Prognostic and Predictive Role of Neutrophil/Lymphocyte Ratio in Egyptian Patients with Metastatic Renal Cell Carcinoma (mrcc)
Received Date: August 25, 2023 Accepted Date: September 25, 2023 Published Date: September 28, 2023
doi: 10.17303/jocr.2023.4.201
Citation: Doaa Atef Soliman (2023) Prognostic and Predictive Role of Neutrophil/Lymphocyte Ratio in Egyptian Patients with Metastatic Renal Cell Carcinoma (mrcc). JJ Oncol Clin Res 4: 1-10
Abstract
Background: Treatment and prognosis of patients with mRCC have been improved by advances in the understanding of its molecular pathogenesis. Several prognostic models based on the data of patients with mRCC treated with targeted therapy and immunotherapy have been useful in clinical practice. Serum blood markers related to inflammatory response have been reported to be associated with their prognosis or prediction of therapeutic efficacy.
Study Design and Methodology: Neutrophil/lymphocyte ratio (NLR) was estimated in thirty-two patients with pathological confirmed mRCC as baseline and after two months of systemic therapy. NLR failure was defined as an increase of 3 or more compared to baseline NLR.
Results: Thirty-two patients were enrolled in the study with a mean age 62.7 years with male gender predominance (81.2%). Twenty-seven patients developed clear cell pathological subtype representing (84.4%). Neutrophil/lymphocyte ratio (NLR) mean value baseline was 3.17 and after 2 months of treatment was 5.88. Pazopanib was the commonest received treatment (50%). Six patient (18.8%) had progressed after 2 months of first line of treatment. By the end of the study, only 2 patients were still alive. Mean DFS for patients presented with non-metastatic disease 16 months. The mean OS for all patients was 18 months. NPL difference change before and after 2 months of treatment, revealed that patients with lower NLR change had a statistically significant better OS than patients with high NLR change (p< 0.0001). Cutoff value of NLR 3.6
Conclusion: NLR is a prognostic marker in patients with mRCC with predictive role in response to treatment on survival rate
Keywords: Renal Cell Carcinoma; Neutrophil/Lymphocyte Ratio; Prognosis
Introduction
According to the 2018 GLOBLE data, 403,000 individuals were diagnosed with kidney cancer each year, accounting for 2.2% of all cancers worldwide [1]. It is the sixth most common type of cancer among males and the ninth among females [2]. Approximately one-third of patients with RCC have experienced metastasis by the time of diagnosis [3].
Metastatic renal cell carcinoma (mRCC) is an incurable malignancy, characterized by its resistance to traditional chemotherapy, radiation, and hormonal therapy [4]. There are several globally prognostic models regarding the survival of patients with mRCC [5]. Treatment prediction and prognosis of patients with mRCC have been significantly improved by advances in understanding of its molecular pathogenesis; this understanding has led to the development of targeted therapeutics agents like anti- vascular endothelial growth factor (VEGF), immune checkpoint inhibitors, (PDL-1) or the mammalian target of rapamycin (mTOR) pathways [6].
In recent years, it has become clear that tumor-related inflammatory responses, such as local and systemic inflammation has a major role in the development and progression of malignancies [7]. The alteration of peripheral blood biomarkers, such as the neutrophil-to-lymphocyte ratio (NLR) can represent the systemic inflammatory response in patients. Several studies have demonstrated that the NLR is a potent prognostic biomarker related to worse overall survival (OS) in several tumor types, including mRCC in the pre-immunotherapy era [8]. Normal NLR values in an adult population in good health are between 0.78 and 3.53. NLR failure was defined as an increase of 3 or more compared to baseline NLR [9].
Study Design and Methodology
In this study neutrophil/lymphocyte ratio (NLR) was estimated as a laboratory predictive and prognostic marker in thirty-two patients with mRCC baseline and after two months of systemic therapy. All patients enrolled retrospectively at clinical oncology department at Ain Shams University hospital and El-Araby international Hospital from January 2016 till December 2021. All enrolled patients had assigned a medical consent for research before data collection.
Inclusion Criteria- Pathologically confirmed renal cell carcinoma
- Clinical and radiological proved metastatic disease
- Any age and gender
- Uncontrolled comorbid disease or another malignancy.
- Any immune related disorders or medications (e.g. immunosuppressant)
- Known family history of RCC or other cancer type
All continuous data summarized in terms of mean and standard deviation, while categorical data were summarized in terms of frequencies and percentages. ROC curve was used to estimate the optimal cutoff point that differentiate progressed and non-progressed patients. Also, we used Kaplan-Meier estimator to calculate the overall survival and disease-free survival. Log-rank test was used for comparison. The R software version 4.1.1.was used in this analysis.
Results
Thirty-two patients with mRCC were enrolled in the study with a mean age 62.7 years with male gender predominance (81.2%). Thirty patients had no family history of renal cell carcinoma with 2 unknown information about their family history. Only 14 patients were cigarette smokers. Fifty percent of patients had ECOG performance status 1 at presentation time. Unfortunately, only two patients are still alive by the end of the study (table 1).
Twenty-seven patients developed clear cell pathological subtype representing (84.4%) of all patients. Stage III was the most common presentation stage (40.6%) and equally presented stage II and Stage IV (21.9%). Twenty percent of patients had a single metastatic site, and the commonest site of metastasis was lungs (22 patients) (table 1)
Pazopanib was the commonest received treatment (50%). Regarding patients’ response after 2 months, 19 patients had partial response (59%), 7 patients with stable disease (21.9%) and 6 patients had progressive disease (18.8%). The NLR mean baseline was 3.17 and after 2 months of treatment was 5.88. Six patient (18.8%) had progressed after 2 months of first line of treatment (table 2).
After estimating the difference between NPL before and after 2 months of treatment, cutoff value of NLR with highest sensitivity and specificity was (3.6). The median OS for all studied patients was 18 months (figure 1) but it was 26 months for patients presented with non-metastatic disease (figure2). Regarding DFS for patients presented with non-metastatic disease, the estimated median DFS was 16 months (figure 3).
According to NLR failure definition as increased by 3 or more, patients with lower NLR change had a statistically significant better OS than patients with high NLR change (p< 0.0001) (figure 4).
Also in this study, Patients presented with non-metastatic disease with lower NLR change had a statistically significant better DFS than patients with high NLR change after being metastatic after 2 months of treatment (p< 0.0003) (figure 5).
Discussion
The neutrophil/lymphocyte ratio (NLR) is an easily measurable and inexpensive serum inflammatory marker with many types of malignancies have been correlated to it [10]. In this study neutrophil/lymphocyte ratio (NLR) was estimated as a laboratory predictive and prognostic marker in 32 Egyptian patients were diagnosed as metastatic renal cell carcinoma (either presented with metastatic disease or with early stages and developed metastasis later during the study.
The results of a Chinese meta-analytical study revealed that a high NLR at baseline or pre-therapy was associated with a poor OS (HR, 2.23; 95% CI, 1.84–2.70; p < 0.001). During treatment, a decrease in the NLR was associated with a significantly longer OS (HR, 0.34; 95% CI, 0.20–0.56; p < 0.001) [11]. Dana- Farber Cancer Institute (Boston, MA) receiving IO based therapies were included. The NLR was examined at baseline and 6 weeks later. Higher NLR at baseline and at 6-weeks showed a trend to reduced worse OS and NLR at 6-weeks (p< 0.001) was a stronger prognostic than baseline values and the changed value between baseline and 6 weeks of treatment (p=0.008). These results coincide with our results as patients with lower NLR change had a statistically significant better OS than patients with higher NLR change after 2 months of treatment (p< 0.0001).
In March 2014, a meta-analysis was performed to generate a combination of HRs with 95% CIs for overall survival (OS) and recurrence-free/progress-free survival (RFS/PFS). Results of 15 cohorts containing 3357 patients were included indicated that elevated NLR predicted poorer OS (HR=1.82, 95% CI 1.51 to2.19) and RFS/PFS (HR=2.18, 95% CI 1.75 to 2.71) in patients with RCC. These findings were different when stratified by study region, sample size, therapeutic intervention, types of RCC and study quality. However, it differed significantly by assessment of the cutoff value defining the ‘elevated NLR’ in RFS/PFS (p=0.004) [13].
Conclusion
Elevated NLR indicates a poorer prognosis for patients with mRCC and should be monitored in patients for risk stratification and predictor for treatment response.
Declaration of Interest
Ethics Approval
Oncology ethical committee of Faculty of Medicine in Shams University approval available on demand, Patient consent was taken unless the patient was died as the study is retrospective.
Competing Interests
The author has declared no conflict of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-- for-profit sectors.
Authors Contribution
Single author
- Padala SA, Barsouk A, Thandra KC, Saginala K, Mohammed A, Vakiti A. et al. (2020) Epidemiology of Renal Cell Carcinoma. World J Oncol 11: 79-87.
- Siegel RL, Miller KD, Fuchs HE, Jemal A (2021) Cancer Statistics. CA: Cancer J Clin 71:7-33.
- Bianchi M, Sun M, Jeldres C, Shariat SF, Trinh QD, Briganti A. et al. (2012) Distribution of Metastatic Sites in Renal Cell Carcinoma: A Population-Based Analysis. Ann Oncol Off J Eur Soc Med Oncol 23: 973-80.
- Oudard S, George D, Medioni J, Motzer R (2007) Treatment options in renal cell carcinoma: past, present, and future. Ann Oncol 18: 25-31.
- Shinohara N, Nonomura K, Abe T, Takashige Abe, Satoru Maruyama et al. (2012) A new prognostic classification for overall survival in Asian patients with previously untreated metastatic renal cell carcinoma. Cancer Sci 103: 695-700.
- Choueiri TK, Motzer RJ (2017) Systemic therapy for metastatic renal-cell carcinoma. N Engl J Med 376: 354-66.
- Diakos CI, Charles KA, McMillan DC, Clarke SJ (2014) Cancer-Related Inflammation and Treatment Effectiveness. Lancet Oncol 15: e493-503
- Guthrie GJ, Charles KA, Roxburgh CS, Horgan PG, McMillan DC, Clarke SJ (2013) The Systemic Inflammation-Based Neutrophil-Lymphocyte Ratio: Experience in Patients with Cancer. Crit Rev Oncol/Hematol 88: 218-30.
- Basu A, Phone A, Bice T, Sweeney P, Acharya L, Suri Y. et al. (2021) Change in neutrophil to lymphocyte ratio (NLR) as a predictor of treatment failure in renal cell carcinoma patients: Analysis of the IROC (Investigating RCC Outcomes) cohort. Genitourinary Cancers Symposium. Journal of Clinical Oncology 39: 344-4.
- Ishizuka M, Nagata H, Takagi K, Iwasaki Y, Kubota K (2013) Combination of platelet count and neutrophil to lymphocyte ratio is a useful predictor of postoperative survival in patients with colorectal cancer. Br J Cancer 109: 401-7.
- Chen Xi, Meng Fa and Jiang Ri (2021) Neutrophil-- to-Lymphocyte Ratio as a Prognostic Biomarker for Patients with Metastatic Renal Cell Carcinoma Treated with Immune Checkpoint Inhibitors: A Systematic Review and Meta-Analysis. Front. Oncol 11: 746976
- Lalani A-K A, Xie W, Martini DJ, McGregor BA, Harshman LC, Choueiri TK et al. (2018) Change in neutrophil-- to-lymphocyte ratio (NLR) in response to immune checkpoint blockade for metastatic renal cell carcinoma (mRCC). J Immunother Cancer 6: 5
- Kaimin Hu, Lixia Lou, Juan Ye, Suzhan Zhang (2015) Prognostic role of the neutrophil–lymphocyte ratio in renal cell carcinoma: a meta-analysis. BMJ Open 5: e006404
FIGURE 1
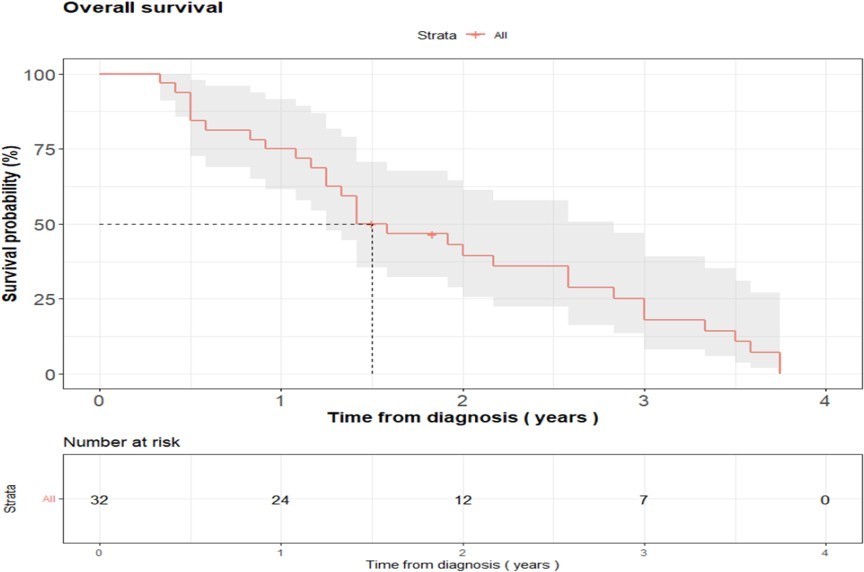
Figure 1: OS for all studied patients with metastatic RCC
FIGURE 2
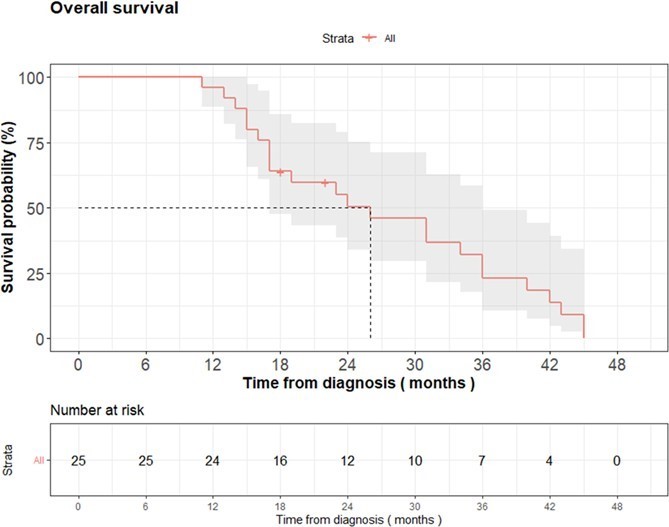
Figure 2: OS for patients presented with non-metastatic RCC
FIGURE 3
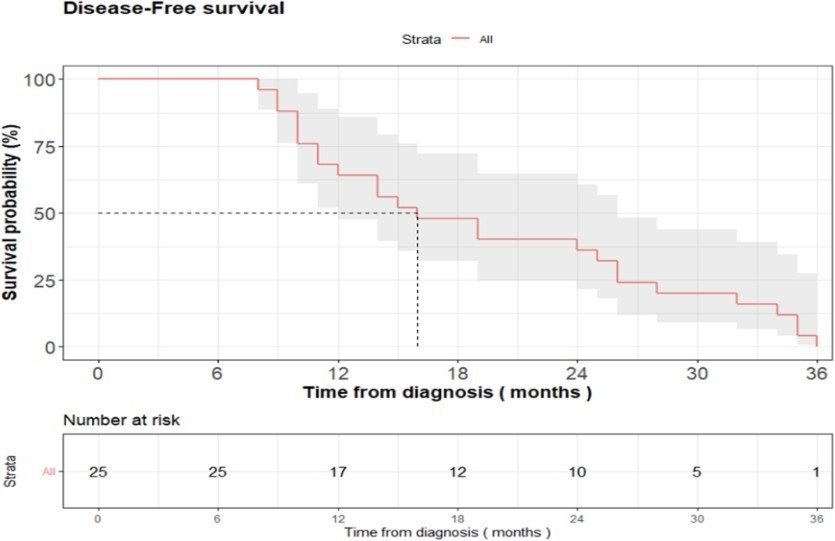
Figure 3: DFS for patient presented with non-metastatic disease
FIGURE 4
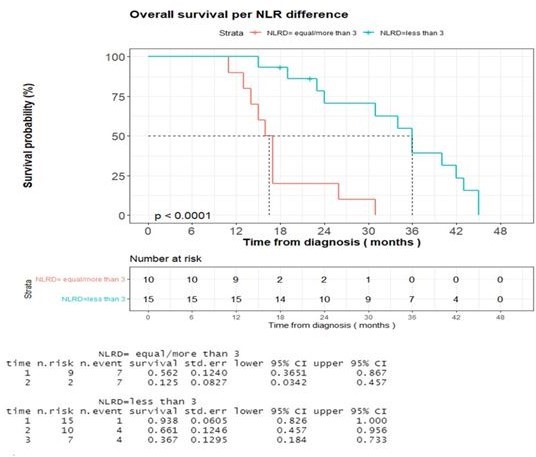
Figure 4: Impact of difference NLR between Baseline and post-treatment on OS in metastatic RCC
FIGURE 5
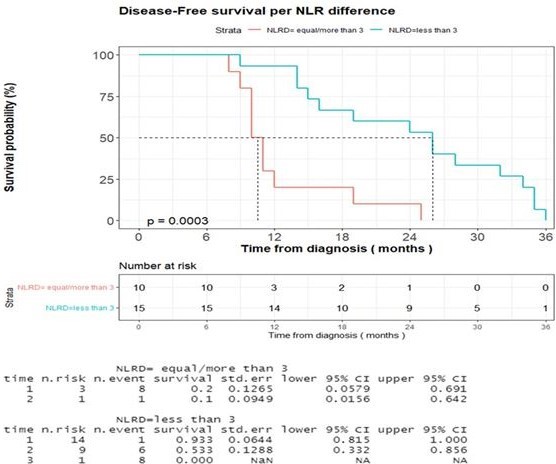
Figure 5: Impact of difference NLR between Baseline and post-treatment on DFS in previously non- metastatic RCC
Tables at a glance
Figures at a glance