lobe of the left lung, which was significantly improved compared with the previous CT scan.” After the patient recovered from RRP, our cancer center gave the patient esophagoscopy and placed titanium clips at the lesion for tumor position marking. Patients were given concurrent chemoradiotherapy. The patient developed grade I acute radiation esophagitis and grade I acute radiation dermatitis during concurrent chemoradiotherapy. The post-treatment follow-up of this patient is still ongoing
Discussion
Several studies have reported RRP caused or suspected to be caused by COVID-19 infection or COVID-19 vaccine injection. Three cases of potential COVID-19 vaccination-induced RRP have been documented, in which two of these patients were treated with dexamethasone and one patient recovered without treatment. Time intervals from radiotherapy were 6 months to 12 months [6-8]. Richard Blake Ross [9] et al reported a radiation recall skin reaction began with the onset of upper respiratory symptoms confirmed to be COVID-19 infection. The extent of these skin reactions correlated anatomically with the radiation dose gradient 7 years earlier, with necrosis of the skin tissue in the area that received the greatest dose. We carefully compared the extent and shape of the radiation field of the patient's radiotherapy 9 years ago and found that the extent of pneumonia was consistent with that of the current follow-up CT scan. It is different from the classic subpleural pneumonia caused by COVID-19, so it may be RRP. However, there is no report of RRP for such a long time, so our research group summarized and reported the data of this patient. The patient had no symptoms associated with pneumonia and was only found to have pneumonia on a CT scan during a follow-up visit for esophageal cancer. After 7 days of nebulization and oxygen therapy, the patient's CT scan showed significant absorption of pneumonia. This provides an opportunity for the treatment of recurrent esophageal cancer (including re-radiotherapy, chemotherapy, etc.).
The pandemic of coronavirus disease 2019 (COVID-19) has raised new challenges for retreatment of cancer patients who have previously received radiation therapy. Careful evaluation of the inflammatory response to COVID-19 is needed in order to provide patients with more rational treatment modalities
- Fang Liang Huang, Sheng Jie Yu (2018) Esophageal cancer: Risk factors, genetic association, and treatment. Asian J Surg 41: 210-5.
- Steven H Lin, Brian P Hobbs, Vivek Verma et al. (2020) Randomized Phase IIB Trial of Proton Beam Therapy Versus Intensity-Modulated Radiation Therapy for Locally Advanced Esophageal Cancer. J Clin Oncol 38: 1569-79.
- Jan PR, Chang JWC, Wu CE (2022) Radiation Recall Pneumonitis: A Rare Syndrome That Should Be Recognized. Cancers 14: 4642.
- D’Angio GJ (1962) Clinical and biologic studies of actinomycin D and roentgen irradiation. Am J Roentgenol 87: 106-9.
- Hanxi Zhao, Wanqi Zhu, Xianguang Zhao et al. (2022) Efficacy of Epigallocatechin-3-Gallate in Preventing Dermatitis in Patients with Breast Cancer Receiving Postoperative Radiotherapy: A Double-Blind, Placebo-Controlled, Phase 2 Randomized Clinical Trial. JAMA Dermatol 158: 779-86.
- Steber CR, Ponnatapura J, Hughes RT et al. (2021) Rapid Development of Clinically Symptomatic RRP Immediately Following COVID-19 Vaccination. Cureus 13: e14303.
- Hughes NM, Hammer MM, Awad MM et al. (2022) RRP on FDG PET/CT Triggered by COVID-19 Vaccination. Clin Nucl Med 47: 281-3.
- Shinada K, Murakami S, Yoshida D et al. (2022) RRP after COVID-19 vaccination. Thorac. Cancer 13: 144-5.
- Richard Blake Ross, Rachel A Rabinovitch (2022) Radiation recall after COVID-19 infection. Lancet Oncol 23: 197.
FIGURE1
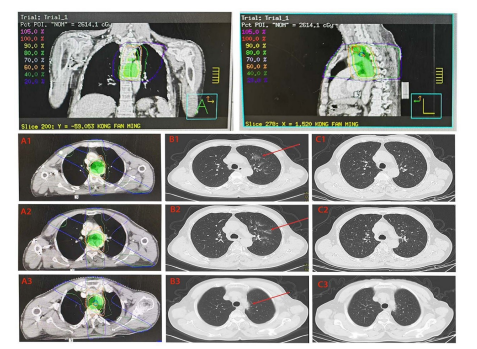
Figure 1: Column A shows the dose line and radiation field distribution direction of patients receiving radiotherapy in March 2014; Column B shows the pneumonia image of the patient's CT scan on February 16, 2023; Column C shows the pneumonia absorption image from the CT scan of the patient on February 27, 2023, after the treatment of pneumonia
Figures at a glance