The Effect of Vitamin D and Calcium Supplementation on Letrozole-Induced Musculoskeletal Side Effects in Egyptian Patients with Breast Cancer
Received Date: November 26, 2023 Accepted Date: December 26, 2023 Published Date: December 29, 2023
doi: 10.17303/jocr.2023.4.204
Citation: Mai A. Hamouda, Sahar K. Hegazy, Rasha A. Khedr, Tarek M. Mostafa (2023) The Effect of Vitamin D and Calcium Supplementation on Letrozole-Induced Musculoskeletal Side Effects in Egyptian Patients with Breast Cancer. JJ Oncol Clin Res 4: 1-16
Abstract
Background and Aim: Vitamin D deficiency and insufficiency may contribute to musculoskeletal complications observed in patients receiving letrozole. This study aimed at assessing the effects of vitamin D3/calcium supplementation on letrozole-related vitamin D deficiency and musculoskeletal complications.
Methods: In this randomized controlled parallel study, forty postmenopausal estrogen receptor positive patients with breast cancer who received letrozole for six months were randomized into 2 groups; group 1 (the control group; n=20) which received letrozole 2.5 mg daily for 6 months, and group 2 (the vitamin D3/calcium group; n=20) which received letrozole 2.5 mg daily in addition to 2000 IU vitamin D3 and 1000 mg of calcium daily for 6 months. At baseline, 3 and 6 months after intervention, serum concentration of 25-hydroxy vitamin D, calcium, phosphorous, alkaline phosphatase (ALP), osteocalcin, and intact parathyroid hormone (PTH) were assayed. Additionally, dual-energy X-ray absorptiometry (DXA), the standard health assessment questionnaire and pain scale were implicated to assess bone mineral density, the patients' disability and pain. Data were analyzed by paired t-test, unpaired t-test, and Chi-Square test.
Results: Six months after intervention and as compared to the control group, vitamin D3/calcium supplementation significantly increased the serum concentrations of vitamin D (p< 0.001), ionized and total calcium (p< 0.001) and phosphorous (p< 0.001), which was associated with significant decline in the concentrations of intact-PTH (p=0.001), and osteocalcin (p=0.028). Additionally, vitamin D3/calcium supplementation improved bone mineral density (p< 0.001), patients' disability and patients' pain (p< 0.001 and p=0.005 respectively).
Conclusion: Vitamin D3/calcium supplementation significantly improved serum vitamin D concentrations and decreased letrozole-related musculoskeletal complications.
Keywords: Breast Cancer; Letrozole; Vitamin D3; Bone Mineral Density; Disability; Musculoskeletal Complications
Introduction
Breast cancer is the most frequent cancer worldwide and represents the second leading cause of death among women, after lung cancer [1]. Vitamin D deficiency has been implicated in a wide variety of cancers [2]. The level of 25-hydroxy vitamin D (25OHD), the major circulating metabolite, provides a direct assessment of vitamin D status in- vivo [3].
Aromatase inhibitors (AI) markedly suppress plasma estrogen levels in postmenopausal women through inhibition of aromatase enzyme responsible for the production of estrogen from androgenic substrates [4]. Letrozole is a third generation aromatase inhibitor which has fewer complications including fatigue and musculoskeletal symptoms which in turn causes negative impact on patient’s adherence to letrozole [5]. Unlike tamoxifen, aromatase inhibitors have no partial estrogen agonist activity [6]. Third generation aromatase inhibitors are more potent and more selective than first and second generation aromatase inhibitors [5]. Third generation aromatase inhibitors are commonly used for estrogen receptor-positive postmenopausal patients with breast cancer and in patients who showed treatment failure to tamoxifen or other hormonal therapies [5].
Severe vitamin D insufficiency can lead to defective bone mineralization and osteomalacia in adults. In less severe vitamin D insufficiency, the decrease in intestinal calcium absorption and the subsequent hypocalcaemia result in an increase in serum parathormone level which stimulates bone remodeling and contributes to osteoporosis in elderly patients [7]. Joint pain, stiffness, muscle pain and muscular weakness are the most common musculoskeletal symptoms [3-5]. Earlier studies demonstrated that, these musculoskeletal symptoms could be attributed to the reduction in the estrogen level and to letrozole induced vitamin D deficiency [8].
In this context, the aforementioned information encourages us to run this study which aimed at assessing the effects of vitamin D3/calcium supplementation on letrozole-related musculoskeletal side effects.
Patients and Methods
Study Design, Study Population and Ethical Approval
This study was designed as a randomized, controlled parallel clinical study. Forty postmenopausal estrogen receptor positive patients with stage II and stage III breast cancer who received letrozole for six months were included in the study. The study was conducted in out-patient Oncology Clinic, Tanta Cancer Center, Tanta, Egypt. The study was approved by the National Research Ethics Committee of Tanta University with an approval Code (35211/1/22). The study was registered as clinical trial at ClinicalTrials.gov with ID: NCT05523609. Written informed consent was obtained from eligible patients. The inclusion criteria included female patients with biopsy-confirmed diagnosis with stage II and stage III breast cancer according to the American Joint Committee on Cancer (TNM staging system) [9]. Women with age ≥ 50 years old and with positive hormonal receptors were included. The inclusion criteria also involved aromatase inhibitor treatment naive postmenopausal women who were assigned to receive hormonal therapy with aromatase inhibitor. Postmenopausal is defined as age ≥55 years old and one year or more of amenorrhea or age < 55 years old and one year or more of amenorrhea, with an estradiol level less than 20 pg/ml [10]. Overweight patients (BMI ≥ 25 kg/m2 and < 30 kg/m2), and obese patients (BMI ≥ 30 kg/m2) were also included in the study. The exclusion criteria were patients with bone metastasis, patients with a history of renal stones, patients with serum calcium >11mg/L, patients with renal insufficiency, patients on steroid hormone replacement therapy, patients with secondary malignancy, women who were treated with luteinizing hormone-releasing hormone agonists (LHRH), and women with cardiovascular disease. The participants were randomized by simple randomization using sealed envelope method into two groups; group 1(the control group; n= 20) which received letrozole 2.5 mg daily for 6 months and group 2 (Vitamin D3/Calcium supplementation group; n=20) which received letrozole 2.5 mg daily in addition to 2000 IU vitamin D3 and 1000 mg of calcium daily for 6 months.
All participants enrolled in this study were with stage II and stage III breast cancer with lymph node involvement. The participants were enrolled in the study after completing their treatment with chemotherapy/surgery/radiotherapy. The chemotherapy used for all participants was FEC regimen (Fluorouracil (500mg/m2), Epirubicin (100mg/m2), and Cyclophosphamide (500 mg/m2)) system for 3 cycles (cycle every 21 days) followed by paclitaxel (175 mg/m2) for 3 cycles (9 weeks), or FAC regimen (Fluorouracil (500mg/m2), Adriamycin (50 mg/m2), and Cyclophosphamide (500 mg/m2)) for 3 cycles (cycle every 21 days) followed by paclitaxel for 3 cycles (9 weeks). After completing the chemotherapy cycles, all patients were submitted to surgery by modified radical mastectomy (MRM) or breast-- conserving surgery (BCS). Within one month after surgery, all women were received a total of 16 sessions of radio-therapy (5 sessions every week) and started on their hormonal therapy (letrozole 2.5 mg/day). There were 9 patients with positive human epidermal growth factor receptor 2 (HER2) in the two study groups (5 patients in the control group, 4 patients in vitamin D3/calcium supplementation group). The immunohistochemistry (IHC) revealed that, those 9 women were with low HER2 (7women were positive 1 and 2 women were positive 2). The confirmatory analysis through fluorescence in-situ hybridization (FISH) revealed negative HER2 (HER2-negative) for all the 9 women. Therefore, those 9 women were not candidates for targeted therapy [11,12].
Measurements
Demographic, Clinical, and Anthropometric Data
At baseline, age, medication history, stage of the disease, and receptor status were collected. Weight and height were measured to the nearest kilogram (kg) and centimeter (cm) and then, the body mass index (BMI) was calculated using the following equation: BMI = Weight (kg)/ height2(m).
Blood Samples Collection and Biochemical Measurements
At baseline, three and six months after the intervention, 5 ml of venous blood was withdrawn from the antecubital vein of every participant after overnight fasting (10- 12 hour fasting period) between 8:30 and 10:30 am.
Blood samples were transferred slowly into a plain test tube then allowed to clot, centrifuged at 3000 rpm for 10 min (Hettich Zentrifugen EBA 20). The sera were collected and divided into two portions; the first portion was used for immediate determination of serum calcium (OCPCOrtho-cresolphthalein complexone method), serum phosphorus (Phosphomolybdate method) and serum alkaline phosphatase (ALP). The second portion of the serum was stored at −80 °C for further analysis of serum levels of 25 (OH) vitamin D (ELISA kit, Calbiotech Biotechnology Company, USA,Catalogue No: VD220B),Intact-parathyroid hormone "PTH" (ELISA kit, Calbiotech Biotechnology Company, USA Catalogue No: PT311T) and Osteocalcin (ElISA Kit, Sunred BioTechnology Company, China, Catalogue No:201-12-1556).
Assessment of Bone Mineral Density
Bone mineral density for all participants was assessed at baseline and after 24 weeks using dual-energy Xray absorptiometry (DXA).
Clinical Assessment
Health Assessment Questionnaire-II (HAQ-II) was completed for assessing the disability of the study participants at baseline and 3 and 6 months after intervention. Health Assessment Questionnaire-II compromises a set of ten standardized questions which was applied to assess the patients' disability that could be attributed to musculoskeletal symptoms. The higher HAQ-II scores the greater degree of disability [13]. In addition, pain score was also assessed using the Brief pain inventory-short form (BPI-SF). The pain score was assessed at baseline and on biweekly basis throughout the study period to assess the pain related to aromatase inhibitors induced arthralgia
Primary and Secondary Outcomes
The primary outcome was the change in biological markers. The secondary outcome was the change in bone mineral density and health assessment questionnaire.
Sample Size Calculation
The sample size calculation was based on a previous study which was conducted in breast cancer patients received aromatase inhibitor. The total sample size used in this former study was 38 patients [14]. With 0.05 α error, 80% power and an attrition rate of 5%, our sample size was 40 patients (20 patients in each group).
Statistical Analysis
All statistical analysis were carried out using IBM-SPSS statistical package version 24.0 (SPSS Inc.: USA 2016). The data were tested for normality using ShapiroWilk test. Paired t-test was used to compare the results at baseline and after treatment within the same group. Unpaired t-test was applied to compare between the means of the two groups. Chi-Square test was used to analyze categorical data. Correlation between variables was evaluated using Pearson correlation coefficient. The data are expressed as the mean ± the standard deviation, range, number and percent. The significance level will be set at p< 0.05.
Results
The total number of encounters with postmenopausal estrogen receptor positive women with breast cancer was 55 patients. Among those, 4 women declined to participate, 2 women had renal insufficiency, 3 women were on steroid, and one woman had secondary malignancy. Therefore, 45 women were randomized into two groups; group 1 or control group (n=22) and group 2 or vitamin D3/calcium supplementation group (n=23). During the treatment period, 5 patients were dropped-out in both groups (2 patients in the control group (data was missed (n=1) and death (n=1)), and 3 patients in the vitamin D3/calcium supplementation group data was missed (n=1), regimen had changed (n=1) and renal stone had developed (n=1)). In this context, the final analysis included 40 patients (20 patients in each group). The flow- chart of the study participants is illustrated in figure (1).
Baseline Characteristics
At baseline, there was non-significant difference between the two study groups (p>0.05) regarding demographic and anthropometric data (age, weight, height and body mass index), hormonal receptor status, stage of the disease, chemotherapy used, type of surgery and ejection fraction (EF) as shown in table (1). At baseline, 15% of patients (6 patients) were deficient in vitamin D (< 10 ng/ml), 80% (32 patient) were insufficient (10-30 ng/ml), and 5% (2 patients) were sufficient in 25-hydroxy vitamin D concentrations.
Effect of Intervention on Biochemical Parameters
At baseline, there was non-significant difference between the two study groups regarding the assessed biochemical parameters (p>0.05) as demonstrated in table (2).
As compared to baseline data, 3 and 6 months after treatment, the control group showed gradual and significant decrease in the serum level of 25(OH) Vitamin D (27.28±8.08 ng/ml versus 25.788±7.765 ng/ml; p1< 0.001 and 27.28±8.080 ng/ml versus 22.978±7.305 ng/ml; p2 < 0.001 respectively), ionized calcium (4.87±0.5 mg/dl versus 4.48±0.586 mg/dl; p1< 0.001 and 4.87±0.5 mg/dl versus 4.175±0.506 mg/dl; p2< 0.001 respectively), total calcium (9.395±0.613 mg/dl versus 8.855±0.728 mg/dl; p1< 0.001 and 9.395±0.613 mg/dl versus 7.595±0.913 mg/dl; p2< 0.001 respectively), and phosphorus (4.580±0.514 mg/dl versus 4.05±0.562 mg/dl; p1< 0.001 and 4.58±0.514 mg/dl versus 3.78±0.542 mg/dl; p2< 0.001 respectively). Furthermore and compared to baseline data, 3 and 6 months after treatment, the control group showed significant increase in the serum level of alkaline phosphatase (78.1±22.143 U/L versus 82.55±23.754 U/L; p1< 0.001 and 78.1±22.143 U/L versus 86.95±24.903 U/L; p2< 0.001 respectively), osteocalcin (29.13±15.082 ng/ml versus 31.57±15.816 ng/ml; p1< 0.001 and 29.13±15.082 ng/ml versus 34.225±16.018 ng/ml; p2< 0.001 respectively) and intact parathyroid hormone level (39.9±21.138 pg/ml versus 45.45±20.009 pg/ml; p1< 0.001 and 39.9±21.138 pg/ml versus 50.7±20.515 pg/ml; p2< 0.001 respectively) as postulated in table (3).
On the other hand and as compared to baseline data, 3 and 6 months after treatment, vitamin D3/calcium supplementation group showed significant elevation in serum concentration of 25(OH) vitamin D level (26.38±9.245 ng/ml versus 29.661±8.765 ng/ml; p3< 0.001 and 26.38±9.245 ng/ml versus 33.126±7.533 ng/ml; p4< 0.001 respectively), ionized calcium (4.7±0.51 mg/dl versus 4.84±0.5 mg/dl ; p3< 0.001 and 4.7±0.51 mg/dl versus 5.29±0.192; p4< 0.001 respectively), total calcium (9.281±0.679 mg/dl versus 9.554±0.476; p3=0.008 and 9.281±0.679 mg/dl versus 9.9±0.242 mg/dl; p4< 0.001 respectively), and phosphorus 4.55±0.476 mg/dl versus 4.7±0.51 mg/dl; p3< 0.001 and 4.55±0.476 mg/dl versus 4.84±0.5 mg/dl; p4< 0.001 respectively which was associated with significant decline in the serum levels of alkaline phosphatase (85.9±24.138 U/L versus 82.9±23.461 U/L; p3=0.001 and 85.9±24.138 U/L versus 80.3±24.336 U/L; p4< 0.001 respectively), osteocalcin (25.053.13±17.964 ng/ml versus 23.445±16.873 ng/ml; p3< 0.001 and 25.053.13±17.964 ng/ml versus 22.43± 16.615 ng/ml; p4< 0.001 respectively), and IPTH (39.5±9.191 pg/ml versus 37.05±8.935 pg/ml; p3< 0.001 and 39.5±9.191 pg/ml versus 33.2±8.661 pg/ml; p4< 0.001 respectively).
The comparison between the two groups revealed that, 6 months after intervention and in comparison with the control group, vitamin D3/calcium supplementation group showed significant elevation in the serum level of 25(OH) Vitamin D (33.126±7.533 ng/ml versus 22.978±7.305 ng/ml; p6˂0.001; effect size= 1.36). In addition, 3 and 6 months after intervention and as compared to the control group vitamin D3/calcium supplementation group showed significant elevation in ionized calcium (4.840±0.5 mg/dl versus 4.48±0.586 mg/dl; p5=0.043 and 5.29±0.192 mg/dl versus 4.175±0.506 mg/dl; p6˂0.001; effect size= 2.91 respectively), total calcium (9.554±0.476 mg/dl versus 8.855±0.728 mg/dl; p5=0.001; and 9.9±0.242 mg/dl versus 7.595±0.913 mg/dl; p6˂0.001; effect size= 3.45 respectively) and phosphorus (4.7±0.51 mg/dl versus 4.05±0.562 mg/dl; p5˂0.001 and 4.84±0.5 mg/dl versus 3.78±0.542 mg/dl; p6˂0.001 respectively). In contrast 6 months after intervention and as compared to the control group, the vitamin D3/calcium supplementation group showed significant decline in the serum levels of osteocalcin (22.43±16.615 ng/ml versus 34.225±16.018 ng/ml; p6=0.028; effect size= 0.72) and I-PTH (33.2±8.661 pg/ml versus 50.7±20.515 pg/ml; p6=0.001; effect size= 1.11). However, 3 and 6 months after intervention the vitamin D3/calcium supplementation group showed non-significant decline in the serum level of alkaline phosphatase when compared to the control group (p5=0.963 and p6=0.398 respectively) as postulated in table (4).
Effect of Intervention on Bone Mineral Density
At baseline, there was non-significant difference between the control group and the vitamin D3/calcium supplementation group concerning bone mineral density (-1.935 ± 0.517 versus -1.830 ± 0.487; p= 0.513). As compared to baseline data, 6 months after treatment the control group showed significant decline in bone mineral density (-1.935 ± 0.517 versus -2.240 ± 0.426; p˂0.001). On the other hand and compared to baseline data, 6 months after treatment vitamin D3/calcium supplementation group showed significant improvement in bone mineral density (-1.830 ± 0.487 versus -1.605 ± 0.472, p˂0.001).
Six months after intervention and as compared to the control group, vitamin D3/calcium supplementation group showed significant improvement in bone mineral density (-1.605 ± 0.472 versus -2.240 ± 0.426; p˂0.001; effect size= 1.41) as figure (2).
Effect of Intervention on Patients' Disability and Pain
At baseline, there was non-significant difference between the control group and the vitamin D3/calcium supplementation group concerning HAQ-II total score (45.45±1.232 versus 45.875±0.943; p=0.228). As compared to baseline data, 3 and 6 months after treatment the control group showed significant decrease in HAQ-II total score (45.45±1.232 versus 38.1±2.128; p1˂0.001 and 45.45±1.232 versus 24.05 ±0.833; p2˂0.001 respectively). On the other hand, and compared to baseline data, 3 and 6 months after treatment vitamin D3/calcium supplementation group showed significant decrease in HAQ-II total score (45.875±0.943versus 34.495±2.835; p3 ˂0.001 and 45.875±0.943 versus 18.825±2.971; p4˂0.001 respectively). The comparison between the two groups 3 and 6 months after intervention showed that, as compared to the control group, vitamin D3/calcium supplementation group showed significantly lower HAQ-II total score which indicates less disability (34.495±2.835 versus 38.1±2.128; p5˂0.001 and 18.825±2.971 versus 24.05±0.833; p6˂0.001; effect size= 2.39 respectively) as shown in table (2), (3) and (4).
Concerning pain score, there was non- significant variation in pain score between the two study groups at baseline (0.7± 0.58 versus 0.5 ± 0.76; p=0.435). The pain score tended to be increased in both groups after each week of Letrozole administration. The difference in pain scores between the two groups remained statistically non-significant till the end of the 20th week. By the end the 24th week, vitamin D3/calcium supplementation group showed significantly lower pain scores than the control group (7.3±0.59 versus 6.7±0.64; p6=0.005) as demonstrated in table (2) and table(4).
Correlation Analysis
The Pearson correlation analysis between the bone mineral density (t-score) and the measured biochemical variables for vitamin D3/calcium supplementation group revealed that, vitamin D, ionized calcium, and phosphorous serum levels were positively and significantly correlated with t-score (r=0.036, p=0.001; r= 0.607, p=< 0.001; r=0.599, p=< 0.001and respectively). In contrast alkaline phosphatase, osteocalcin and I-PTH were negatively and significantly correlated with bone mineral density (r=-0.565, p=< 0.001, r=-0.150, p=0.027 and r=-0.405, p=< 0. 001respectively) as postulated in table (5).
Discussion
Breast cancer ranks second among all types of cancer that affect women. About 2.7 million new cases were diagnosed in 2021 [15]. Letrozole, is the most potent non-steroidal aromatase inhibitor (AI) used for the treatment of hormonal receptor positive breast cancer. Letrozole was reported to cause musculoskeletal complications and fatigue which is attributed to vitamin D deficiency and insufficiency [16].
This study aimed at evaluating the effects of vitamin D3/calcium supplementation on letrozole-related vitamin D deficiency and musculoskeletal complications. The dose used of vitamin D3/calcium supplementation during the current study was 2000 IU vitamin D3 and 1000 mg of calcium daily which seems in parallel with a previously reported study [17].
The duration of the current study was 6 months which seems in parallel with a previously reported study [18]. In the present study, the patients' age was ≥55 years old and all patients were overweight and obese subjects. The participants of the current study had low serum 25 (OH) vitamin D concentration. This previous finding comes in accordance with some former studies which demonstrated that, serum 25 (OH) vitamin D concentration tended to be decreased in elderly patients [19] secondary to reduced outdoor activity, food intake, skin synthesis and absorption of vitamin D [20]. Furthermore, it was demonstrated that, obese patients had low concentrations of serum 25 (OH) vitamin D which is attributed to lack of physical activity and sequestration of vitamin D into subcutaneous fat depots [21].
In the control group, there was a decline in serum 25 (OH) vitamin D concentrations throughout the treatment course with letrozole. Previous studies have shown that letrozole decreased estrogen concentration. It was hypothesized that, reduced estrogen concentrations may unmask subclinical vitamin D deficiency since estrogen increases the activity of 1- α hydroxylase, needed for the production of the active form of vitamin D [16,22].
Pre-vitamin D is transported and converted by the liver into 25-hydroxyvitamin D, the major circulating form. Then, 25-hydroxyvitamin D is converted by the kidney into 1,25-dihydroxyvitamin D which represents the active form [23]. Through competing with hepatic cytochrome P450 3A4 system, aromatase inhibitors may attenuate vitamin D metabolism in the liver and subsequently decrease the circulating 25-hydroxyvitamin D [24].
Our result comes in consonance with a previously reported finding demonstrated that patients received letrozole for long time had a low serum concentration of vitamin D [17]. The main function of vitamin D is to maintain calcium and phosphorus balance in the body by allowing calcium and phosphorus absorption from the intestines and kidneys [25]. During vitamin D deficiency, only 10%-15% of calcium and 50%-60% of phosphorus can be absorbed from dietary sources [25]. This could explain the low levels of calcium and phosphorus observed with the control group. This results seems in matching with a previously reported finding postulated that, low concentrations of serum 25 (OH) vitamin D is associated with low concentrations of serum calcium and phosphorus and high concentrations of PTH [26]. Low serum calcium concentration causes an increase in PTH secretion, which in turn stimulates the production of 1,25-dihydroxyvitamin D. Through this mechanism, 1,25-dihydroxyvitamin D is kept at near normal concentrations at the expense of higher serum PTH concentration [27]. In this context, during the current study, vitamin D3 and calcium supplementation resulted in an increase in the concentrations of calcium and phosphorous level which was associated with a significant decrease in the concentrations of parathyroid hormone and alkaline phosphatase serum levels which come in consonance with a previously reported finding [17].
Osteocalcin is considered to be one of the markers for osteoporosis and bone formation [28,29]. Osteocalcin is synthesized in the skeleton by osteoblasts, the cells responsible for the bone formation. Osteocalcin has a high affinity to calcium and a compact calcium dependent α helical conformation, in which the γ-carboxyglutamic acid (Gla) residues binds and promote absorption to hydroxyapatite in bone matrix with subsequent bone mineralization.
Vitamin D deficiency and insufficiency which results in calcium and phosphorous deficiency may lead to decreased formation of hydroxyapatite crystals and reduced bone mineralization. This could justify the observed elevated level of osteocalcin in the control group and its low level in the intervention group during the current study. Our result comes in matching with a previously reported finding demonstrated that, there is an inverse association between vitamin D and osteocalcin [28,29].
During the current study, our data revealed that vitamin D3/calcium supplementation group showed an improvement in bone mineral density (BMD) as compared to the control group. It has been demonstrated that, Vitamin D deficiency and insufficiency have negative impact on osteoblastic activity, matrix ossification, bone mineral density and bone remodeling. Low serum 25 hydroxy vitamin D concentrations is associated with secondary hyperparathyroidism, increased bone turnover and reduced bone mineral density BMD with elevated risk of fractures [30]. Additionally, it was hypothesized that, treatment for 3 months with alendronate + calcium + Vitamin D may be helpful to prevent bone loss, and increasing the bone strength [29,31]. Furthermore it was demonstrated that, vitamin D deficiency is a risk factor for low bone density, increased bone turnover and supplementation with vitamin D appears to suppress bone turnover, possibly mediated by suppressing of parathyroid hormone [32].
After intervention and as compared to the control group, vitamin D3/calcium supplementation group showed significantly lower pain score and health assessment questionnaire (HAQ-II) score meaning that, this group showed less musculoskeletal symptoms. Patients in the control group had low serum 25 (OH) vitamin D concentrations and are more vulnerable to musculoskeletal symptoms as evidenced by their higher pain and HAQ-II scores. These musculoskeletal symptoms may be attributed to the expansion of the collagen matrix that increases the pressure on periosteal surfaces and sensory pain fibers. Furthermore, hypophosphatemia induced by hyperparathyroidism may lead to muscle pain and weakness [33]. Additionally, estrogen deficiency is thought to cause arthritis through its direct effect on joint tissues and through inflammatory pathways and release of inflammatory cytokines including interleukin-6 and through its effect on central and peripheral nociception [24].
This result seems compatible with the results demonstrated by other authors who showed that patients with low 25 (OH) vitamin D concentrations had higher HAQ scores and musculoskeletal symptoms [34].
The points of strength of the current study include its design, the assessment of many biological markers and DXA score, the use of the same brand of letrozole, vitamin D and calcium supplement throughout the study and the relatively good study duration. However, the current study has some limitations including a relatively small sample size, the lack of assessment of estradiol serum level. In this context, future studies are still recommended.
Conclusion
This study aimed at assessing the effects of vitamin D3/calcium supplementation on letrozole-related vitamin D deficiency and musculoskeletal complications. Patients received vitamin D3/calcium supplementation showed significant elevation in the serum concentrations of vitamin D, calcium and phosphorus and significant decline in the serum levels of alkaline phosphatase, parathyroid hormone and osteocalcin. In addition vitamin D3/calcium supplementation resulted in an improvement in bone mineral density (DXAscore) and less pain and musculoskeletal symptoms (HAQII score). Based on the data obtained with the current study, we recommend supplementation of 2000 IU/day vitamin D3 and 1000 mg/day calcium for postmenopausal patients with breast cancer who will be treated with letrozole. However, further detailed studies are still needed.
Consent
Authors declare that, written informed consent was obtained from approving authority for publication of this research.
Ethical Approval
The study was approved by the National Research Ethics Committee of Tanta University with an approval Code (35211/1/22). The study was consistent with the Helsinki Declaration's ethical principles in 1964 and its later amendments.
Acknowledgment
We are grateful to our participants, wishing them full health and rapid recovery. We are thankful to the physicians at Oncology Clinic, Tanta Cancer Center, Tanta, Egypt, for their valuable assistance and co-operation.
Authors' Contribution
Tarek M. Mostafa, Sahar K. Hegazy reviewed the literature and created the study design. Rasha A. Khedr contributed to the conceptualization and eligibility evaluation. Tarek M. Mostafa and Mai A. Hamouda contributed to the samples analysis. Mai A. Hamouda performed the statistical analysis. All authors wrote, reviewed, and approved the final manuscript.
Funding
This current study was self-funded and wasn't funded by any organization, agency, or pharmaceutical company.
Data Availability
All data generated or analyzed during the current study are available from the corresponding author upon reasonable request.
Declarations
Conflict of Interest
There are no conflicts of interest to disclose for any of the authors.
Consent to Participate
All the study participants provided their informed consent since there is no personal data, publication consent is not requested.
ClinicalTrials.gov Identifier
NCT05523609 Retrospectively
- Azamjah N, Soltan-Zadeh Y, Zayeri F (2019) Global Trend of Breast Cancer Mortality Rate: A 25-Year Study. Asian Pac J Cancer Prev. 20: 2015-20.
- Amrein K, Scherkl M, Hoffmann M, Neuwersch-Sommeregger S, Köstenberger M, Tmava Berisha A, et al. (2020) Vitamin D deficiency 2.0: an update on the current status worldwide. Eur J Clin Nutr 74: 1498-513.
- Castillo-Peinado LdlS, Calderon-Santiago M, Herrera-Martínez AD, Leon-Idougourram S, Galvez-Moreno MA, Sanchez-Cano RL, et al. Measuring Vitamin D3 Metabolic Status, Comparison between Vitamin D Deficient and Sufficient Individuals. Separations 9: 141.
- Nahm N, Mee S, Marx G (2018) Efficacy of management strategies for aromatase inhibitor-induced arthralgia in breast cancer patients: a systematic review. Asia Pac J Clin Oncol 14: 374-82.
- Grigorian N, Baumrucker SJ (2022) Aromatase inhibitor-associated musculoskeletal pain: An overview of pathophysiology and treatment modalities. SAGE Open Med 10: 20503121221078722.
- Kunder SK, Arivazhahan A (2021) Hormonal Agents in the Pharmacotherapy of Cancer. In: Paul A, Anandabaskar N, Mathaiyan J, Raj GM, editors. Introduction to Basics of Pharmacology and Toxicology: Volume 2 : Essentials of Systemic Pharmacology: From Principles to Practice. Singapore: Springer Nature Singapore; 2021. p. 1103-10.
- Perera N, Fernando N, Perera R, Jayasekara P, Senevirathne B, Ratnayake W (2020) Metastatic breast cancer spread to peripancreatic lymph nodes causing biliary obstruction. Breast J 26: 511-3.
- Gupta A, Henry NL, Loprinzi CL (2020) Management of Aromatase Inhibitor–Induced Musculoskeletal Symptoms. JCO Oncology Practice 16: 733-9.
- Amin MB, Greene FL, Edge SB, Compton CC, Gershenwald JE, Brookland RK, et al. (2017) The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more "personalized" approach to cancer staging. CA Cancer J Clin 67: 93-9.
- Diorio C, Lemieux J, Provencher L, Hogue JC, Vachon E (2012) Aromatase inhibitors in obese breast cancer patients are not associated with increased plasma estradiol levels. Breast Cancer Res Treat 136: 573-9.
- Wolff AC, Hammond MEH, Allison KH, Harvey BE, Mangu PB, Bartlett JMS, et al. (2018) Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. J Clin Oncol 36: 2105-22.
- Fehrenbacher L, Cecchini RS, Geyer CE, Jr., Rastogi P, Costantino JP, Atkins JN, et al. (2020) NSABP B-47/NRG Oncology Phase III Randomized Trial Comparing Adjuvant Chemotherapy With or Without Trastuzumab in High-Risk Invasive Breast Cancer Negative for HER2 by FISH and With IHC 1+ or 2. J Clin Oncol 38: 444-53.
- Wolfe F, Michaud K, Pincus T (2004) Development and validation of the health assessment questionnaire II: a revised version of the health assessment questionnaire. Arthritis Rheum 50: 3296-305.
- Coscia EB, Sabha M, Gerenutti M, Groppo FC,Bergamaschi CC (2017) Estrone and Estradiol Levels in Breast Cancer Patients Using Anastrozole Are Not Related to Body Mass Index. Rev Bras Ginecol Obstet 39: 14-20.
- Donepudi MS, Kondapalli K, Amos SJ, Venkanteshan P (2014) Breast cancer statistics and markers. J Cancer Res Ther 10: 506-11.
- O'Shaughnessy J (2007) A decade of letrozole: FACE. Breast Cancer Res Treat 105: 67-74.
- Arul Vijaya Vani S, Ananthanarayanan PH, Kadambari D, Harichandrakumar KT, Niranjjan R, Nandeesha H (2016) Effects of vitamin D and calcium supplementation on side effects profile in patients of breast cancer treated with letrozole. Clinica Chimica Acta 459: 53-6.
- Jacot W, Firmin N, Roca L, Topart D, Gallet S, Durigova A, et al. (2016) Impact of a tailored oral vitamin D supplementation regimen on serum 25-hydroxyvitamin D levels in early breast cancer patients: a randomized phase III study. Ann Oncol 27: 1235-41.
- Wiacek M, Zubrzycki IZ, Bojke O, Kim HJ (2013) Menopause and age-driven changes in blood level of fat- and water-soluble vitamins. Climacteric 16: 689-99.
- Boucher BJ (2012) The problems of vitamin d insufficiency in older people. Aging Dis 3: 313-29.
- Vashi PG, Trukova K, Lammersfeld CA, Braun DP, Gupta D (2010) Impact of oral vitamin D supplementation on serum 25-hydroxyvitamin D levels in oncology. Nutr J 9: 60.
- Bhatnagar AS (2007) The discovery and mechanism of action of letrozole. Breast Cancer Res Treat 105: 7-17.
- Erbay E, Mersin S, İbrahimoglu O (2019) Effect of vitamin D on body systems. Health Care Acad J 6: 201-2016.
- Smith IE, Dowsett M (2003) Aromatase inhibitors in breast cancer. N Engl J Med 348: 2431-42.
- TORUN T, CAVUSOGLU H (2018) Vitamin D deficiency rickets and nursing care. J Hacettepe Univ Fac Nurs 5: 169-76.
- Moe SM (2008) Disorders involving calcium, phosphorus, and magnesium. Prim Care 35: 215-37.
- Lips P (2001) Vitamin D deficiency and secondary hyperparathyroidism in the elderly: consequences for bone loss and fractures and therapeutic implications. Endocr Rev 22: 477-501.
- Chidre YV, Shaik A (2017) Association of vitamin D and osteocalcin levels in postmenopausal women with osteoporosis. Int J Reprod Contracept Obstet Gynecol 6: 1244-8.
- Jagtap VR, Ganu JV, Nagane NS (2011) BMD and Serum Intact Osteocalcin in Postmenopausal Osteoporosis Women. Indian J Clin Biochem 26: 70-3.
- Beg M, Akhtar N, Alam M, Rizvi I, Ahmad J, Gupta A (2014) Vitamin D status and serum osteocalcin levels in post-menopausal osteoporosis: Effect of bisphosphonate therapy. JIACM 15: 172-6.
- Sambrook P, Cooper C (2006) Osteoporosis. Lancet 367: 2010-8.
- Jorde R, Stunes AK, Kubiak J, Joakimsen R, Grimnes G, Thorsby PM, et al. (2019) Effects of vitamin D supplementation on bone turnover markers and other bone-related substances in subjects with vitamin D deficiency. Bone 124: 7-13.
- Waltman NL, Ott CD, Twiss JJ, Gross GJ, Lindsey AM (2009) Vitamin D insufficiency and musculoskeletal symptoms in breast cancer survivors on aromatase inhibitor therapy. Cancer Nurs 32: 143-50.
- Geisler J (2011) Differences between the non-steroidal aromatase inhibitors anastrozole and letrozole--of clinical importance? Br J Cancer 104: 1059-66.
FIGURE 1
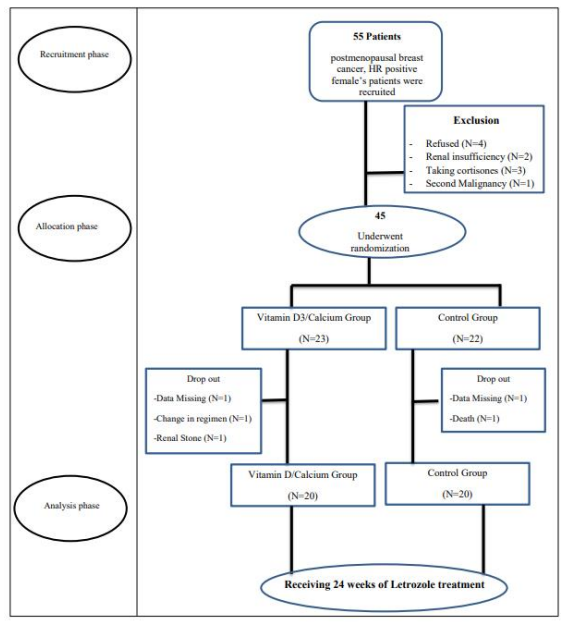
Figure 1: Flow chart of the study participants
FIGURE 2
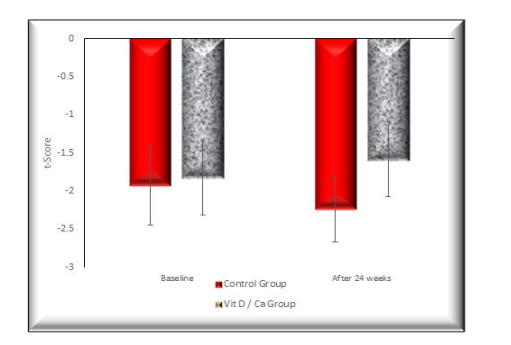
Figure 2: Bone mineral density for the two study groups
Control group: postmenopausal, hormone receptor positive female patients with breast cancer received Letrozole only for 24 weeks, Vit D3/-
Ca group: postmenopausal, hormone receptor positive female patients
with breast cancer received Letrozole in addition to 2000IU vitamin D3 and 1000mg Calcium for 24 weeks.
Tables at a glance
Figures at a glance