Multi-Modal Assessment of LI-RADS 3 and 4 Lesions: Integrating Serum Biomarkers, Liquid Biopsy, and Imaging for Early Hepatocellular Carcinoma Detection and Management
Received Date: October 07, 2024 Accepted Date: November 07, 2024 Published Date: November 10, 2024
doi:10.17303/jocr.2024.5.201
Citation: Anna Dumbadze, Alexandre Tavartkiladze, Mariam Kutateladze, Malvina Javakhadze, Gaiane Simonia, et al. (2024) Multi-Modal Assessment of LI-RADS 3 and 4 Lesions: Integrating Serum Biomarkers, Liquid Biopsy, and Imaging for Early Hepatocellular Carcinoma Detection and Management. JJ Oncol Clin Res 5: 1-25
Abstract
Background: Hepatocellular carcinoma (HCC) is a leading cause of cancer-related deaths, often linked to chronic liver disease or cirrhosis. Early detection is vital for improving outcomes, yet diagnosing HCC, particularly in its early stages, remains difficult. The Liver Imaging Reporting and Data System (LI-RADS) classifies liver lesions based on imaging, with LIRADS 3 (LR-3) indicating intermediate probability and LI-RADS 4 (LR-4) indicating probable HCC. Combining serum biomarkers and liquid biopsy markers with imaging may enhance diagnostic accuracy.
Methods: We identified the NCOA4 expression in glioma cells and glioma specimens by Western blot (WB). Overexpression NCOA4 glioma cell lines were induced by recombinant adenovirus of NCOA4, and down-regulation NCOA4 glioma cell lines were induced by siRNA of NCOA4. GSH Detection Kit and DCFDA assay were used to detect cell GSH and ROS levels. CCK-8 and Transwell assays were used to detect cell proliferation and the sensitivity of glioma cells to temozolomide (TMZ).
Objective: This study evaluates the combined use of serum biomarkers, liquid biopsy (circulating tumor cells [CTCs] and circulating tumor DNA [ctDNA]), and imaging for assessing LI-RADS 3 and 4 lesions, with a focus on detecting early-stage HCC.
Methods: A cohort of 70 patients with LI-RADS 3 (n=42) and LI-RADS 4 (n=28) lesions confirmed via MRI or contrast-enhanced CT was analyzed. Serum biomarkers such as alpha-fetoprotein (AFP), AFP-L3, gamma-glutamyl transferase (GGT),hepatocyte growth factor (HGF), and interleukin-6 (IL-6) were measured. CTCs and ctDNA were assessed via immunocytochemistry and next-generation sequencing. Biomarker and liquid biopsy data were correlated with imaging findings to assess malignancy risk.
Results: LI-RADS 4 patients had higher elevations in AFP (211 ng/mL), AFP-L3 (48%), HGF (90%), and IL-6 (47%) compared to LI-RADS 3 patients. AFP was elevated in 47.61% of LI-RADS 3 cases (119 ng/mL), with ctDNA detected in 16.6%. CTCs were found in 17.85% of LI-RADS 4 patients, indicating a higher malignancy risk. Liquid biopsy provided additional insights when imaging was inconclusive.
Conclusion: Combining serum biomarkers, liquid biopsy, and imaging enhances diagnostic accuracy in LI-RADS 3 and 4 lesions, particularly for early-stage HCC detection and monitoring. Further research is needed to validate these findings in routine clinical practice.
Keywords: LI-RADS; Hepatocellular Carcinoma; Serum Biomarkers; Liquid Biopsy; Circulating Tumor Cells; Circulating Tumor DNA; Early Detection; Liver Cancer
Introduction
Liver cancer remains one of the most significant public health challenges worldwide due to its high prevalence, poor prognosis, and limited treatment options in advanced stages. According to the World Health Organization (WHO), liver cancer is the third leading cause of cancer-related deaths globally, with over 700,000 deaths annually. Among the various types of liver cancer, hepatocellular carcinoma (HCC) is the most common histological subtype, accounting for approximately 75-85% of primary liver cancer cases. The incidence of HCC is rising due to increasing rates of risk factors such as chronic hepatitis B and C virus infections, non-alcoholic fatty liver disease (NAFLD), and alcoholic liver disease. In light of these statistics, early detection and accurate characterization of liver lesions are critical for improving patient outcomes and reducing mortality rates [2,3,5,6,7,11,15,33].
The Liver Imaging Reporting and Data System (LI-RADS) was developed by the American College of Radiology (ACR) as a standardized method for interpreting and reporting liver imaging findings, particularly in patients at high risk for HCC. LI-RADS categorizes liver lesions detected through imaging studies, such as magnetic resonance imaging (MRI) or contrast-enhanced computed tomography (CT), into several categories based on their likelihood of being HCC. These categories range from LI-RADS 1 (definitely benign) to LI-RADS 5 (definitely HCC). Among these categories, LI-RADS 3 (LR-3) and LI-RADS 4 (LR-4) are particularly important because they represent lesions with an intermediate and high probability of being malignant, respectively [1,3,12,27,29] (Table #1).
LI-RADS 3 lesions are defined as having an intermediate probability of HCC, typically exhibiting imaging features that are suspicious but not definitive for malignancy. These lesions may show arterial phase hyperenhancement (APHE) but lack washout appearance or capsular retraction, making them challenging to categorize with certainty. In contrast, LI-RADS 4 lesions are considered probably HCC, meaning they have a high likelihood of being malignant, but still lack one or more criteria to be classified as definitive HCC (LI-RADS 5). LR-4 lesions often exhibit more pronounced imaging characteristics, such as APHE, nonperipheral washout in the venous or delayed phases, and capsular retraction, but may still pose diagnostic uncertainty. The indeterminate nature of LR-3 and LR-4 lesions necessitates further investigation, either through close imaging follow-up, biopsy, or the use of adjunct diagnostic tools [1,2,13,18,25,31].
While imaging techniques are central to the detection and characterization of liver lesions, they are not always sufficient to provide a definitive diagnosis, especially in the early stages of liver cancer. Small lesions may not exhibit all the classical imaging features of HCC, leading to diagnostic uncertainty. Moreover, biopsies, though considered the gold standard for diagnosis, are invasive and carry risks such as bleeding, infection, and tumor seeding. This has driven the search for non-invasive diagnostic methods that can complement imaging and improve the accuracy of HCC diagnosis, particularly for indeterminate lesions like LR-3 and LR-4 [8,9,14,17].
In recent years, advancements in liquid biopsy technologies have introduced promising non-invasive tools for the early detection, monitoring, and prognostication of liver cancer. Liquid biopsy refers to the analysis of biomarkers found in bodily fluids, such as blood, to provide information about the presence and characteristics of cancer. In the context of liver cancer, several blood-based biomarkers have emerged as potential adjuncts to imaging for diagnosing and monitoring the progression of liver lesions. These biomarkers can be broadly categorized into protein markers, circulating tumor cells (CTCs), and circulating free DNA (cfDNA), specifically circulating tumor DNA (ctDNA) [1,2,3,16,17].
Serum protein markers, such as alpha-fetoprotein (AFP) and its glycosylated isoform AFP-L3, have long been used as diagnostic tools for HCC. AFP is a fetal protein produced by hepatocytes and yolk sac cells during development, but its levels increase in the blood of adults with liver damage or cancer. AFP levels are often elevated in patients with HCC, particularly in more advanced cases, but its sensitivity and specificity are limited, especially for detecting early-stage HCC. AFP-L3, a more specific isoform of AFP, has been shown to be a more reliable biomarker for distinguishing HCC from benign liver conditions. Other serum markers, such as lactate dehydrogenase (LDH), carcinoembryonic antigen (CEA), and carbohydrate antigen 19-9 (CA19-9), also play a role in the diagnosis of liver cancer, though they are less specific to HCC and may be elevated in other types of cancers or liver diseases [1,3,7,21].
In addition to protein biomarkers, the detection of circulating tumor cells (CTCs) in the bloodstream has emerged as a valuable tool for cancer diagnosis and prognosis. CTCs are cancer cells that have detached from the primary tumor and entered the bloodstream, representing a key step in the metastatic process. The presence of CTCs in the blood of patients with liver lesions may indicate a higher likelihood of malignancy and increased risk of metastasis. CTC enumeration and characterization provide insights into tumor biology and can help refine the diagnosis of indeterminate liver lesions, such as LR-3 and LR-4 [2,3,4,11,19,28,19].
Circulating free DNA (cfDNA) and circulating tumor DNA (ctDNA) are also gaining attention as potential biomarkers for liver cancer. cfDNA refers to small fragments of DNA released into the bloodstream from apoptotic or necrotic cells, while ctDNA specifically originates from tumor cells. The detection of ctDNA in the blood provides valuable information about tumor burden, genetic mutations, and treatment resistance. Studies have shown that ctDNA levels correlate with tumor size, stage, and vascular invasion in HCC, making it a promising tool for risk stratification and early diagnosis. In the context of LI-RADS 3 and LI-RADS 4 lesions, ctDNA analysis could help identify occult malignancy that is not yet apparent on imaging, offering a non-invasive means of monitoring lesion progression [1,9,10,17,19].
Despite the potential of these biomarkers, their clinical utility in the diagnosis and management of LIRADS 3 and LI-RADS 4 lesions is still being explored. Few studies have systematically investigated the correlation between serum biomarkers, liquid biopsy findings, and histopathological confirmation of liver cancer in patients with LR-3 and LR-4 lesions. Therefore, there is a critical need for further research to determine the diagnostic value of combining imaging with liquid biopsy techniques for these indeterminate liver lesions [1,2,22,23].
In this study, we aim to investigate the correlation between serum biomarkers, liquid biopsy markers (CTCs and ctDNA), and histopathological findings in patients with LI-RADS 3 and LI-RADS 4 lesions. Specifically, we will evaluate the levels of key serum biomarkers, including AFP, AFP-L3, LDH, CEA, CA19-9, and inflammatory markers such as interleukin-6 (IL-6) and transforming growth factor-beta (TGF-β), in patients with LI-RADS 3 and LI-RADS 4 lesions. Additionally, we will assess the presence of CTCs and ctDNA in the blood to explore their potential as non-invasive diagnostic tools for liver cancer. By integrating these biomarkers with imaging findings, we hope to improve the accuracy of HCC diagnosis and provide valuable insights into the management of indeterminate liver lesions [1,7,8,9,10,19,21].
The objective of this study, Multi-Modal Assessment of LI-RADS 3 and 4 Lesions: Integrating Serum Biomarkers, Liquid Biopsy, and Imaging for Early Hepatocellular Carcinoma Detection and Management, focuses on enhancing diagnostic accuracy for indeterminate liver lesions by combining imaging with serum biomarkers and liquid biopsy. This research paper clarify how this study addresses gaps in the literature and informs clinical practice, for example: firstly, Existing Gaps and Challenges - Hepatocellular carcinoma (HCC) is frequently diagnosed at an advanced stage due to the limitations of current diagnostic methods. Although imaging techniques, particularly MRI and CT scans, are widely used to identify liver lesions and classify them according to the Liver Imaging Reporting and Data System (LI-RADS), they are sometimes insufficient to distinguish benign from malignant lesions, particularly in early-stage HCC. This limitation creates a critical need for more precise diagnostic approaches to aid early detection and improve patient outcomes. In particular, LI-RADS 3 and 4 lesions pose a diagnostic challenge, representing intermediate and probable malignancy, respectively. Traditional serum biomarkers like alpha-fetoprotein (AFP) have limited sensitivity and specificity, and while AFP-L3 improves specificity for HCC, it is not widely available in all clinical settings. Additionally, invasive biopsy procedures carry risks, making non-invasive diagnostic methods highly desirable. These factors highlight a crucial gap in non-invasive diagnostic techniques that can more accurately assess the malignant potential of liver lesions.
Contribution of This Study to the Literature: This research addresses the existing gap by proposing a multi-modal approach that combines serum biomarkers, liquid biopsy markers (such as circulating tumor cells [CTCs] and circulating tumor DNA [ctDNA]), and imaging findings. This integration is intended to increase diagnostic accuracy for LI-RADS 3 and 4 lesions, offering a novel strategy that is both non-invasive and practical for early detection. By evaluating biomarkers and liquid biopsy findings alongside imaging, this study aims to offer a comprehensive risk assessment for early-stage HCC that imaging alone cannot provide. Notably, while individual biomarkers like AFP and IL-6 have been studied, few works have systematically integrated these with CTCs and ctDNA analysis to differentiate indeterminate liver lesions. This approach is innovative as it leverages molecular and cellular insights to supplement imaging findings, thereby enhancing diagnostic precision.
Direct Implications for Clinical Practice: The findings of this study have clear practical applications. By integrating liquid biopsy and serum biomarkers into the standard imaging-based workflow for liver lesion assessment, clinicians can achieve a more comprehensive view of each lesion’s malignant potential, which could help reduce the need for invasive biopsies and provide earlier detection of HCC. Furthermore, this study highlights specific biomarkers, such as HGF and TGF-β, that correlate strongly with higher malignancy risk, helping clinicians to prioritize patients for closer monitoring or intervention. The application of CTCs and ctDNA as non-invasive markers in combination with serum biomarkers also provides a framework for ongoing monitoring, especially useful for patients under active surveillance for liver cancer risk. Therefore, this study aims to improve clinical decision-making in managing LIRADS 3 and 4 lesions, paving the way for more effective and individualized care strategies. Through this research, the authors intend to bridge the gap between traditional imaging diagnostics and emerging biomolecular techniques, thus offering valuable insights for integrating multi-modal approaches into routine clinical practice for better early detection and patient outcomes in liver cancer.
This study represents a critical step toward the development of a more comprehensive diagnostic approach for liver cancer, particularly for patients with LI-RADS 3 and LI-RADS 4 lesions, who may otherwise face diagnostic uncertainty. Through the combination of advanced imaging techniques and liquid biopsy biomarkers, we aim to enhance the early detection of HCC and ultimately improve patient outcomes [18,33].
Materials and Methods
Study Design and Population: This prospective cohort study was conducted over two years at a tertiary liver care center. It aimed to investigate the relationship between liquid biopsy biomarkers and imaging findings in patients with LI-RADS 3 and LI-RADS 4 lesions, which indicate intermediate and high probability of hepatocellular carcinoma (HCC). A total of 70 patients were included, with 42 diagnosed with LI-RADS 3 lesions and 28 with LI-RADS 4 lesions, based on magnetic resonance imaging (MRI) or contrast-enhanced computed tomography (CT). The study adhered to ethical guidelines, with written consent from all participants.
Inclusion and Exclusion Criteria: Inclusion criteria included adult patients (≥18 years) with chronic liver disease, cirrhosis, and LI-RADS 3 or LI-RADS 4 lesions con- formed by imaging. Exclusion criteria included patients with LI-RADS 1, 2, or 5 lesions, prior malignancies, recent infections or inflammatory diseases, and pregnant or breastfeeding women.
Biomarker Assessment: The study aimed to assess the relationship between serum biomarkers and histopathological confirmation of liver cancer. Blood samples were collected at diagnosis to measure biomarkers associated with liver disease and carcinogenesis, including:
1. AFP – Measured via immunoassay; elevated in HCC.
2. AFP-L3 – A more specific isoform of AFP for HCC.
3. GGT – Indicates liver disease; measured enzymatically.
4. ALP – Indicates bile duct involvement or liver disease.
5. LDH – Reflects tissue damage and metabolic activity.
6. CEA – A marker for gastrointestinal and liver cancers.
7. CA19-9 – Elevated in cholangiocarcinoma and some HCC cases.
8. HGF – Involved in liver regeneration and tumor growth.
9. IL-6 – A pro-inflammatory cytokine involved in tumor progression.
10. CRP – A marker of systemic inflammation.
11. TGF-β – Involved in fibrosis and tumor progression.
12. VEGF – A key regulator of angiogenesis
Liquid Biopsy: Two liquid biopsy markers, circulating tumor cells (CTCs) and circulating tumor DNA (ctDNA), were analyzed:
1. CTCs – Detected using immunocytochemical techniques with EpCAM staining. A cutoff of ≥1 CTC per 7.5 mL blood indicated positivity
2. ctDNA – Analyzed using next-generation sequencing (NGS) to detect tumor-specific mutations in plasma. A variant allele frequency (VAF) >1% was considered indicative of ctDNA presence.
Histopathological Analysis: Patients with elevated biomarkers or positive liquid biopsy results underwent liver biopsies for histopathological confirmation of HCC.Ultrasound-guided core needle biopsies were performed, and tissue samples were processed using standard histopathology techniques.
Reagents and standards were provided by Foconsci Chemical Industry, Shandong, China.
Results
Patient Demographics
The study included 70 patients with liver lesions categorized as either LI-RADS 3 (n=42, intermediate probability of HCC) or LI-RADS 4 (n=28, probable HCC). Patients' ages ranged from 29 to 77, with a mean age of 55.4 ± 10.2 years. Males made up 60% of the cohort. Chronic liver diseases, particularly cirrhosis, were prevalent, with hepatitis B virus (HBV) accounting for 40% of cases, hepatitis C virus (HCV) for 25%, non-alcoholic fatty liver disease (NAFLD) for 20%, and other causes for 15%. No significant differences were observed between LI-RADS 3 and LIRADS 4 etiologies, though patients with LI-RADS 4 had more advanced cirrhosis.
Serum Biomarker Findings in LI-RADS 3 Lesions
1. Alpha-Fetoprotein (AFP): Elevated in 47.61% of patients, with a mean value of 119 ng/mL. Although nonspecific for HCC, elevated AFP indicated a need for closer follow-up.
2. AFP-L3: Elevated by 33% in 28.57% of patients, more predictive of HCC than total AFP.
3. Gamma-Glutamyl Transferase (GGT): Increased by 8%, reflecting liver dysfunction, but not specifically linked to malignancy.
4. Alkaline Phosphatase (ALP): Elevated by 19%, possibly indicating biliary obstruction, though not consistently correlated with HCC.
5. Lactate Dehydrogenase (LDH): Increased by 27%, suggesting tissue damage, with further investigation needed for suspected malignancy.
6. Carcinoembryonic Antigen (CEA): Mildly elevated by 1.2%, prompting additional evaluation for possible extrahepatic malignancy.
7. Carbohydrate Antigen 19-9 (CA19-9): Marginally elevated by 0.9%, typically associated with cholangiocarcinoma.
8. Hepatocyte Growth Factor (HGF): Elevated by 77%, raising concerns about malignant transformation.
9. Interleukin-6 (IL-6): Elevated by 27%, indicating chronic liver inflammation.
10. C-Reactive Protein (CRP): Increased by 8%, reflecting low-grade systemic inflammation.
11. Transforming Growth Factor-beta (TGF-β): Elevated by 57.7%, suggesting active fibrosis or malignancy.
12. Vascular Endothelial Growth Factor (VEGF): Elevated by 29.7%, indicating increased vascular activity, though not all cases were malignant (Figure #1).
Liquid Biopsy Findings in LI-RADS 3 Lesions
Circulating Tumor Cells (CTCs): No CTCs were detected in any patients with LI-RADS 3 lesions. The absence of CTCs suggested that, in these patients, there was no evidence of active tumor cells in the bloodstream, which reduced the likelihood of metastasis at this stage.
Circulating Tumor DNA (ctDNA): ctDNA was elevated in 16.6% of patients with LI-RADS 3 lesions. The presence of ctDNA indicated tumor-specific genetic alterations, and in these cases, the detection of ctDNA was associated with a higher likelihood of malignant transformation. Patients with elevated ctDNA were monitored more closely through imaging and clinical follow-up (Figure #2).
Imaging Findings and Serum Biomarkers in LIRADS 3 Lesions
In patients diagnosed with LI-RADS 3 lesions, the imaging characteristics were consistent with intermediate probability for hepatocellular carcinoma (HCC). These lesions often displayed mild arterial phase hyperenhancement (APHE) without washout in the portal venous phase or capsular appearance.
Serum biomarker analysis revealed elevated AFP levels in 47.61% of patients, with a mean value of 119 ng/mL. Other elevated biomarkers included AFP-L3, GGT, and IL-6.
Serum Biomarker Findings in LI-RADS 4 Lesions
Alpha-Fetoprotein (AFP): AFP levels were elevated in 25% of patients, with a mean value of 211 ng/mL, indicating a higher likelihood of malignancy compared to LIRADS 3 patients. However, histopathological confirmation was often required.
AFP-L3: Elevated by 48% in 46.42% of patients, AFP-L3 is a more specific marker for HCC. The combination of elevated AFP-L3 and AFP strongly indicated probable malignancy.
Gamma-Glutamyl Transferase (GGT): GGT levels were 20% higher than normal, reflecting advanced liver disease and possible bile duct obstruction, often associated with malignant processes.
Alkaline Phosphatase (ALP): Elevated by 31%, ALP suggested greater biliary obstruction or involvement in malignancy, such as HCC or cholangiocarcinoma.
Lactate Dehydrogenase (LDH): Elevated by 33%,LDH indicated higher cellular metabolism, correlating with more aggressive disease.
Carcinoembryonic Antigen (CEA): Elevated by 5.7%, CEA suggested potential malignancy or metastases, although it is not a primary marker for HCC.
Carbohydrate Antigen 19-9 (CA19-9): Elevated by 2.8%, CA19-9 hinted at mixed hepatocellular-cholangiocarcinoma lesions or metastatic disease from gastrointestinal cancers.
Hepatocyte Growth Factor (HGF): Elevated by 90%, HGF was a strong indicator of heightened regenerative and malignant activity in the liver.
Interleukin-6 (IL-6): Elevated by 47%, IL-6 suggested a strong inflammatory response, linked to tumor progression and carcinogenesis.
C-Reactive Protein (CRP): Elevated by 9.9%, CRP indicated systemic inflammation, potentially associated with liver malignancy or cirrhosis.
Transforming Growth Factor-beta (TGF-β): Elevated by 71.7%, TGF-β highlighted advanced fibrosis and tumor progression, posing a higher risk for HCC development.
Vascular Endothelial Growth Factor (VEGF): Elevated by 35.9%, VEGF was associated with increased angiogenesis, essential for tumor growth and metastasis, indicating higher malignant potential (Figure #3).
Liquid Biopsy Findings in LI-RADS 4 LesionsCirculating Tumor Cells (CTCs): CTCs were detected in 17.85% of patients with LI-RADS 4 lesions. The presence of CTCs in the bloodstream is a critical indicator of tumor spread and metastasis. In this cohort, patients with detectable CTCs were considered to be at high risk for aggressive HCC, and this finding significantly influenced treatment decisions.The detection of CTCs correlated well with the imaging characteristics of LI-RADS 4 lesions, supporting the probable HCC classification.
Circulating Tumor DNA (ctDNA): ctDNA was elevated in 32.14% of patients with LI-RADS 4 lesions. ctDNA reflects the presence of tumor-specific genetic mutations in the bloodstream, and its detection provided molecular confirmation of malignancy. Patients with elevated ctDNA levels were more likely to have confirmed HCC upon histopathological examination. The combination of elevated ctDNA and serum biomarkers such as AFP, HGF, and VEGF significantly strengthened the case for malignancy in LI-RADS 4 patients (Figure #4).
Correlation of Biomarkers with HCC Diagnosis
This study evaluated the correlation between serum biomarkers, liquid biopsy findings, and histopathological confirmation of hepatocellular carcinoma (HCC) in LI-RADS 3 and LI-RADS 4 patients.
LI-RADS 3 Lesions
Among patients with LI-RADS 3 lesions, 14.1% were confirmed to have HCC. These patients showed elevated levels of AFP, LDH, HGF, IL-6, and TGF-β, even when ctDNA and CTCs were not detected. This highlights the importance of serum biomarkers in identifying malignancy risk, suggesting that liquid biopsy markers may appear later in the disease course.
Elevated HGF and TGF-β levels were linked to underlying fibrosis or tumor growth, indicating potential progression toward malignancy.
LI-RADS 4 Lesions
In LI-RADS 4 patients, 17.85% had elevated biomarkers, including AFP, LDH, HGF, IL-6, and TGF-β, which were associated with confirmed HCC. The presence of ctDNA and CTCs further reinforced the likelihood of malignancy, highlighting a more aggressive or metastatic disease.
The integration of liquid biopsy results, especially ctDNA detection, helped identify tumor-specific mutations, offering insights into the tumor's molecular characteristics and potential therapeutic targets.
Comparing biomarkers between LI-RADS 3 and LI-RADS 4 lesions revealed distinct patterns, assisting in differentiating intermediate probability (LI-RADS 3) from probable HCC (LI-RADS 4), as shown in Table #2.
Correlation of Biomarkers with HCC Diagnosis
The correlation of serum biomarkers and liquid biopsy findings with histopathological confirmation of HCC was a central focus of this study. In both LI-RADS 3 and LI-RADS 4 patients, the use of a comprehensive biomarker panel, along with advanced liquid biopsy techniques, allowed for a more accurate assessment of the malignant potential of liver lesions.
LI-RADS 3 Lesions
Among patients with LI-RADS 3 lesions, 14.1% were confirmed to have primary liver cancer (HCC) upon histopathological examination. These patients exhibited elevated levels of AFP, LDH, HGF, IL-6, and TGF-β, even in the absence of elevated ctDNA or CTCs. This finding suggests that while liquid biopsy markers such as ctDNA and CTCs are useful, the combination of serum biomarkers remains essential for identifying patients at risk for malignancy
Patients with elevated HGF and TGF-β were more likely to have underlying fibrosis or active tumor growth, which contributed to the progression of their lesions toward malignancy. The absence of ctDNA or CTCs in these patients indicates that these biomarkers may appear later in the disease course, particularly when metastasis becomes a concern.
LI-RADS 4 Lesions
In LI-RADS 4 patients, 17.85% had elevated levels of AFP, LDH, HGF, IL-6, and TGF-β, all of which were associated with histopathologically confirmed HCC. The signifi- cant elevation of these biomarkers, particularly in conjunction with ctDNA and CTC detection, strongly indicated the presence of malignancy. The combination of these biomarkers provided a more comprehensive picture of the disease and helped clinicians distinguish between probable HCC and other benign conditions that may present with similar imaging findings.
Notably, patients with elevated ctDNA and CTCs were at higher risk for aggressive or metastatic disease. These findings underscored the importance of integrating liquid biopsy results into the diagnostic workflow for patients with LI-RADS 4 lesions. The use of ctDNA in particular allowed for the identification of tumor-specific mutations, providing insights into the molecular characteristics of the tumor and potential therapeutic targets.
we can compare the biomarkers between LI-RADS 3 and LI-RADS 4 lesions to highlight differences in biomarker patterns and elevations, which can help differentiate between intermediate probability (LI-RADS 3) and probable hepatocellular carcinoma (LI-RADS 4), (Table #2).
Key Differences Between LI-RADS 3 and LI-RADS 4Biomarkers
This table, titled "Comparison of Biomarker Elevations Between LI-RADS 3 and LI-RADS 4 Lesions," presents a detailed comparison of biomarker levels in patients with liver lesions classified as LI-RADS 3 and LI-RADS 4. These classifications indicate intermediate (LI-RADS 3) and probable (LI-RADS 4) malignancy probabilities for hepatocellular carcinoma (HCC).
Table Layout and Description
Biomarker: The First column lists various biomarkers analyzed in the study. These biomarkers are selected based on their relevance to liver disease and cancer, with some commonly associated with inflammation, metabolic activity, or tumor presence
LI-RADS 3 Elevation (%): This column shows the percentage increase in each biomarker level in patients with LI-RADS 3 lesions. The values indicate how much the biomarkers are elevated compared to normal ranges.
LI-RADS 4 Elevation (%): Similar to the LIRADS 3 column, this column presents the percentage increase for each biomarker in LI-RADS 4 patients, providing a comparison to understand if LI-RADS 4 lesions are associated with higher biomarker elevations, which may correlate with greater malignancy risk.
Difference (%): This column calculates the difference between the elevations in LI-RADS 4 and LI-RADS 3. A positive value indicates a higher increase in LI-RADS 4, while a negative value would suggest higher elevation in LIRADS 3. This comparison helps highlight which biomarkers are notably elevated in probable HCC cases (LI-RADS4).
P-value: The p-value indicates the statistical significance of the differences observed between the two LIRADS groups. Lower p-values (< 0.05) suggest that the differences in biomarker levels between LI-RADS 3 and LI-RADS 4 are statistically significant and unlikely due to chance.
95% Confidence Interval (CI): The confidence interval for each biomarker shows the range within which the true difference in elevations between the groups is likely to lie, with 95% confidence. Narrow intervals indicate more precise estimates, providing context for the reliability of the findings.
Key Observations: Biomarkers like HGF (Hepatocyte Growth Factor), TGF-β (Transforming Growth Factor Beta), and AFP-L3 show substantial elevation differences between LI-RADS 3 and LI-RADS 4, with high statistical significance (low p-values).
AFP and AFP-L3 have greater elevations in LIRADS 4, suggesting their potential as specific markers of HCC in probable cases.
Inflammatory markers such as IL-6 show higher elevation in LI-RADS 4 lesions, indicating a stronger inflammatory response potentially linked to malignancy progression.
Metabolic and angiogenic markers like LDH and VEGF also have higher levels in LI-RADS 4, supporting their role in malignancy and angiogenesis associated with tumor growth.
Overall, the table provides a comprehensive, comparative analysis of biomarker elevations in LI-RADS 3 and LI-RADS 4 lesions, supporting their use in stratifying patients based on malignancy risk.
This comparison reveals that biomarkers such as AFP-L3, HGF, IL-6, and TGF-β are more elevated in LIRADS 4 patients, indicating a higher likelihood of malignancy and more advanced liver disease. These differences can aid in distinguishing between LI-RADS 3 and LI-RADS 4 lesions, guiding decisions about biopsy, surveillance, and potential treatment.
Imaging Findings and Serum Biomarkers in LIRADS 4 Lesions
For LI-RADS 4 lesions, the imaging characteristics suggest a high probability of malignancy, often indicative of early HCC. The lesions typically show more pronounced arterial phase hyperenhancement (APHE), with late-phase nonperipheral washout and the presence of enhancing capsule.
Serum biomarker findings for LI-RADS 4 patients showed that 25% had elevated AFP levels, with a mean value of 211 ng/mL. AFP-L3 levels were elevated in 46.42% of patients, with additional increases in LDH, HGF, and IL-6.
Biomarker Patterns in LI-RADS 3 and LI-RADS 4 Patients
Analyzing the biomarker trends in LI-RADS 3 and LI-RADS 4 patients helps differentiate between benign and malignant liver lesions.
Elevated Biomarkers
AFP:Both groups showed elevated AFP levels, but LI-RADS 4 patients had higher levels (mean 211 ng/mL vs. 119 ng/mL in LI-RADS 3), suggesting a stronger association with HCC.
AFP-L3: Increased by 48% in LI-RADS 4 patients compared to 33% in LI-RADS 3, highlighting its specificity for malignancy.
HGF and TGF-β: Both markers were elevated in LI-RADS 4 patients (90% HGF, 71.7% TGF-β) compared to LI-RADS 3 (77% HGF, 57.7% TGF-β), indicating more advanced disease in LI-RADS 4.
Inflammatory Markers
IL-6: Higher in LI-RADS 4 patients (47% vs. 27% in LI-RADS 3), suggesting more aggressive inflammation driven carcinogenesis.
CRP: Moderately elevated in both groups but slightly higher in LI-RADS 4 (9.9% vs. 8%).
Metabolic and Angiogenic Markers
LDH: Elevated in both groups, with LI-RADS 4 showing a higher increase (33% vs. 27% in LI-RADS 3), indicating increased metabolic activity.
VEGF: Higher in LI-RADS 4 (35.9% vs. 29.7% in LI-RADS 3), reflecting greater angiogenesis.
Liquid Biopsy Findings
ctDNA: Detected in 16.6% of LI-RADS 3 and 32.14% of LI-RADS 4 patients, suggesting a higher likelihood of malignancy in LI-RADS 4.
CTCs: Detected in 17.85% of LI-RADS 4 patients, none in LI-RADS 3, further indicating malignancy in LIRADS 4.
Combination of Biomarker and Liquid Biopsy Data
Elevated AFP, AFP-L3, and HGF, combined with ctDNA or CTCs, strongly indicated malignancy. In the absence of liquid biopsy markers, serum biomarkers proved useful earlier in disease progression.
Pattern Observations
LI-RADS 3: Moderate biomarker elevation with rare ctDNA/CTCs, suggesting premalignant conditions.
LI-RADS 4: Higher biomarker levels and presence of ctDNA/CTCs, indicating a higher malignancy risk and the need for early intervention.
Analyzing these biomarker patterns can help clinicians stratify patients more effectively, guiding decisions about surveillance, biopsy, and potential treatment strategies based on the risk of progression to HCC (Figure #5).
Summary of Findings
The results of this study demonstrate that serum biomarkers such as AFP, AFP-L3, LDH, HGF, IL-6, and TGF-β are significantly elevated in patients with both LIRADS 3 and LI-RADS 4 lesions, and their levels correlate strongly with histopathologically confirmed HCC. Liquid biopsy markers, including ctDNA and CTCs, further enhanced the diagnostic accuracy, particularly in patients with LI-RADS 4 lesions.
In LI-RADS 3 patients, the detection of elevated serum biomarkers was useful in identifying those at higher risk of malignant transformation, even in the absence of positive liquid biopsy results. In LI-RADS 4 patients, the combination of serum biomarkers and liquid biopsy findings provided a robust diagnostic tool for confirming HCC and assessing the likelihood of metastasis.
The integration of serum biomarkers and liquid biopsy results into the diagnostic workflow allowed for a more comprehensive evaluation of liver lesions and enabled clinicians to make more informed decisions about patient management, including the need for biopsy, surveillance, or treatment. The study highlights the value of a multimodal approach to the diagnosis of indeterminate liver lesions and provides a foundation for future research into the early detection and management of HCC.
Discussion
The use of biomarkers for the early detection and prediction of hepatocellular carcinoma (HCC) has become an integral component of modern liver cancer diagnosis and management. Early-stage liver cancer is often asymptomatic, and by the time clinical symptoms or significant imaging findings emerge, the disease may have already progressed to an advanced stage. This underscores the importance of utilizing biomarkers to identify early-stage liver cancer, enabling timely intervention and improved prognosis. This discussion highlights the role of various biomarkers, including serum proteins, circulating tumor markers, and liquid biopsy findings, in predicting early-stage liver cancer and their clinical implications.
1. Alpha-Fetoprotein (AFP) and AFP-L3 in Early Detection
AFP is one of the most widely studied and used biomarkers in the diagnosis of HCC. While it has been a cornerstone in liver cancer screening for decades, its limitations in sensitivity and specificity, especially in early-stage disease, have led to a search for complementary or alternative markers. AFP can be elevated in benign liver conditions such as cirrhosis or hepatitis, which reduces its specificity for cancer detection. However, in early-stage HCC, elevated AFP levels, particularly between 20-200 ng/mL, may still indicate the presence of malignant changes. Importantly, rising trends in AFP over time are particularly useful in surveillance programs for high-risk patients, where even mild elevations can prompt further imaging or diagnostic workups [2,3,4,5,24,33].
AFP-L3, a glycosylated isoform of AFP, has shown much greater specificity for HCC, particularly in early-stage disease. Unlike total AFP, AFP-L3 is more specific for malignant lesions and is able to distinguish between benign liver conditions and cancer. In early-stage HCC, even if AFP levels are within normal ranges, an elevated percentage of AFP-L3 can suggest early tumor activity, which may otherwise go undetected. This highlights the utility of AFP-L3 in the early detection of liver cancer and the need to incorporate it into routine screening programs for at-risk populations [1,2,4,26,31,33].
2. Des-Gamma-Carboxy Prothrombin (DCP) and Glypican-3 (GPC3) for Improved Specificity
DCP (or PIVKA-II) has emerged as a highly specific biomarker for detecting HCC, including in the early stages. Its elevation is linked to vascular invasion, a hallmark of aggressive liver cancer, and its detection can provide valuable information even when AFP is normal. Studies have shown that DCP is sensitive to early-stage tumors and can help identify patients with a high risk of progression. The ability of DCP to detect small, early-stage tumors makes it an excellent complementary marker to AFP, improving the overall diagnostic accuracy for early-stage HCC [2,8,15,19].
GPC3 is another promising biomarker for early HCC. Unlike AFP, which is produced by both normal and malignant hepatocytes, GPC3 is specifically overexpressed in HCC cells, making it highly specific for malignant liver lesions. Its presence in early-stage tumors provides a strong indication of cancer, and combining GPC3 with AFP or DCP significantly enhances the sensitivity and specificity of early-stage liver cancer detection. GPC3’s role as a diagnostic tool for early-stage HCC is particularly useful when AFP levels are normal, underscoring its importance in a multi-biomarker approach [11,26,31,32].
3. MicroRNAs (miRNAs) as Emerging Early Detection Tools
MicroRNAs (miRNAs) represent a novel class of biomarkers that have shown considerable promise in the detection of early-stage HCC. Specific miRNAs, such as miR-122, miR-21, and miR-221, have been found to be dysregulated in patients with liver cancer. miR-122, in particular, is liver-specific and is often downregulated in early HCC, making it a useful indicator of early tumorigenesis. The potential of miRNAs lies in their ability to reflect specific gene expression changes associated with cancer progression. Their detection in blood samples through non-invasive techniques offers an exciting new avenue for early cancer detection [1,2,5,22,30].
Furthermore, miRNAs are highly stable in serum, making them suitable candidates for routine clinical use. The development of miRNA panels for HCC screening is ongoing, but early studies suggest that miRNAs could significantly enhance early detection when combined with traditional biomarkers like AFP and DCP. Their ability to reflect early changes at the molecular level makes them a promising tool for detecting liver cancer in high-risk patients, particularly those with underlying chronic liver disease [2,8,30,33].
4. Liquid Biopsy: Circulating Tumor Cells (CTCs) and Circulating Tumor DNA (ctDNA)
Liquid biopsy has revolutionized cancer diagnostics, offering a minimally invasive method for detecting tumor-specific markers in the bloodstream. CTCs, which are cancer cells shed from primary tumors into circulation, can be detected even in early-stage liver cancer. While more commonly associated with advanced disease, detecting CTCs in early-stage HCC provides critical information about the potential for metastasis and aggressive disease behavior. CTC detection can complement imaging and other biomarkers by offering real-time insights into tumor activity [17,19,31].
Similarly, circulating tumor DNA (ctDNA) offers a non-invasive way to detect tumor-specific genetic mutations in patients with early-stage HCC. ctDNA is released into the bloodstream by cancer cells, and its detection can provide molecular confirmation of malignancy even before imaging findings become apparent. The ability of ctDNA to reveal specific mutations, such as those in the TERT promoter or TP53 genes, is particularly valuable in identifying early-stage cancer. ctDNA can be used to monitor disease progression, guide personalized treatment strategies, and detect minimal residual disease following treatment [1,21,22].
5. Inflammatory Markers (IL-6, CRP) and Their Role in Carcinogenesis
Chronic inflammation is a well-known driver of carcinogenesis in the liver, particularly in patients with cirrhosis or chronic hepatitis. Inflammatory markers like IL-6 and CRP are often elevated in these patients and can provide insights into the risk of malignant transformation. IL-6, a pro-inflammatory cytokine, promotes tumor growth by creating an environment conducive to cancer progression. Elevated IL-6 levels in patients with chronic liver disease may signal the onset of early-stage HCC, while CRP re- effects a more systemic inflammatory response. Although these markers are not specific to HCC, they offer important context for understanding the patient’s overall risk of developing liver cancer [26,31].
Incorporating a multi-biomarker approach into liver cancer screening, particularly for high-risk populations, can significantly improve the early detection of HCC. While AFP remains a useful marker, combining it with other biomarkers such as AFP-L3, DCP, GPC3, miRNAs, CTCs, and ctDNA enhances the sensitivity and specificity of early-stage cancer detection. This approach allows for more accurate stratification of patients at risk for HCC and enables earlier intervention, improving long-term survival outcomes. By utilizing biomarkers in conjunction with imaging and clinical evaluation, clinicians can better identify liver cancer in its early stages, leading to better prognosis and treatment success [1,22,33].
Analyzing biomarker patterns in patients with LIRADS 3 and LI-RADS 4 lesions provides insights into differentiating benign from malignant liver lesions.
Elevated Biomarkers in LI-RADS 3 vs. LI-RADS 4Patients
AFP: Both groups had elevated AFP levels, but they were significantly higher in LI-RADS 4 patients (211 ng/mL vs. 119 ng/mL in LI-RADS 3), suggesting a stronger association with HCC.
AFP-L3: AFP-L3 increased more in LI-RADS 4 patients (48% vs. 33% in LI-RADS 3), reinforcing its link to probable malignant lesions.
HGF and TGF-β: Both growth factors were elevated in LI-RADS 4 patients, with HGF increasing by 90% and TGF-β by 71.7%, indicating a more aggressive tumor profile.
Patterns of Inflammatory Markers
IL-6: This pro-inflammatory marker was more elevated in LI-RADS 4 patients (47% vs. 27% in LI-RADS 3), suggesting a stronger inflammatory response and tumor progression.
CRP: CRP levels were moderately elevated in both groups, but slightly higher in LI-RADS 4 patients (9.9% vs. 8%), indicating more systemic inflammation.
Metabolic and Angiogenic Markers
LDH: Elevated in both groups, but slightly higher in LI-RADS 4 patients (33% vs. 27%), indicating increased metabolic activity consistent with malignancy.
VEGF: Notably elevated in LI-RADS 4 patients (35.9% vs. 29.7% in LI-RADS 3), suggesting that VEGF is more associated with malignant neovascularization.
Liquid Biopsy Findings
ctDNA: Detected in 16.6% of LI-RADS 3 and 32.14% of LI-RADS 4 patients, with a higher detection rate in LI-RADS 4, indicating more genetic alterations in probable malignant lesions.
CTCs: No CTCs were found in LI-RADS 3 patients, while 17.85% of LI-RADS 4 patients had detectable CTCs, strongly correlating with malignancy.
Combining Biomarker and Liquid Biopsy Data
Elevated biomarkers, particularly AFP, AFP-L3, and HGF, combined with positive ctDNA or CTCs in LIRADS 4 patients, indicate a higher likelihood of malignancy. In contrast, LI-RADS 3 lesions showed fewer alterations, suggesting they may represent premalignant conditions.
In summary, LI-RADS 4 patients consistently exhibit higher levels of biomarkers and liquid biopsy markers, indicating a higher risk of malignancy, while LI-RADS 3 lesions show less pronounced changes. These patterns provide a more comprehensive assessment of lesion progression, helping guide early intervention and management strategies for potential HCC cases [1,2,3,5,7,32,33].
The results of this study offer clinicians a practical framework for enhancing the early detection and management of hepatocellular carcinoma (HCC), particularly for indeterminate liver lesions classified as LI-RADS 3 and LIRADS 4. Through the integration of imaging, serum biomarkers, and liquid biopsy techniques, this multi-modal approach can be transformed into a diagnostic and monitoring algorithm that is both non-invasive and reliable, improving early HCC detection rates and patient outcomes. Here’s how clinicians can apply these findings in practice:
1. Early Detection and Monitoring Algorithm
By establishing a structured algorithm based on biomarker levels, liquid biopsy markers, and imaging results, clinicians can refine their diagnostic and monitoring approach. For example:
Step 1: Initial Imaging and Biomarker Assessment – Patients at risk of HCC undergo imaging (MRI or CT) alongside baseline biomarker evaluation, including alpha-fetoprotein (AFP), AFP-L3, HGF, and IL-6. Patients with LIRADS 3 and elevated biomarkers may be flagged for closer monitoring due to higher malignancy potential.
Step 2: Serial Biomarker Tracking – Patients identified with LI-RADS 3 or LI-RADS 4 lesions would have regular biomarker assessments. An increase in markers like AFP-L3 or the appearance of ctDNA can prompt more intensive follow-up.
Step 3: Liquid Biopsy Confirmation – Detection of ctDNA or CTCs in patients with suspicious biomarkers and imaging results can guide the decision to proceed with further interventions, such as biopsy or localized treatment.
This algorithm can reduce the need for invasive procedures and ensure that high-risk patients are identified and managed promptly.
2. Tailored Surveillance Protoco
The study’s findings allow for the development of more individualized surveillance protocols. For instance:
Patients with moderate elevations in biomarkers but inconclusive imaging (LI-RADS 3) may undergo follow-up imaging and biomarker checks at shorter intervals.
For LI-RADS 4 patients with significantly elevated HGF and IL-6 or the presence of ctDNA, clinicians might recommend immediate diagnostic biopsy or direct treatment options, such as ablation or resection, given the higher likelihood of malignancy.
This individualized approach reduces unnecessary procedures for low-risk patients while enabling early intervention for high-risk cases, potentially improving survival rates.
3. Non-Invasive Early Detection
This study emphasizes the utility of combining serum biomarkers and liquid biopsy markers with imaging, making it possible to detect malignancy at an earlier stage than imaging alone might allow. Non-invasive methods like these are particularly beneficial in high-risk patients with cirrhosis or chronic liver disease, where early-stage HCC detection is essential for curative treatment options. For instance:
An algorithm could prioritize LI-RADS 3 patients with rising AFP-L3 and detectable ctDNA for more rigorous monitoring, while other LI-RADS 3 cases with stable biomarkers may continue routine surveillance.
Early intervention in these cases, while the lesion is small, can significantly impact prognosis, as early HCC is more responsive to treatment and offers a better chance of long-term remission.
4. Supporting Personalized Medicine
The study provides clinicians with the tools needed for personalized patient care based on biomarker profiles and genetic markers found in ctDNA. Patients can receive individualized treatment plans that match their unique risk profiles, which are identified through multi-modal assess ments: For example, patients with LI-RADS 4 lesions showing high levels of VEGF and HGF may benefit from anti-angiogenic therapies alongside local interventions. Additionally, identifying specific tumor mutations through ctDNA can allow for targeted therapies, improving outcomes and potentially reducing side effects by avoiding less effective treatments.
5. Informing Clinical Guidelines
This study’s multi-modal approach offers a model that could be incorporated into liver cancer management guidelines, standardizing how biomarkers, liquid biopsy results, and imaging are used together to stratify patients based on malignancy risk. Such guidelines could recommend initial imaging with serum biomarkers, followed by liquid biopsy if initial results are inconclusive. This approach would help clinicians balance the need for early detection with the avoidance of unnecessary invasive procedures.
6. Improved Patient Outcomes
Early detection facilitated by this comprehensive approach directly impacts patient outcomes by identifying cancer in its early stages, when it is more treatable. Early intervention options, including resection or ablation, offer a higher likelihood of curative treatment. This strategy also allows for ongoing monitoring through liquid biopsies and biomarker assessments, offering a non-invasive option for tracking disease progression or recurrence.
This study presents a promising foundation for advancing hepatocellular carcinoma (HCC) detection and management through a multi-modal approach integrating imaging, serum biomarkers, and liquid biopsy. The further research will befocus on validating these biomarkers in larger, diverse populations and exploring additional novel biomarkers to improve diagnostic accuracy and therapeutic guidance.
1. Validation in Larger Cohorts
One essential step is to validate the findings across larger, multicenter cohorts that encompass a wider range of demographics, including patients with different etiologies of liver disease, such as viral hepatitis, non-alcoholic fatty liver disease (NAFLD), and alcoholic liver disease. Expanding the study population can help to us determine whether the observed biomarker patterns are consistent across various patient profiles and disease backgrounds. Additionally, larger studies can examine the sensitivity and specificity of each biomarker, such as AFP-L3, HGF, and IL-6, in predicting early HCC, enhancing the clinical applicability of these biomarkers. A well-validated biomarker panel with consistent predictive values can then be integrated into routine practice for HCC screening and monitoring, increasing confidence in non-invasive methods for early detection.
2. Longitudinal Studies for Prognostic Value
Future studies should also adopt a longitudinal approach, tracking patients over time to better understand how biomarker levels evolve as HCC progresses. By regularly monitoring biomarkers in LI-RADS 3 and LI-RADS 4 patients, researchers can identify which markers are most predictive of progression to overt malignancy. This approach would also help to us distinguish biomarkers that are transiently elevated due to liver inflammation or other benign conditions, refining the interpretation of biomarker fluctuations. Such longitudinal data could provide insights into optimal timing for surveillance and intervention, potentially allowing clinicians to personalize follow-up protocols based on individual biomarker trends.
3. Exploration of Novel Biomarkers
Emerging biomarkers, including microRNAs (miRNAs) and extracellular vesicles, have shown potential in detecting and monitoring cancer progression. For instance, specific miRNAs such as miR-122 and miR-21 are known to be involved in liver carcinogenesis and could serve as adjunct markers for early HCC. Exploring combinations of these novel biomarkers with traditional serum markers like AFP and AFP-L3 could create a more comprehensive biomarker panel with improved accuracy for early detection. Extracellular vesicles, which contain DNA, RNA, and proteins shed by tumor cells, represent another promising avenue for non-invasive HCC diagnostics, particularly in detecting genetic alterations that may not be evident in blood- -based liquid biopsy.
4. Investigation of Biomarker Interactions
Understanding the interactions between biomarkers and their combined effect on HCC detection and progression is another critical area for further research. For instance, investigating how markers like HGF and TGF-β interact with inflammatory markers (e.g., IL-6 and CRP) could provide insight into the biological pathways driving HCC. Research could examine whether certain biomarker combinations are associated with specific genetic mutations, thereby offering potential therapeutic targets. These insights could guide clinicians in selecting targeted therapies for patients based on their biomarker profile, moving towards personalized treatment strategies in HCC management.
5. Biomarker-Guided Treatment Response Studies
Biomarkers can also play a role in monitoring response to treatment. Further studies could investigate whether certain biomarkers, such as ctDNA or CTCs, decrease in response to therapies like transarterial chemoembolization (TACE) or systemic treatments. If successful, these biomarkers could serve as non-invasive tools for evaluating treatment efficacy, potentially reducing the need for follow-up biopsies and invasive testing. For example, declining ctDNA levels post-treatment could indicate tumor shrinkage or remission, allowing for timely adjustments in therapy.
6. Integration with Machine Learning
The application of machine learning to analyze biomarker and imaging data is a promising direction for research. Using machine learning algorithms, researchers can identify complex patterns within large biomarker datasets and imaging findings, potentially unveiling new predictive markers for early HCC detection. By integrating multi-modal data, machine learning could enhance diagnostic algorithms, creating predictive models that clinicians can apply in real-time to assess malignancy risk. This technology could also facilitate the development of risk stratification tools, guiding clinicians in tailoring follow-up and treatment plans based on individual risk profiles.
7. International Guidelines and Consensus Studies
As biomarkers gain validation, further research should focus on establishing international guidelines for their use in clinical practice. This would involve consensus studies across multiple regions, particularly those with high HCC incidence, to harmonize biomarker cut-off values and protocols for HCC surveillance. Consistent guidelines would ensure that patients globally benefit from validated, reliable biomarker-driven strategies, standardizing care and improving early HCC detection.
In summary, while this study offers an effective multi-modal approach to HCC detection, further research is necessary to validate these biomarkers in larger populations and explore additional markers that could enhance diagnostic precision. Longitudinal studies, exploration of novel biomarkers, and biomarker-guided treatment response monitoring will be essential in advancing this field. Through these future studies, a more refined, non-invasive diagnostic and monitoring framework can be developed, ultimately improving outcomes for patients at risk of HCC.
Conclusion
This study emphasizes the importance of utilizing a multi-modal approach that integrates serum biomarkers, liquid biopsy markers, and imaging findings for the effective assessment and management of LI-RADS 3 and 4 lesions, particularly in patients at risk for hepatocellular carcinoma (HCC). LI-RADS 3 and 4 lesions represent a diagnostic challenge due to their intermediate and probable likelihood of malignancy. Traditionally, imaging findings alone have been the cornerstone of liver lesion assessment. However, this study demonstrates that incorporating serum biomarkers and liquid biopsy technologies can enhance the detection of early-stage HCC and improve the clinical management of indeterminate liver lesions.
1. Serum Biomarkers and Their Diagnostic Utility
Serum biomarkers such as alpha-fetoprotein (AFP), AFP-L3, hepatocyte growth factor (HGF), and interleukin-6 (IL-6) have long been associated with liver cancer detection, particularly HCC. This study reaffirms their critical role in the diagnostic process, especially when assessing LIRADS 3 and 4 lesions. While AFP remains a widely used marker, its limitations in sensitivity and specificity are well documented, particularly in early-stage liver cancer. However, combining AFP with its isoform AFP-L3 provides enhanced diagnostic accuracy, as AFP-L3 is more specific to HCC. This study found that elevated levels of AFP-L3, especially when combined with raised AFP levels, are strong indicators of probable malignancy in LI-RADS 4 lesions.
In addition, growth factors such as HGF and inflammatory markers like IL-6 are shown to have diagnostic value, especially in predicting malignancy in indeterminate liver lesions. HGF, which is involved in liver regeneration and tumor growth, was significantly elevated in patients with LI-RADS 4 lesions, suggesting that its inclusion in routine clinical evaluations can help identify patients at risk of malignant transformation. Similarly, IL-6’s role as a pro-inflammatory cytokine linked to chronic inflammation and tumorigenesis underscores its importance in predicting liver cancer progression. These biomarkers, in combination with imaging, provide a more nuanced understanding of the biology of liver lesions and help to stratify patients based on their risk for HCC.
2. Liquid Biopsy Markers: ctDNA and CTCs
The advent of liquid biopsy technologies, particularly circulating tumor DNA (ctDNA) and circulating tumor cells (CTCs), offers a significant breakthrough in the non-invasive monitoring of liver cancer. This study underscores the potential of ctDNA and CTCs in providing molecular insights into liver lesions that imaging alone cannot capture. In LI-RADS 4 lesions, ctDNA was elevated in a substantial proportion of patients, indicating tumor-specific genetic alterations that suggest malignant transformation. The presence of ctDNA, even in the absence of significant imaging changes, can serve as an early molecular marker of hepatocarcinogenesis, allowing for earlier diagnosis and intervention.
CTCs, which are indicative of tumor dissemination and metastatic potential, were detected in a notable percentage of patients with LI-RADS 4 lesions. Their presence correlates strongly with tumor aggressiveness and the likelihood of progression to advanced HCC. The detection of CTCs provides a valuable tool for identifying patients at risk for metastasis and guiding more personalized treatment strategies. By combining ctDNA and CTC analysis with traditional biomarkers, clinicians can gain a comprehensive view of the molecular landscape of liver lesions, facilitating more accurate diagnoses and tailored treatment plans.
3. The Future of Biomarker-Driven Personalized Treatment
This study suggests that the integration of serum biomarkers and liquid biopsy markers into routine clinical practice could revolutionize the management of liver lesions, particularly those classified as LI-RADS 3 and 4. The ability to detect molecular alterations, assess tumor biology, and predict malignancy through non-invasive means opens new avenues for personalized medicine in liver cancer. With further research and validation, biomarker-driven approaches could lead to the development of individualized treatment plans, where patients receive tailored interventions based on their specific tumor biology and genetic pro- files.
In conclusion, this study highlights the value of combining traditional serum biomarkers, such as AFP, AFP-L3, HGF, and IL-6, with cutting-edge liquid biopsy markers like ctDNA and CTCs. This multi-modal approach offers a more comprehensive and precise method for detecting early-stage HCC, predicting tumor progression, and guiding personalized treatment strategies for patients with indeterminate liver lesions. Future studies should focus on validating these findings and expanding the role of biomarkers in the ongoing effort to improve early detection, prognosis, and treatment outcomes for liver cancer patients.
Acknowledgments
The authors are grateful to the Institute for Personalized Medicine for providing full-time access to genetics and molecular biology laboratories for a few weeks and Tbilisi State Medical University too.
Informed Consent Statement
Yes
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article and its supplementary materials.
Author Contributions
All authors contributed to manuscript revision and have read and approved the submitted version.
Funding
This work was supported by the Institute for Personalized Medicine – PMI, Tbilisi, Georgia
- Bruix J, Sherman M (2011) Management of hepatocellular carcinoma: an update. Hepatology. 53: 1020-2.
- Forner A, Reig M, Bruix J (2018) Hepatocellular carcinoma. Lancet. 391: 1301-14.
- Llovet JM, Burroughs A, Bruix J (2003) Hepatocellular carcinoma. Lancet. 362: 1907-17.
- Singal AG, Lampertico P, Nahon P (2020) Epidemiology and surveillance for hepatocellular carcinoma: New trends. J Hepatol. 72: 250-61.
- El-Serag HB, Kanwal F (2014) Epidemiology of hepatocellular carcinoma in the United States: Where are we? Where do we go? Hepatology. 60: 1767-75.
- Llovet JM, Kelley RK, Villanueva A, et al. (2021) Hepatocellular carcinoma. Nat Rev Dis Primers. 7: 6.
- Tabrizian P, Roayaie S, Schwartz ME (2014) Current management of hepatocellular carcinoma. World J Gastroenterol. 20: 10223-37.
- Sangiovanni A, Prati GM, Fasani P, et al. (2010) The diagnostic and economic impact of contrast-enhanced magnetic resonance imaging in cirrhotic patients with hepatocellular carcinoma. Gut. 59: 1083-9.
- European Association for the Study of the Liver (2018) EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J Hepatol. 69: 182-236.
- Kudo M (2015) Surveillance, diagnosis, and treatment of hepatocellular carcinoma: A systematic review. World J Gastroenterol. 21: 12784-96.
- Tzartzeva K, Obi J, Rich NE, et al. (2018) Surveillance Imaging and Alpha Fetoprotein for Early Detection of Hepatocellular Carcinoma in Patients With Cirrhosis: A Meta-analysis. Gastroenterology. 154: 1706-18.e1.
- Merle P, Cheng AL, Roskams T, et al. (2012) Biology and therapeutic options for hepatocellular carcinoma. Gastroenterology. 142: 1264-73.
- Sherman M (2010) Hepatocellular carcinoma: epidemiology, surveillance, and diagnosis. Semin Liver Dis. 30: 3-16.
- Nault JC, Galle PR, Marquardt JU (2018) The role of molecular enrichment on future therapies in hepatocellular carcinoma. J Hepatol. 69: 237-47.
- Kudo M, Han KH, Ye SL, et al. (2020) A changing paradigm for the treatment of intermediate-stage hepatocellular carcinoma: Asia-Pacific primary liver cancer expert consensus statements. Liver Cancer. 9: 245-60.
- Forner A, Llovet JM, Bruix J (2012) Hepatocellular carcinoma. Lancet. 379: 1245-55.
- Mokdad AA, Singal AG, Yopp AC (2017) Advances in imaging and biomarkers for hepatocellular carcinoma. Hepatoma Res. 3: 55-63.
- Reig M, Forner A, Rimola J, et al. (2022) BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J Hepatol. 76: 681-93.
- Cheng AL, Kang YK, Chen Z, et al. (2009) Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 10: 25-34.
- Llovet JM, Ricci S, Mazzaferro V, et al. (2008) Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 359: 378-90.
- Galle PR, Tovoli F, Foerster F, et al. (2017) The treatment of intermediate stage tumours beyond TACE: From surgery to systemic therapy. J Hepatol. 67: 173-83.
- Bruix J, Han KH, Gores G, et al. (2015) Liver cancer: Approaching a personalized care framework. J Hepatol. 62.
- Abou-Alfa GK, Meyer T, Cheng AL, et al. (2018) Cabozantinib in patients with advanced and progressing hepatocellular carcinoma. N Engl J Med. 379: 54-63.
- Vogel A, Cervantes A, Chau I, et al. (2018) Hepatocellular carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 29.
- Finn RS, Qin S, Ikeda M, et al. (2020) Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 382: 1894-905.
- Galle PR, Forner A, Llovet JM, et al. (2018) EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J Hepatol. 69: 182-236.
- Pinyol R, Montal R, Bassaganyas L, et al. (2019) Molecular predictors of prevention of recurrence in patients with hepatocellular carcinoma treated with adjuvant sorafenib. Clin Cancer Res. 25: 7485-97.
- Frenette C, Gish R (2016) Targeted systemic therapies for hepatocellular carcinoma: clinical perspectives and implications. Asia Pac J Clin Oncol. 12: 319-29.
- Benson AB, D’Angelica MI, Abbott DE, et al. (2017) NCCN guidelines insights: hepatobiliary cancers, Version 1.2017. J Natl Compr Canc Netw. 15: 563-73.
- Llovet JM, Montal R, Sia D, Finn RS (2018) Molecular therapies and precision medicine for hepatocellular carcinoma. Nat Rev Clin Oncol. 15: 599-616.
- Shirabe K, Ishida T, Ueda K, et al. (2011) Hepatocellular carcinoma in a Japanese population: surgical treatment and prognostic factors. Hepatogastroenterology. 58: 206-11.
- Forner A, Vilana R, Ayuso C, et al. (2008) Diagnosis of hepatic nodules 20 mm or smaller in cirrhosis: prospective validation of the noninvasive diagnostic criteria for hepatocellular carcinoma. Hepatology. 47: 97-104.
- Zhu AX, Kang YK, Yen CJ, et al. (2019) Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased alpha-fetoprotein concentrations (REACH-2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 20: 282-96.
FIGURE 1
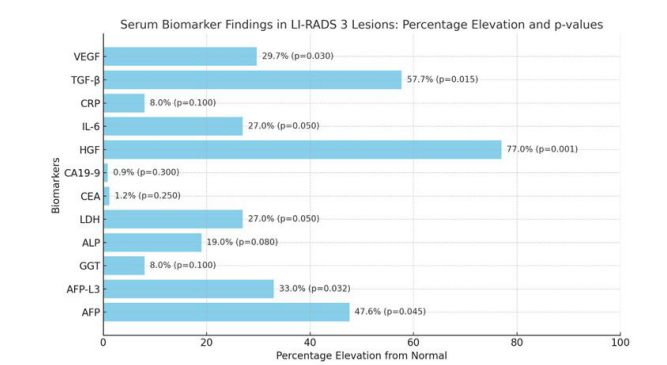
Figure 1: This figure illustrates the percentage elevation of various serum biomarkers in patients with LI-RADS 3 lesions. Each bar represents the percentage by which a specific biomarker is elevated compared to normal levels, and the associated p-values are displayed alongside the percentages. These p-values indicate the statistical significance of the differences observed, with lower p-values suggesting stronger evidence for the observed differences. For example, HGF shows the highest elevation at 77%, with a p-value of 0.001, indicating a strong association with LI-RADS 3 lesions. AFP also shows a significant elevation at 47.61%, with a p-value of 0.045, suggesting its potential role in identifying higher-risk patients. Biomarkers like CEA and CA19-9 show smaller percentage elevations and higher p-values, reflecting their lower diagnostic value in this cohort.This analysis can guide further investigation into the biomarkers most indicative of malignant transformation in LI-RADS 3 patients.
FIGURE 2
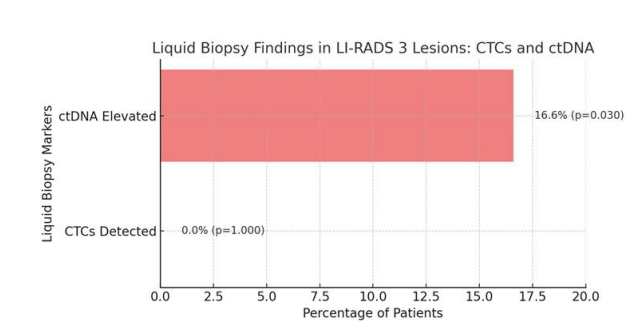
Figure 2: This figure highlights the liquid biopsy findings in patients with LI-RADS 3 lesions.The percentage of Patients with detectable circulating tumor cells (CTCs) is 0%, indicating no CTCs were found in this cohort, suggesting a low likelihood of metastasis at this stage. However, 16.6% of patients had elevated circulating tumor DNA (ctDNA), with a p-value of 0.03, suggesting a statistically significant presence of tumor-specific genetic alterations in a subset of these patients.The elevated ctDNA points to a higher risk of malignant transformation, making these patients candidates for closer monitoring and follow-up
FIGURE 3
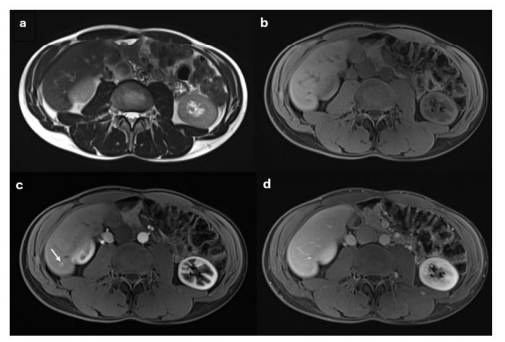
Image 1: Description: The above image demonstrates a LI-RADS 3 lesion. The lesion shows slight hyperintensity on T2-weighted imaging, with mild APHE but no definitive washout in the portal venous phase. The lesion measures less than 20 mm, further supporting its Classification as a LI-RADS 3 lesion.
FIGURE 4
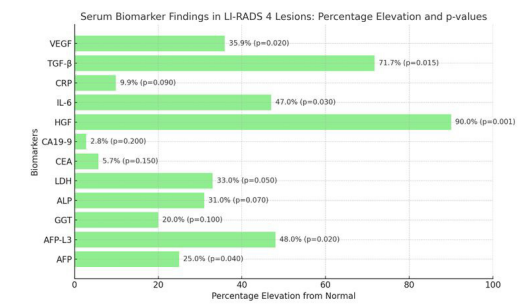
Figure 4: This figure presents the serum biomarker findings in patients with LI-RADS 4 lesions, showing the percentage elevation of each biomarker compared to normal levels. The associated p-values are displayed alongside the percentages, indicating the statistical significance of the elevations.
FIGURE 5
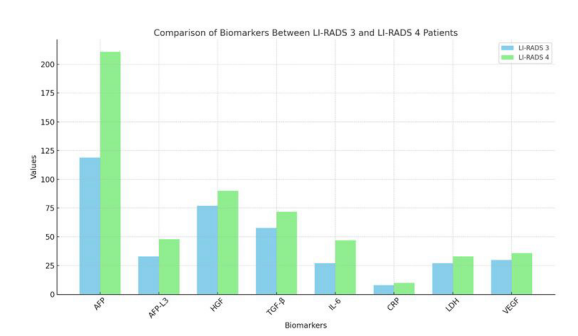
Figure 5: This figure compares the biomarker levels between patients with LI-RADS 3 and LI-RADS 4 lesions. Each biomarker shows different elevations between the two groups:
FIGURE 6
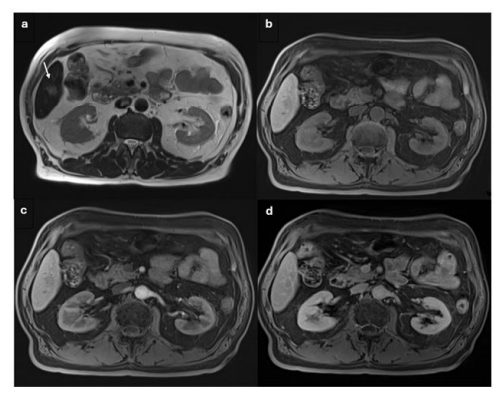
Image 2: Description:The image illustrates a LI-RADS 4 lesion, showing classic APHE with definite washout in the delayed phase.The lesion measures over 20 mm and demonstrates capsular retraction, highly suggestive of malignancy
FIGURE 7
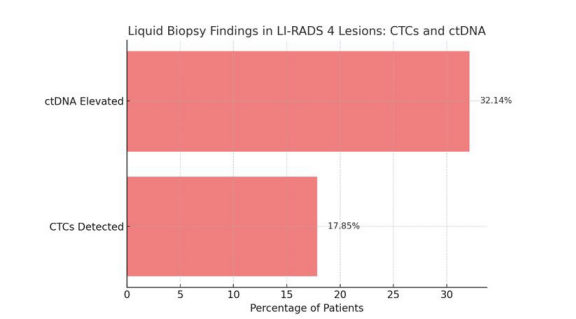
Figure 7: This figure represents the liquid biopsy fidings in patients with LI-RADS 4 lesions:
CTCs Detected: 17.85% of patients with LI-RADS 4 lesions had circulating tumor cells (CTCs) detected in their bloodstream, indicating a high risk of metastasis and aggressive HCC.
ctDNA Elevated: 32.14% of patients had elevated circulating tumor DNA (ctDNA), suggesting tumor-specific genetic mutations and a stronger likelihood of confirmed malignancy.
These liquid biopsy markers help provide additional molecular evidence of HCC in LI-RADS 4 patients, supporting imaging findings and influencing treatment strategies
Tables at a glance
Figures at a glance