Succinate Dehydrogenase Subunit B Deficient Pediatric Gastrointestinal Stromal Tumor
Received Date: August 22, 2024 Accepted Date: September 22, 2024 Published Date: September 25, 2024
doi: DOI: 10.17303/jocr.2024.5.104
Citation: Melek Yaman Ortaköylü MD, Sonay İncesoy Özdemir MD, Dilvin Çelik Ateş MD, Hale Kıvrak MD, Işınsu Kuzu MD, et al. (2024) Succinate Dehydrogenase Subunit B Deficient Pediatric Gastrointestinal Stromal Tumor. JJ Oncol Clin Res 5: 1-6
Abstract
Gastrointestinal stromal tumors (GISTs) are rare mesenchymal neoplasms with 0,4-2 % occurring in individuals under the age of 20 years. We present a case of a pediatric GIST with Succinate Dehydrogenase (SDH) subunit B deficiency, managed with imatinib for 33 months without disease recurrence. Although SDH-deficient GISTs are known to be unresponsive to imatinib, it is difficult to assess meaningful treatment responses to the use of alternative tyrosine kinase inhibitors because of the rarity of cases and the slow natural course of the disease.
Keywords: Gastrointestinal Stromal Tumors; GIST; SDH-Deficient; Tyrosine Kinase Inhibitors
Introduction
Gastrointestinal stromal tumors (GISTs) are rare mesenchymal neoplasms of the gastrointestinal tract. GISTs occur predominantly in older individuals and exceedingly uncommon in children and adolescents. Approximately 0,4-2 % of GISTs arise in children and young adults under the age of 20 years [1]. Most GISTs are driven by KIT (CD117) or platelet derived growth factor receptor alpha (PDGFRA) gene mutations. Eighty five percent of pediatric GISTs and 15 % of adult GISTs lack oncogenic mutations in KIT and PDGFRA. These wild type (WT) GISTs are known to respond poorly to kinase inhibitor treatment [2]. The WT GISTs can be classified into two main subtypes as succinate dehydrogenase (SDH)-competent and deficient, according to the SDH immunohistochemical status. To diagnose SDH deficiency, tumor immunostaining for SDHB is relevant. Absence of SDHB indicates germline and/or somatic loss of function mutations in any of the four SDH subunits (SDHA, SDHB, SDHC or SDHD) [3,4]. Here we would like to introduce the Succinate Dehydrogenase subunit B deficient pediatric GIST case.
Case Presentation
The patient was a 10-year-old otherwise healthy girl who initially presented with upper gastrointestinal bleeding. She was admitted to the emergency department with the complaints of hematochezia and melena. Upper gastrointestinal endoscopy revealed an ulcerated mass lesion involving the antrum and corpus of the stomach, measuring approximately 6,3 centimeter in greatest diameter. No metastasis or other mass was detected in abdominal tomography. A subtotal gastrectomy was performed. The patient was residing in the Eastern Anatolia region, and operation was performed there. Upon consultation, the pathology slides were bought for further genetic examination at an advanced center.
In the pathological microscopic examination, tumoral growth was observed in the muscularis propria, which developed as large nodules, involving the entire wall from the serosa to the mucosa. Tumor forming cells were identified as having oval or spindle-shaped nuclei and pale eosinophilic cytoplasm with indistinct borders, containing fine granular chromatin. Bleeding was observed in certain areas within the tumor, along with superficial ulceration and mucosal involvement, as well as necrosis in a few regions. No lymph node metastasis was detected. In the immunohistochemical examination, the infiltrative cells were found to strongly express CD34, CD117, and DOG1. Conversely, they tested negative for Desmin, SMA, and S-100; while normal smooth muscle and nerve cells in the surrounding environment tested positive. The proliferation index, as determined by Ki-67, was found to be 7%.
DNA extraction was carried out from paraffin block sections containing 90% neoplastic cells. Despite screening all exons of the KIT and PDGFRA genes, no clinically significant mutations were found, in line with current literature. However, in Exon 4 of the SDHD gene (NCBI NM_001276506.2 transcript variant), a clinically significant frameshift mutation, according to Phase1A-AMP/ASCO/- CAP 2017 guideline, (nucleotide c.370dupC, amino acid p.Q124fs*) resulting in loss of function in the protein was detected, leading to a loss of protein function, with a 5.85% allele frequency in 9454 reads. Additionally, in Exon 11 of the SDHA gene (NCBI NM_001294332.1 transcript variant), a point mutation (nucleotide c.1477A>T, amino acid p.K493*) was identified, possibly leading to protein dysfunction, with a 1.85% allele frequency in 1457 reads. While SDHA was widely cytoplasmic positive in tumoral cells, loss of diffuse expression with SDHB was noted. Based on these findings, the case was classified as SDHB Deficient GIST. Notably, the mutations identified here are novel variants not previously reported in SDH-deficient GISTs.
Discussion
Some GISTs arise in the setting of specific tumor syndromes such as familial GIST, Carney’s triad, Carney-Stratakis syndrome, type 1 neurofibromatosis [1]. The patient’s medical history, physical examination, as well as laboratory and radiological findings, did not indicate any specific tumor syndromes. Since germline inherited SDH gene mutation can be seen in SDHB deficient GISTs, the patient was referred to genetic counseling [2]. No cancer history was present within the family.
Imatinib treatment at a dose of 400 mg once a day commenced three months post-surgery. The drug has been well-tolerated, with no reported side effects. She has been followed for 36 months since diagnosis without any signs of disease recurrence. Endoscopic examination which has been performed, revealed complete remission.
Like our patient, according to current literature, SDH-deficient GISTs predominantly manifest in the stomach, exhibit multifocality, multinodular architecture, and epithelioid/mixed cytomorphology, and are more commonly observed in younger, female patients [5,6].
This case report highlights a rare pediatric GIST involving a 10-year-old girl diagnosed with SDHB-deficient GIST, which is a subtype of WT GIST. While pediatric GISTs typically lack common KIT and PDGFRA mutations, the SDH-deficient subtype is characterized by mutations in the SDH genes, which were evident in this case (7). This case contributes valuable information to the limited pool of pediatric GIST cases, particularly regarding the novel mutations discovered in SDHD and SDHA and highlights the importance of genetic testing in diagnosis and management. These mutations are essential in understanding the tumor biology and have broader implications for diagnosis, prognosis, and therapeutic strategies in pediatric GISTs.
The introduction of TKIs changed the treatment of GISTs radically because of the impressive and effective control of disease with imatinib as the first-line treatment, especially in KIT and PDGFRA, TKI-sensitive mutations. After that, sunitinib and regorafenib are approved as the second and third-line treatments in patients with GISTs who develop resistance to imatinib [4,7,8]. Boikos et al. [9] and Heinrich et al. [10] stated that they observed almost no activity in their SDH deficient GISTs patients with Imatinib.However, the heterogeneous nature of these tumors means that these findings need to be assessed in light of the tumor biology on a case-by-case basis, as the sensitivities of the numerous different mutations found in these tumors are not well studied [11,12]. For example, recent reports have demonstrated that SDHA-mutated GIST subtype is imatinib responsive, likely because this mutation does not cause an inactivation of the SDH-complex [13]. Numerous studies have also suggested that second generation TKIs show improved activity against these subsets of tumors [14], thought likely due to its broadened activity against KIT, PDGFRA, PDGFRB, and VEGFR [15]. Studies by Janeway and Reichardt have also shown that second-generation TKIs have shown slowed progression of disease with imatinib-resistant GIST in both adult and pediatric patients [16,17]. Martin Broto and colleagues administered Regorafenib as a first-line treatment in a group of 15 KIT and PDGFR negative WT GIST patients. They observed that patients within the SDHD subgroup had a better clinical outcome [18]. The role of TKIs in patients with SDH deficient GISTs remains controversial and has limited results. Our patient has been followed in remission with imatinib for approximately three years.
The novel frameshift mutation in this case leads to a loss of function of the SDHD protein, which further disrupts the SDH complex. The absence of SDH activity, demonstrated by the loss of SDHB staining in immunochemistry, suggests that the tumor’s metabolic profile shifted towards glycolysis, a hallmark of cancer metabolism known as the Warburg effect [20]. This supports the idea that SDH-deficient GIST may not rely on the same signaling pathways as KIT or PDGFRA-mutant GISTs, thereby explaining their resistance to traditional TKIs like imatinib. The identification of a point mutation in exon 11 of the SDHA gene (p.K493*) is another important finding. While SDHA mutations are less common than SDHB or SDHC mutations in GISTs, its presence in this case broadens the understanding of the mutations spectrum in SDH-deficient GISTs [21].
Conclusion
To date, there is no published standard guidelines available for the best treatment of pediatric GISTs. The essential treatment for non-metastatic WT GISTs is surgery. In addition to providing local disease control, surgery is crucial for pathological diagnosis and genotyping. SDH deficient GISTs are known to be unresponsive to imatinib, but it is difficult to assess meaningful treatment responses to the use of alternative tyrosine kinase inhibitors because of the rarity of cases and the slow natural course of the disease. The observed remission in this patient following imatinib treatment challenges the established understanding that SDH-deficient GISTs are generally resistant to imatinib. This situation underlines the heterogeneous biology of GISTs with SDH mutations and suggests that treatment responses can vary. The observed favorable outcomes in SDHA-mutated GIST may provide further significance to the positive result achieved in this case, aligning with the growing evidence of improved survival in this specific subtype [22]. The importance of genetic evaluation in these patients lies in guiding diagnosis, prognosis, and personalized treatment strategies. There is a need for further research and the establishment of comprehensive treatment guidelines. Hence, it’s advisable to centralize patients in specialized centers and promote the sharing of results to increase knowledge about this rare childhood disease.
Declarations
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
- Joensuu H, Hohenberger P, Corless CL (2013) Gastrointestinal stromal tumour. Lancet. 382: 973-83.
- Belinsky MG, Rink L, von Mehren M (2013) Succinate dehydrogenase deficiency in pediatric and adult gastrointestinal stromal tumors. Front Oncol. 3: 117.
- Holmes P, Mark C, Markku M (2014) Succinate Dehydrogenase–Deficient Gastrointestinal Stromal Tumor: A Clinical Example and Discussion of the Entity. AJSP: Reviews & Reports, 19: 74-7.
- Nannini M, Rizzo A, Indio V, et al. (2021) Targeted therapy in SDH-deficient GIST. Ther Adv Med Oncol. 13: 17588359211023278.
- Lv BB, Li JM, Yao ZG, et al. (2021) Succinate dehydrogenase deficient gastrointestinal stromal tumor in a three month old boy with a fatal clinical course: a case report and review of literature. Diagn Pathol. 16: 14.
- Ibrahim A, Chopra S (2020) Succinate Dehydrogenase-Deficient Gastrointestinal Stromal Tumors. Arch Pathol Lab Med. 144: 655-60.
- Meyra Y, Shruti B, Avi K, et al. (2022) Establishment of Patient-derived Succinate Dehydrogenase-deficient Gastrointestinal Stromal Tumor Models for Predicting Therapeutic Response. Clin Cancer Res. 28: 187-200.
- Serrano C, George S (2020) Gastrointestinal Stromal Tumor: Challenges and Opportunities for a New Decade. Clin Cancer Res. 26: 5078-85.
- Schaefer IM, DeMatteo RP, Serrano C (2022) The GIST of Advances in Treatment of Advanced Gastrointestinal Stromal Tumor. Am Soc Clin Oncol Educ Book. 42: 1-15.
- Boikos SA, Pappo AS, Killian JK, et al. (2016) Molecular Subtypes of KIT/PDGFRA Wild-Type Gastrointestinal Stromal Tumors: A Report From the National Institutes of Health Gastrointestinal Stromal Tumor Clinic. JAMA Oncol. 2: 922-8.
- Heinrich MC, Rankin C, Blanke CD, et al. (2017) Correlation of Long-term Results of Imatinib in Advanced Gas trointestinal Stromal Tumors With Next-Generation Sequencing Results: Analysis of Phase 3 SWOG Intergroup Trial S0033. JAMA Oncol. 3: 944-52.
- Yantiss RK, Rosenberg AE, Sarran L, et al. (2005) Multiple gastrointestinal stromal tumors in type I neurofibromatosis: a pathologic and molecular study. Mod Pathol. 18: 475-84.
- Miranda C, Nucifora M, Molinari F, et al. (2012) KRAS and BRAF mutations predict primary resistance to imatinib in gastrointestinal stromal tumors. Clin Cancer Res. 18: 1769-76.
- Szucs Z, Thway K, Fisher C, et al. (2017) Molecular subtypes of gastrointestinal stromal tumors and their prognostic and therapeutic implications. Future Oncol. 13: 93-107.
- Agaram NP, Wong GC, Guo T, et al. (2008) Novel V600E BRAF mutations in imatinib-naive and imatinib-resistant gastrointestinal stromal tumors. Genes Chromosomes Cancer. 47: 853-9.
- Sakamoto KM (2004) Su-11248 Sugen. Curr Opin Investig Drugs. 5: 1329-39.
- Janeway KA, Albritton KH, Van Den Abbeele AD, et al. (2009) Sunitinib treatment in pediatric patients with advanced GIST following failure of imatinib. Pediatr Blood Cancer. 52: 767-71.
- Reichardt P, Kang YK, Rutkowski P, et al. (2015) Clinical outcomes of patients with advanced gastrointestinal stromal tumors: safety and efficacy in a worldwide treatment-use trial of sunitinib. Cancer. 121: 1405-13.
- Martin-Broto J, Valverde C, Hindi N, et al. (2023) REGISTRI: Regorafenib in first-line of KIT/PDGFRA wild type metastatic GIST: a collaborative Spanish (GEIS), Italian (ISG) and French Sarcoma Group (FSG) phase II trial. Mol Cancer. 22: 127.
- Karin E, Thamara EO, Thera PL, et al. (2020) Clinical implications of the oncometabolite succinate in SDHx-mutation carriers. Clin Genet. 97: 39-53.
- Pushpa N, Sudeep B, Paul TF, et al. (2019) Current Management of Succinate Dehydrogenase Deficient Gastrointestinal Stromal Tumors. Cancer Metastasis Rev. 38: 525-35.
- Ilaria G, Flavio F, Francesca F, et al. (2015) Good survival outcome of metastatic SDH-deficient gastrointestinal stromal tumors harboring SDHA mutations. Genet. Med. 17: 391-5
FIGURE 1
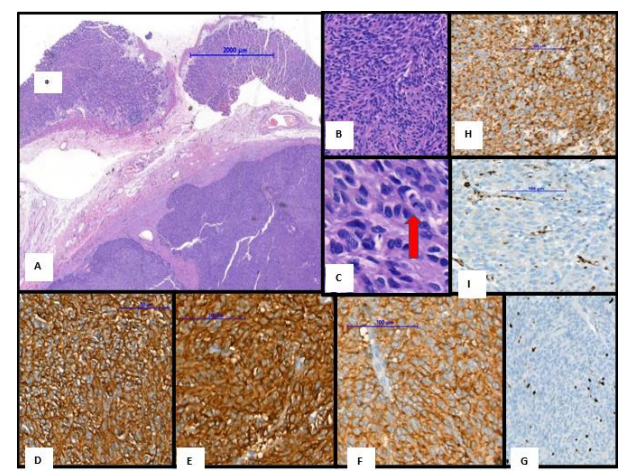
Figure 1: Morphology and immunohistochemical findings in case (A) The gastric tumor with multinodulated growth pattern (B,C) The tumor composed of spindl and epitheloid cells (E-G) Immunohistochemically, tumor cell expressed CD 34 (E), CD117 (F) and DOG-1 (G). (H) Ki67 proliferative activity found 7%. (I-J) Immunohistochemically, tumor showed SDHA positivity (I) while the expression of SDHB was lost (J).
Figures at a glance