Management of the Axilla in Breast Cancer Surgery
Received Date: April 04, 2024 Accepted Date: May 04, 2024 Published Date: May 07, 2024
doi: 10.17303/jocr.2024.5.102
Citation: Lužaić K, Lachanas K, Vamvakopoulos K-O, Sidiropoulos A, Vamvakopoulou D, Nomikos I. (2024) Management of the Axilla in Breast Cancer Surgery. JJ Oncol Clin Res 5: 1-11
Abstract
We summarize important clinical advances that have led us to today's surgical management of breast cancer and pave the way to new levels of de-escalation in breast cancer surgery.
Keywords: Breast Conserving Surgery; Lymph Nodes; Radiotherapy of the Axilla; Neoadjuvant Chemotherapy
Abbreviations
CALND-complete axillary lymph node dissection,
DCIS-ductal carcinoma in situ,
ITC-isolated tumor cells,
NAC-neoadjuvant chemotherapy,
SLNB-sentinel lymph node biopsy,
TAD-targeted axillary dissection,
Introduction
Complete axillary lymph node dissection (CALND), involving the removal of potentially infiltrated lymph nodes from levels I and II of the axilla [1,2], was the most relevant prognostic factor for risk estimation in breast cancer through the late 1990s [3-5]. The less invasive sentinel lymph node biopsy (SLNB) procedure, which uses a vital blue dye and/or 99m technetium sulfur colloid to identify the first lymph node draining from the tumor, was introduced in 1993 [6-8]. We review the implications of clinical trials that led to present-day diagnostic and therapeutic approaches to the axilla and pave ways to improved treatment of breast cancer.
Clinical Trial Records
Axillary Node-Negative Invasive Breast Cancer
Several carefully designed multicenter clinical trials (Z0010, NSABP-32, ALMANAC) from early 2000, converged on the establishment of sentinel lymph node biopsy (SLNB) as the treatment of choice for early-stage breast cancer patients with clinically negative nodes [9-12].
Axillary Metastatic Disease in Invasive Breast Cancer
a) Isolated tumor cells or Micrometastases
A similarly renowned clinical trial (IBCSG 23-01) confirmed that CALND is not required for patients with occult sentinel lymph node (SLN) metastases [13,14].
b) Macrometastases
A pioneer clinical trial from the early 1970s (NSABP B-04) studied the outcome of total mastectomy with and without radiation therapy in patients with clinically negative nodes and found no significant difference in disease-free survival and mortality for any treatment regimen used. The only significant finding was a greater incidence of treatment failure and mortality in patients with clinically positive nodes [15,16]. The host of clinical trials that followed refined most clinical practices in the surgical treatment of breast cancer. ACOSOG Z0011 assessed the omission of CALND in women with clinically node-negative axilla who underwent breast-conserving surgery (BCS) [17,18] and concluded that CALND can be omitted in patients with T1-2 tumors and with up to two metastases on SLNB without extra-nodal extension [19-21]. AMAROS (After Mapping of the Axilla: Radiotherapy or Surgery) compared CALND with SLNB plus axillary and supraclavicular radiotherapy in T1-2 early breast cancer patients with positive SLNB and found that cases with clinically negative nodes but positive SLN(s) could forgo CALND and receive axillary radiation with less morbidity [22]. OTOASOR (The Optimal Treatment of the Axilla - Surgery or Radiotherapy) found no significant difference in axillary recurrence of CALND (2%), radiotherapy (1.7%) and overall survival with a mean follow-up of 97 months. Arm morbidity was higher in the CALND group (15.3%) than in the radiotherapy group (4.7%) after one year of radiation treatment at the axillary levels, supraclavicular, and ± internal mammary nodes [23]. ACOSOG Z1071 enrolled women with biopsy-proven clinical stage T0–T4, N1, or N2 breast cancer, to determine the false-negative rate of SLNB in originally node-positive patients following neoadjuvant chemotherapy (NAC) [24]. The majority of patients had mobile lymphadenopathy at presentation, i.e., clinical stage N1, and following neoadjuvant treatment, over 80% of those had no residual palpable axillary nodes. The study protocol stipulated that at least two sentinel nodes should be removed, after which an CALND was performed. While 93% of patients had at least one sentinel node identified, only 79% met the criteria for the removal of two sentinel nodes, followed by a CALND. cN1 patients with at least two sentinel nodes removed, had a false-negative rate of 12.6%. A reduction in false-negative rate was evident as the number of sentinel nodes removed increased, dropping to the clinically acceptable rate of 9% only upon removal of three or more nodes. The false-negative rate was also low (11%) when both blue dye and radio colloid tracers were used for axillary mapping [14,24]. SENTINA (SENTInel Neo Adjuvant) enrolled both clinically node-negative and node-positive patients before neoadjuvant chemotherapy (NAC) [25]. These patients received a post-neoadjuvant SLNB followed by CALND. Unlike the Z1071 trial, a biopsy of clinically or radiologically suspicious axillary nodes was recommended. The overall sentinel node detection rate was 80%, with a false-negative rate of 14%. Just like in ACOSOG Z1071, the false-negative rate varied according to the number of sentinel nodes removed: 24%, one node; 18%, two nodes; and less than 8% when three or more nodes were removed [14,25].
Clinical Implications and Recommendations
Early Breast Cancer
a) Clinically Negative Nodes
From its introduction [8,26], SLNB with an identification rate of over 90% [27-31] became rapidly the standard procedure for early-stage breast cancer patients with cT1-2 negative axillary nodes. Women without SLNB metastases should not receive CALND. Surgeons who perform SLNB however, should be cautious of rare, less than 10%, false-negative rate cases, because of their higher axillary recurrence and inappropriate staging probabilities. Axillary recurrence after a negative SLNB is generally an early event, occurring within the first five years after surgery [32]. Meta-- analyses recorded an axillary recurrence of 0,3% after a median follow-up of 34 months [33], which increased to 0,7% after five years and to 0,8% after 10 and 15 years from surgery [32].
b. Clinically Positive Nodes
b. 1) Micrometastases: Initial guidelines recommended a CALND when micro-metastases were found. However, studies showed that with modern adjuvant therapy regimens, the additional surgical treatment of the axilla confers no advantage to overall survival or disease-free survival. Central pathology review of NSABP B-32 trial, identified isolated tumor cells (ITC) in 11% of nodal specimens from initially SLNB-negative patients. The absolute reduction in overall survival of patients with ITC or micro-metastases was only 1.2%. Thus, women with these small-volume nodal diseases who underwent SLNB plus CALND, had no survival advantage over those with SLNB alone [14].
b. 2) Macrometastases
b. 2a) Clinically Negative, SLNB Positive Axillary Nodes:Despite arm morbidity, CALND was the standard treatment of breast cancer patients with SLNB metastasis until 2011 [34-37]. However, the absence of significant difference in axillary recurrence, overall survival and disease-free survival of patients not submitted to CALND who received axillary radiotherapy, supported the omission of CALND in SLNB-positive breast cancer patients undergoing breast-conserving surgery or mastectomy, should the axilla be treated with radiotherapy. Furthermore, the lack of significant difference in axillary recurrence in cT1-2 patients with up to two metastases on SLNB without extra-nodal extension who underwent breast-conserving surgery without CALND followed by whole breast radiotherapy, compared with those undergoing CALND, could be attributed to the tangential radiation effect for the axillary region during whole breast radiotherapy. In conclusion, axillary dissection can safely be omitted in patients with up to two metastatic SLNB and without extra-nodal extension undergoing breast-conserving surgery or in patients with metastatic sentinel lymph nodes undergoing breast-conserving surgery or mastectomy after adjuvant radiotherapy [38].
b. 2b) Clinically Positive Nodes: The American Joint Committee on Cancer (AJCC) recommends imaging studies or clinical examination for the identification of clinically node-positive patients. Axillary ultrasound (U/S) combined with U/S-guided lymph node biopsy is increasingly being used to assess axillary lymph nodes at the time of presentation. Preoperative identification of axillary nodal positivity will select patients with axillary metastases who can proceed immediately to CALND without SLNB, or commence neoadjuvant systemic treatment aiming to axillary down-staging. The sensitivity of axillary US is 50% with 25% false-negative ratio [39]. Nonetheless, judicious use of US-guided axillary staging is required when deciding on the surgical management of the axilla. As established by the ACOSOG Z0011 trial, further treatment is not required in patients with one or two positive axillary nodes. The mere presence of abnormal nodes on imaging in clinically nodenegative patients is not reliable indicator for the need of CALND [40]. In conclusion, axillary radiotherapy successfully replaces CALND in patients with micro- or macro-metastasis on SLNB,. The arm morbidity rate is significantly lower in patients with positive SLNB treated with breast surgery and radiotherapy of the whole breast and axilla. Furthermore, axillary dissection could safely be omitted in patients with up to two metastatic nodes on SLNB and without extra-nodal extension, who undergo breast-conserving surgery and whole breast radiotherapy or in patients with radiotherapy for all three axillary levels, the supraclavicular fossa, and ± mammary internal and/or the whole breast or chest wall [14]. The diagram in Figure 1 displays the flowchart of recommended diagnostic and therapeutic interventions for early invasive breast cancer patients, in accordance to findings from clinical trials.
Management of the Axilla in Special Circumstances
Neoadjuvant Chemotherapy
National Comprehensive Cancer Network (NCCN) guidelines state that SLNB can be performed on selected patients with clinically N1 breast cancer who have clinically negative axillae after NAC. The SLNB false-negative rate can be improved by removing more than two lymph nodes, using dual tracers, or marking biopsied lymph nodes to document their removal [41]. Following these rules, the proportion of patients with positive SLNB who did not undergo CALND after NAC increased from 0 % in 2009 to 10% in 2017 [42]. NAC reduces the need for CALND and downstages axillary disease and surgical morbidity without increasing loco-regional recurrence risk. SLNB after NAC accurately represents the status of the axillary lymph nodes and therefore could guide the indication of CALND. CALND remains the standard treatment for patients with positive SLNB after NAC. However, it could be avoided in clinically axillary node-negative or in clinical or biopsy-proven axillary-positive patients who converted to clinical node-negative and had at least three negative SLN(s) or had any negative sentinel node, if SLNB is performed with dual tracer. National guidelines allow omission of CALND in cases with known node-positive clinical N1 disease having NAC treatment if a targeted axillary dissection (sentinel nodes + clipped node) demonstrates a complete pathologic response [43,44]. In patients with positive SLNB after NAC, axillary radiotherapy instead of CALND could lead to the conservation of the axilla and thus could avoid the harmful consequences of CALND [38].
Targeted Axillary Dissection
The high false–negative rates of SLNB after NAC in patients with clinically positive axillary nodes in both SENTINA and ACOSOG Z1071 trials (14.6% and 12.6% respectively) questioned the safety and reliability of SLNB in this group of patients [24,25]. Therefore, alternative less invasive surgical techniques were evaluated for axillary lymph node status assessment. Targeted axillary dissection (TAD) is a new concept for the assessment of axillary status where a formal SLNB is combined with a targeted lymph node biopsy (TLNB). In TLNB, at least 1 suspicious lymph node (target lymph node) is marked before NAC either with an iodine seed or a clip followed by surgical removal of the marked lymph node after completion of NAC (44-51). SenTa, a prospective registry study, tested the safety of TAD without CALND after NAC in patients with node-positive breast cancer. Patients with clinically node-positive breast cancer underwent clipping of the most suspicious lymph node before NAC. After NAC and TAD, CALND followed according to the clinician’s choice. Patients who did not undergo TAD were excluded. No difference in invasive disease-free survival, breast cancer-specific survival, axillary recurrence, or loco-regional recurrence, and a low false-negative rate of 4.3% was recorded among 199 study participants after a follow-up of 43 months. The 3-year distant disease-free survival was 93.9%, ipsilateral axillary recurrence occurred in only 1.8% of patients receiving TAD alone, and no loco-regional recurrence occurred in patients who were ycN0 (ie clinically node-negative after NAC) and ypN0 (ie pathologically node-negative after NAC) with 3 or more nodes excised in the TAD group (45). So, there is convincing evidence that axillary staging based on TAD without CALND is associated with excellent clinical outcomes in selected patients, mainly those with good responses to NAC and at least 3 TAD lymph nodes. The diagram in Figure 2 displays the flowchart of recommended diagnostic and therapeutic interventions for patients who received NAC as an induction therapy, in accordance to findings from clinical trials.
Occult Breast Cancer with Axillary Metastases
Bilateral breast magnetic resonance imaging (MRI) is the standard imaging diagnostic approach to breast evaluation in this patient group. It detects primary breast cancer in approximately 75% of women with a normal breast on clinical examination, mammogram and ultrasound. These lesions should be subjected to MRI or U/Sguided biopsy if a suspicious lesion is identifiable. Accurate localization of the primary breast lesion may facilitate breast-conserving surgery in some of these patients. The surgical management of the axilla in this setting remains an CALND. Depending on the hormone receptors profile, NAC should be considered. Optimal management of the ipsilateral breast in patients with no primary breast lesion identification, even after MRI, remains controversial. High rates of loco-regional failure were observed in patients who received CALND without treatment to the ipsilateral breast, implying the need for treatment of the ipsilateral breast. A small number of comparative, non-randomized trials, recorded similar rates of both loco-regional recurrence and overall survival in patients treated with CALND and mastectomy or CALND and whole-breast radiotherapy [52]. Therefore, whole-breast radiotherapy is a breast-conserving alternative to mastectomy in these patients. The diagram in Figure 3 displays the flowchart of recommended diagnostic and therapeutic interventions in patients presented with invasive breast cancer metastatic disease in axillary lymph nodes without obvious breast lesion (occult breast cancer), according to findings from clinical trials.
Ductal Carcinoma in Situ
Patients with pure ductal carcinoma in situ (DCIS) have no risk of lymph node metastases and hence no need for axillary staging. Pathological assessment of resected specimens revealed that patients who proceeded to surgery after a breast core-needle biopsy diagnosis of DCIS, were at risk of upstaging to invasive cancer. The best estimate of upstaging to either micro-invasion or invasive cancer is approximately 15%. For patients undergoing a mastectomy for the surgical treatment of DCIS due to either disease extent or patient preference, an SLNB should be performed at the time of surgery if final histology reveals invasive disease, at which point an SLNB would not be feasible. Even in patients upstaged to micro-invasion, the risk of sentinel node metastases is only 1% [14]. The diagram in Figure 4 displays the flowchart of recommended clinical practices for the management of the axilla in patients with DCIS, according to findings from clinical trials.
Hormone Receptors Positive Breast Cancer
Endocrine therapy is the standard treatment for all patients with hormone-receptor-positive breast cancer. The omission of SLNB in women 70 years old or older with non-palpable axillary lymph nodes treated with endocrine therapy, does not increase loco-regional recurrence rate and has no impact on breast cancer mortality [53-56].
Summary of Key Findings and Future Perspectives
The diagrams in Figures 1-4 summarize the key findings from clinical trials and display the recommended breast cancer treatments in simple flowchart format that may serve as training primers to medical practitioners. It is imperative to note, however, that the practicing physician should adopt case-specific therapeutic approaches to the axilla, in association with patient’s age and tumor features, like hormone receptor and molecular profiling, along with patient’s consent following detailed and comprehensive presentation of suitable therapeutic alternatives, including CRISPR gene editing options, and their expected outcomes on patient’s quality of life. In line to breast conserving surgery, multicenter clinical assessments of axillary conserving surgery without compromising patient survival and quality of life, are also gaining pace [57,58]. It is estimated that the continuous enrichment of medical applications with modern technologies would significantly improve the disease-free survival outcome of breast cancer patients undergoing surgical treatment.
Concluding Remarks
- CALND can safely be omitted in T1-T2 invasive breast cancer that is clinically node-negative and sentinel-node negative or has up to two positive sentinel nodes.
- Clinical trials (ACOSOG Z1071, SENTINA) showed that SLNB following NAC conversion of node-positive disease to clinically node-negative, is an acceptable method for axilla staging.
- National guidelines allow omission of CALND in known NAC-treated node-positive clinical N1 cases, if TAD (sentinel nodes + clipped node) demonstrates a complete pathologic response.
- The promising introduction of artificial intelligence-guided procedures into clinical practice, may radically transform breast cancer surgery
- Toomey A, Lewis CR (2023) Axillary Lymphadenectomy. [Updated 2023 Jul 24]. In: StatPearls [Internet]. Treasure Island (FL).
- Nomikos IN (2018) Breast cancer and axillary lymph node dissection: past, present, future. Hellenic Journal of Surgery, 90: 167-8.
- Goldhirsch A, Glick JH, Gelber RD, Senn HJ (1998) Meeting highlights: International consensus panel on the treatment of primary breast cancer. J Natl Cancer Inst, 90: 1601-8.
- Goldhirsch A, Glick JH, Gelber RD, Senn HJ (1998) Meeting highlights: International consensus panel on the treatment of primary breast cancer. J Natl Cancer Inst, 90: 1601-8.
- Rescigno J, Zampell JC, Axelrod D (2009) Patterns of axillary surgical care for breast cancer in the era of sentinel lymph node biopsyAnn Surg Oncol, 16: 687-96.
- Amersi F, Giuliano AE (2013) Management of the axilla. Hematol Oncol Clin North Am, 27: 687-702.
- Bembenek A, Schlag PM (2001) Sentinel node detection. In: Holzheimer RG, Mannick JA, editors. Surgical Treatment: Evidence-Based and Problem-Oriented. Munich: Zuckschwerdt.
- Krag DN, Weaver DL, Alex JC, Fairbank JT (1993) Surgical resection and radiolocalization of the sentinel lymph node in breast cancer using a gamma probe. Surg Oncol, 2: 335-40.
- Hunt KK, Ballman KV, McCall LM et al. (2012) Factors associated with local-regional recurrence after a negative sentinel node dissection: results of the ACOSOG Z0010 trial. Ann Surg, 256: 428-36.
- Fisher CS, Margenthaler JA, Hunt KK, Schwartz T (2020) The landmark series: axillary management in breast cancer. Ann Surg Oncol, 27: 724-9.
- Krag DN, Anderson SJ, Julian TB et al. (2010) Sentinel-lymph-node resection compared with conventional axillary-lymph-node dissection in clinically node-negative patients with breast cancer: Overall survival findings from the NSABP B-32 randomized phase 3 trial. Lancet Oncol, 11: 927-33.
- Mansel RE, Fallowfield L, Kissin M et al. (2006) Randomized multicenter trial of sentinel node biopsy versus standard axillary treatment in operable breast cancer: The ALMANAC trial. J Natl Cancer Inst, 98: 599-609.
- Galimberti V, Cole BF, Zurrida S et al. (2013) Axillary dissection versus no axillary dissection in patients with sentinel-node micrometastases (IBCSG 23-01): A phase 3 randomized controlled trial. Lancet Oncol, 14: 297-305.
- McCartan D, Gemignani ML (2016) Current management of the axilla. Clin Obstet Gynecol, 59: 743-55.
- Fisher B, Wolmark N, Redmond C, Deutsch M, Fisher ER (1981) Findings from NSABP Protocol No. B-04: comparison of radical mastectomy with alternative treatments. II. The clinical and biologic significance of medial-central breast cancers. Cancer, 48: 1863-72.
- Fisher B, Montague E, Redmond C et al. (1980) Findings from NSABP Protocol No. B-04-comparison of radical mastectomy with alternative treatments for primary breast cancer. I. Radiation compliance and its relation to treatment outcome. Cancer, 46: 1-13.
- Giuliano AE, Ballman KV, McCall L et al. (2017) Effect of axillary dissection vs no axillary dissection on 10-year overall survival among women with invasive breast cancer and sentinel node metastasis: The ACOSOG Z0011 (Alliance) randomized clinical trial. JAMA - Journal of the American Medical Association, 318: 918-26.
- Giuliano AE, McCall L, Beitsch P et al. (2010) Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases: the American College of Surgeons Oncology Group Z0011 randomized trial. Ann Surg, 252: 426-33.
- Dengel LT, Van Zee KJ, King TA et al. (2014) Axillary dissection can be avoided in the majority of clinically node-negative patients undergoing breast-conserving therapy. Ann Surg Oncol, 21: 22-7.
- Yi M, Kuerer HM, Mittendorf EA et al. (2013) Impact of the American College of Surgeons Oncology Group Z0011 criteria applied to a contemporary patient population. J Am Coll Surg, 216: 105-13.
- Roberts A, Nofech-Mozes S, Youngson B, Youngson B, McCready DR, Al-Assi M Cil Tulin (2015) The importance of applying ACOSOG Z0011 criteria in the axillary management of invasive lobular carcinoma: a multi-institutional cohort study. Ann Surg Oncol, 22: 3397-401.
- Donker M, van Tienhoven G, Straver ME et al. (2014) Radiotherapy or surgery of the axilla after a positive sentinel node in breast cancer (EORTC 10981-22023 AMAROS): A randomized, multicentre, open-label, phase 3 non-inferiority trial. Lancet Oncol, 15: 1303-10.
- Sávolt Á, Péley G, Polgár C et al. (2017) Eight-year follow-up result of the OTOASOR trial: the optimal treatment of the axilla - surgery or radiotherapy after positive sentinel lymph node biopsy in early-stage breast cancer: A randomized, single centre, phase III, non-inferiority trial. Eur J Surg Oncol, 43: 672-9.
- Boughey JC, Suman VJ, Mittendorf EA, et al. (2013) Sentinel lymph node surgery after neoadjuvant chemotherapy in patients with node-positive breast cancer: The ACOSOG Z1071 (alliance) clinical trial. JAMA, 310: 1455-61.
- Kuehn T, Bauerfeind I, Fehm T et al. (2013) Sentinel-lymph-node biopsy in patients with breast cancer before and after neoadjuvant chemotherapy (SENTINA): A prospective, multicentre cohort study. Lancet Oncol, 14: 609-18.
- Giuliano AE, Kirgan DM, Guenther JM, Morton DL (1994) Lymphatic mapping and sentinel lymphadenectomy for breast cancer. Ann Surg, 220: 391-401.
- Tafra L, Lannin DR, Swanson MS, et al. (2001) Multicenter trial of sentinel node biopsy for breast cancer using both technetium sulfur colloid and isosulfan blue dye. Ann Surg, 233: 51-9.
- McMasters KM, Tuttle TM, Carlson DJ et al. (2000) Sentinel lymph node biopsy for breast cancer: a suitable alternative to routine axillary dissection in multi-institutional practice when optimal technique is used. J Clin Oncol, 18:2560-6.
- Kim T, Giuliano AE, Lyman GH (2006) Lymphatic mapping and sentinel lymph node biopsy in early-stage breast carcinoma: A meta-analysis. Cancer, 106: 4-16.
- Zavagno G, De Salvo GL, Scalco G et al (2008) A randomized clinical trial on sentinel lymph node biopsy versus axillary lymph node dissection in breast cancer: Results of the Sentinella/GIVOM trial. Ann Surg, 247: 207-13.
- Kuru B, Gulcelik MA, Topgul K et al. (2011) Application of sentinel node biopsy in breast cancer patients with clinically negative and positive axilla and role of axillary ultrasound examination to select patients for sentinel node biopsy. J BUON, 16: 454-9.
- Matsen C, Villegas K, Eaton A et al. (2016) Late axillary recurrence after a negative sentinel lymph node biopsy is uncommon. Ann Surg Oncol, 23: 2456-61.
- van der Ploeg IMC, Nieweg OE, van Rijk MC, Valdés Olmos RA, Kroon BBR (2008) Axillary recurrence after a tumour-negative sentinel node biopsy in breast cancer patients: A systematic review and meta-analysis of the literature. European Journal of Surgical Oncology, 34: 1277-84.
- Veronesi U, Viale G, Paganelli G et al. (2010) Sentinel lymph node biopsy in breast cancer: Ten-year results: Of a randomized controlled study. Ann Surg, 251: 595-600.
- Lyman GH, Giuliano AE, Somerfield MR et al. (2005) American Society of Clinical Oncology guideline recommendations for sentinel lymph node biopsy in early-stage breast cancer. Journal of Clinical Oncology, 23: 7703-20.
- Ozaslan C, Kuru B (2004) Lymphedema after treatment of breast cancer. Am J Surg, 187: 69-72.
- Armer JM, Ballman K V, McCall L et al. (2019) Factors associated with lymphedema in women with node-positive breast cancer treated with neoadjuvant chemotherapy and axillary dissection. JAMA Surg, 154: 800-9.
- Kuru B (2020) The adventure of axillary treatment in early-stage breast cancer. Eur J Breast Health, 16: 1-15.
- Diepstraten SCE, Sever AR, Buckens CFM et al. (2014) Value of preoperative ultrasound-guided axillary lymph node biopsy for preventing completion axillary lymph node dissection in breast cancer: A systematic review and meta-analysis. Ann Surg Oncol, 21: 51-9.
- Pilewskie M, Jochelson M, Gooch JC, Patil S, Stempel M, Morrow M (2016) Is preoperative axillary imaging beneficial in identifying clinically node-negative patients requiring axillary lymph node dissection? J Am Coll Surg, 222:138-45.
- Gradishar WJ, Moran MS, Abraham J et al. (2023) NCCN Guidelines® Insights: Breast Cancer, Version 4.2023. J Natl Compr Canc Netw, 21: 594-608.
- T Nguyen TT, Hoskin TL, Day CN et al. (2018) Decreasing use of axillary dissection in node-positive breast cancer patients treated with neoadjuvant chemotherapy. Ann Surg Oncol, 25: 2596-602.
- G Curigliano G, Burstein HJ, Winer EP et al. (2017) De-escalating and escalating treatments for early-stage breast cancer: The St. Gallen International Expert Consensus Conference on the Primary Therapy of Early Breast Cancer 2017. Annals of Oncology, 28: 1700-12.
- Gradishar WJ, Moran MS, Abraham J et al. (2022) Breast Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. Journal of the National Comprehensive Cancer Network, 20: 691-722.
- Kuemmel S, Heil J, Rueland A, et al. (2022) A prospective, multicenter registry study to evaluate the clinical feasibility of targeted axillary dissection (TAD) in node-positive breast cancer patients. Ann Surg, 276: 553-62.
- Swarnkar PK, Tayeh S, Michell MJ, Mokbel K (2021) The evolving role of Marked Lymph Node Biopsy (MLNB) and Targeted Axillary Dissection (TAD) after Neoadjuvant Chemotherapy (NACT) for node-positive breast cancer: systematic review and pooled analysis. Cancers (Basel), 13: 1539.
- Caudle AS, Kuerer HM (2015) Targeting and limiting surgery for patients with node-positive breast cancer. BMC Med, 13.
- Caudle AS, Yang WT, Krishnamurthy S et al. (2016) Improved axillary evaluation following neoadjuvant therapy for patients with node-positive breast cancer using selective evaluation of clipped nodes: Implementation of targeted axillary dissection. Journal of Clinical Oncology, 34: 1072-8.
- Donker M, Straver ME, Wesseling J et al. (2015) Marking axillary lymph nodes with radioactive iodine seeds for axillary staging after neoadjuvant systemic treatment in breast cancer patients the mari procedure. Ann Surg, 261: 378-82.
- Flores-Funes D, Aguilar-Jiménez J, Martínez-Gálvez M et al. (2019) Validation of the targeted axillary dissection technique in the axillary staging of breast cancer after neoadjuvant therapy: Preliminary results. Surg Oncol, 30: 52-7.
- Caudle AS, Yang WT, Mittendorf EA et al. (2015) Selective surgical localization of axillary lymph nodes containing metastases in patients with breast cancer: A prospective feasibility trial. JAMA Surg, 150: 137-43.
- Macedo FIB, Eid JJ, Flynn J, Jacobs MJ, Mittal VK (2016) Optimal Surgical Management for Occult Breast Carcinoma: A Meta-analysis. Ann Surg Oncol, 23: 1838-44.
- Hughes KS, Schnaper LA, Bellon JR et al. (2013) Lumpectomy plus tamoxifen with or without irradiation in women age 70 years or older with early breast cancer: Longterm follow-up of CALGB 9343. Journal of Clinical Oncology, 31: 2382-7.
- Martelli G, Miceli R, Daidone MG et al. (2011) Axillary dissection versus no axillary dissection in elderly patients with breast cancer and no palpable axillary nodes: Results after 15 years of follow-up. Ann Surg Oncol, 18: 125-33.
- Rudenstam CM, Zahrieh D, Forbes JF et al. (2006) A randomized trial comparing axillary clearance versus no axillary clearance in older patients with breast cancer: First results of International Breast Cancer Study Group trial 10-93. Journal of Clinical Oncology, 24: 337-44.
- Bredbeck BC, Baskin AS, Wang T et al. (2022) Incremental Spending Associated with Low-Value Treatments in Older Women with Breast Cancer. Ann Surg Oncol, 29:1051-9.
- Oreste Davide Gentilini, Edoardo Botteri, Claudia Sangalli, Viviana Galimberti, Mauro Porpiglia, et al. (2023) for the SOUND Trial Group. Sentinel Lymph Node Biopsy vs No Axillary Surgery in Patients With Small Breast Cancer and Negative Results on Ultrasonography of Axillary Lymph Nodes The SOUND Randomized Clinical Trial. JAMA Oncol, 9: 1557-64.
- Toralf Reimer, Angrit Stachs, Kristina Veselinovi, Silke Polata, Thomas Müller, et al. (2023) on behalf of the INSEMA investigators. Patient-reported outcomes for the Intergroup Sentinel Mamma study (INSEMA): a randomised trial with persistent impact of axillary surgery on arm and breast symptoms in patients with early breast cancer. www.thelancet.com e Clinical Medicine, 55: 101756.
FIGURE 1
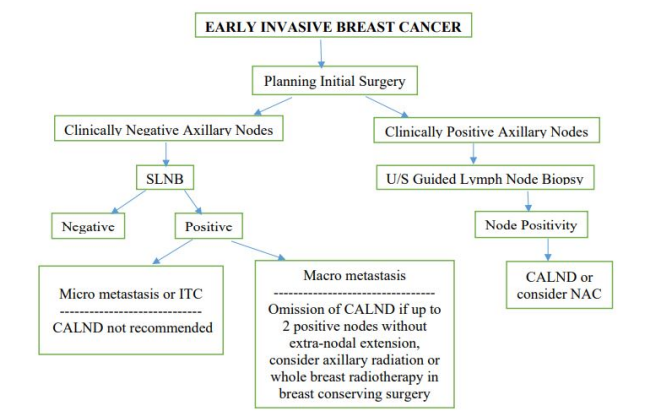
Figure 1: Flowchart of recommended diagnostic and therapeutic interventions in early invasive breast cancer patients aiming to de-escalate axillary surgery
FIGURE 2
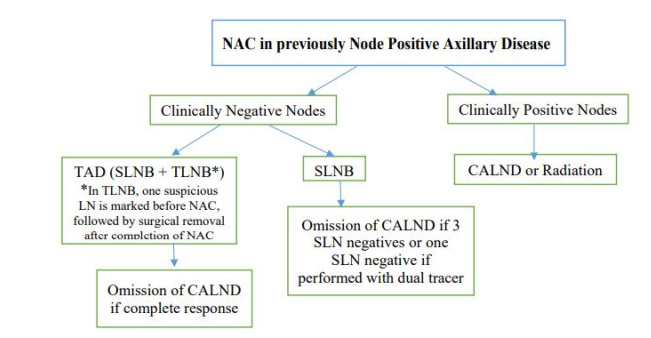
Figure 2: Flowchart of recommended diagnostic and therapeutic interventions in patients where NAC had been preceded as induction therapy. The new technique of TAD was introduced to reduce the high false negative rates of SLNB
FIGURE 3
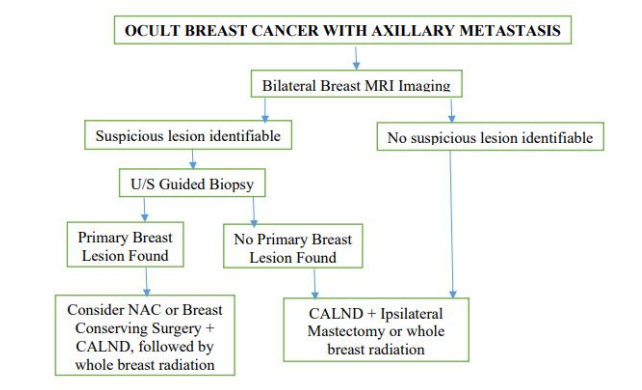
Figure 3: Flowchart of recommended diagnostic and therapeutic interventions in patients presented with occult breast cancer involving invasive breast cancer metastatic disease in axillary lymph nodes without obvious breast lesions
FIGURE 4
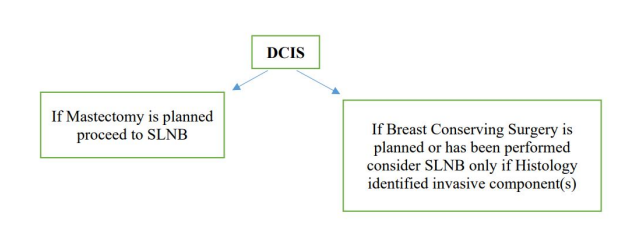
Figure 4: Flowchart of recommended management of the axilla in patients with DCIS. Axillary staging is only indicated if total mastectomy is planned or when a macro-invasive component is found on Histology
Figures at a glance