Cutaneous Metastases in Paediatric Adrenal Neuroblastoma: A Rare Clinical Manifestation of a Common Childhood Malignancy
Received Date: February 28, 2026 Accepted Date: March 11, 2026 Published Date: March 14, 2026
doi:10.17303/jocr.2026.7.101
Citation: Noor Hasmira Bismi, Noor Diyana Osman, Nik Fatimah Salwati Nik Malek, Marlina Yusuf (2026) Cutaneous Metastases in Paediatric Adrenal Neuroblastoma: A Rare Clinical Manifestation of a Common Childhood Malignancy. J Oncol Clin Res 7: 1-8
Abstract
Neuroblastoma is the most common extracranial solid malignancy in infants and young children, typically originating from the adrenal glands. While metastatic spread is frequently present at diagnosis, cutaneous involvement is rare and may lead to diagnostic uncertainty due to its atypical presentation. We report a case of a 5-month-old female infant who presented with a one-month history of progressive abdominal distension by left labial swelling. Clinical examination revealed abdominal distension with firm subcutaneous nodules involving the left labia majora. Ultrasound and computed tomography (CT) showed a large left adrenal mass with associated soft tissue metastases to the labial region. Histopathological analysis confirmed cutaneous infiltration by neuroblastoma. Cutaneous metastasis in infants is uncommon and may be misinterpreted as a benign dermal or subcutaneous condition. This case emphasizes the critical role of radiological imaging in identifying the primary tumour and delineating the extent of metastatic spread. Clinicians and radiologists should maintain a high index of suspicion for metastatic disease in infants presenting with unusual soft tissue swellings. Early imaging evaluation and tissue biopsy are crucial to facilitate timely management and improve clinical outcomes.
Keywords: Neuroblastoma, Cutaneous Metastasis, Adrenal Neoplasms, Infant, Soft Tissue Swelling
Introduction
Neuroblastoma is the most common extracranial solid tumour in infancy and early childhood, accounting for approximately 7–11% of all paediatric cancers worldwide [1]. It is a significant childhood neoplasm, responsible for approximately 15% of all paediatric cancer-related deaths. Derived from neural crest–derived sympathetic tissues, it most commonly originates in the adrenal medulla (40%) or, less frequently, from the sympathetic ganglia in the abdomen, chest, or neck. The malignancy is characterised by its highly heterogeneous clinical behaviour, which ranges from spontaneous regression and differentiation to an aggressive, deadly metastatic course. While the median age at diagnosis is approximately 18 months, common sites of metastatic spread include the bone marrow, bone, liver, and lymph nodes [1].
In contrast, cutaneous metastases are distinctly uncommon, reported in fewer than 5% of neuroblastoma cases and predominantly affecting infants [2]. In the paediatric population, CMs are most frequently associated with neuroblastoma and rhabdomyosarcoma. Their presence typically signifies advanced disease and carries a poor prognosis, with a reported median survival of 7.98 months.
Furthermore, approximately 74% of patients with these skin lesions present with concomitant visceral metastases [6]. These cutaneous deposits usually manifest as firm, bluish to purplish subcutaneous nodules that may be easily mistaken for benign dermatological or congenital lesions, such as cysts or vascular malformations. This clinical uncertainty often delays appropriate diagnostic investigation. In the present case, the left labial swelling was initially presumed to represent a cystic lesion, resulting in an initial referral for gynaecological evaluation.
The aim of this case report is to describe the rare presentation of labial cutaneous metastasis as the primary indicator of adrenal neuroblastoma in an infant and to highlight the multi-modal diagnostic pathway required for accurate identification. This aim was achieved through the demonstration of (pathognomonic radiological findings and histopathological confirmation in establishing an accurate diagnosis [3].
Case Report
A 5-month-old female infant was brought to the hospital with a one-month history of progressive abdominal distension accompanied by swelling of the left labia majora. The parents reported no associated fever, weight loss, or changes in feeding pattern, although the abdomen had been increasing rapidly in size. The labial swelling was initially presumed to be a benign cystic lesion. On initial physical examinations, the infant appeared generally well but pale, with vital signs within normal limits for her age. Abdominal assessment revealed marked distension abdomen with a large, firm, non-tender mass palpable in the left upper quadrant extending across the midline. Examination of the left labia majora revealed a firm, non-mobile, ovoid subcutaneous nodule measuring approximately 2 x 1 cm, with overlying erythematous and slightly purplish skin changes. In view of these findings, which suggest for systemic or metastatic disease, the patient was urgently referred to the paediatric surgery team for further assessment.
Bedside ultrasound of the abdome revealed hepatomegaly with multiple suspicious hypoechoic liver lesions. A formal abdominal ultrasound was subsequently demonstrated gross hepatomegaly with multiple hypoechoic liver lesions suggestive of metastases. Additionally, a large left suprarenal mass, likely originating from the left adrenal gland, measuring approximately 6 cm in maximal dimension, was also identified. Ultrasound of the left labia majora showed a discrete subcutaneous lesion, raising strong suspicion for cutaneous metastasis.
Subsequent contrast-enhanced computed tomography (CT) of the abdomen confirmed a well-defined left adrenal mass with associated multifocal hepatic lesions and a firm left labial mass consistent with soft tissue metastasis. The primary tumour displaced the left kidney inferiorly and anteriorly. Blood tests revealed mild anemia, and further biochemical testing, including urinary catecholamine metabolites, was performed to confirm the diagnosis.
An ultrasound-guided biopsy of the left labial lesion was performed. Histopathological examination revealed features of differentiating neuroblastoma, characterized by small, round blue cells forming vague nests and neurofibrillary matrix, indicative of a low mitosis-karyorrhexis index (MKI). Immunohistochemical staining showed a strong positivity for neuroendocrine markers, including neuron-specific enolase (NSE) and synaptophysin, confirming the diagnosis of metastatic neuroblastoma.
The infant was subsequently referred to the paediatric oncology team for initiation of risk-adapted chemotherapy and supportive care based on the high- risk disseminated disease consistent with International Neuroblastoma Staging System (INSS) stage 4. A follow-up contrast-enhanced CT scan performed three months after commencement of chemotherapy demonstrated a slight reduction in the size of the left adrenal mass, accompanied by interval decreases in the multiple hepatic lesions and the left labia majora soft tissue lesion, indicating a partial response to the treatment.
This case highlights an unusual presentation of paediatric adrenal neuroblastoma with cutaneous metastasis manifesting as a left labial swelling with overlying erythematous skin changes. This case serves as a practical reminder that for infants with unusual symptoms, bridging the gap between initial confusion and a life-saving diagnosis requires us to rely on both detailed imaging and close communication between different medical specialties.
Discussion
Cutaneous metastases from neuroblastoma represent an uncommon clinical manifestation, reported in fewer than 5% of cases and most frequently observed in infants [2]. Their rarity and nonspecific clinical appearance often contribute to diagnostic delay or initial misdiagnosis, as seen in this case, in which the left labial swelling was initially considered to be a benign cystic lesion.
The early suspicion of a benign lesion was a direct result of how easily these rare metastatic patterns can mask a serious underlying malignancy in this age group. In infants, a swelling in the labia majora commonly raises differential diagnoses such as congenital cysts (e.g., hydrocele of the canal of Nuck), vascular malformations (e.g., hemangiomas or lymphangiomas), or infectious and inflammatory processes [3]. Given the firm consistency and overlying erythematous changes, other rare malignancies, such as rhabdomyosarcoma, must also be considered when evaluating soft tissue masses in the perineal region.
This case highlights the importance of maintaining a high index of suspicion for an underlying systemic malignancy when an infant presents with atypical soft tissue swellings, particularly in the context of systemic features such as abdominal distension. Early recognition of unusual metastatic patterns and prompt use of imaging and tissue diagnosis are essential to avoid delays in identifying neuroblastoma-associated cutaneous metastasis. The presence of cutaneous metastasis in neuroblastoma usually indicates advanced disease with extensive systemic dissemination. In this case, the concurrent hepatomegaly and multiple hepatic lesions further confirmed widespread metastatic involvement at presentation. Early imaging assessment, initially with ultrasound and subsequently with contrast-enhanced CT scanning, played a crucial role in delineating the primary adrenal tumour, characterising the metastatic burden, and guiding targeted biopsy and therapeutic planning.
Histopathological analysis confirmed a differentiating neuroblastoma subtype with a low mitosis-karyorrhexis index (MKI), a feature generally with more favourable biological behaviour compared with more aggressive variants [4]. Nevertheless, the presence of cutaneous metastasis is usually indicative of high-risk disease and correlates with poorer clinical outcomes, necessitating intensive multi-modal therapy.
The partial response observed on follow-up CT imaging three months after initiation of chemotherapy demonstrates that meaningful treatment responses are achievable, even in disseminated disease. This case serves as a practical lesson that catching these rare patterns early and ensuring precise staging are the most critical steps in starting the infant on the right therapeutic course. Given the diagnostic challenges posed by cutaneous metastases, particularly when they mimic benign lesions, this case emphasises the need for heightened clinical vigilance supported by comprehensive imaging and histopathological evaluation [5]. Increasing awareness of such atypical presentations among paediatricians, radiologists, and surgeons is essential to minimise diagnostic delays, facilitate timely intervention, and potentially improve clinical outcomes for children with neuroblastoma.
Conclusions
This case highlights an uncommon cutaneous manifestation of neuroblastoma, presenting as labial swelling in an infant and initially mimicking a benign lesion. The atypical clinical appearance contributed to early diagnostic misdirection, reminding us of the necessity for a high index of suspicion for malignancy when evaluating unusual soft tissue lesions in infants. The combination of rapid imaging and early biopsy served as the foundation for establishing an accurate diagnosis, allowing the initiation of the appropriate treatment course without delay [3]. Increased awareness of rare metastatic patterns, such as cutaneous involvement, among paediatric clinicians and radiologists is essential to facilitate earlier diagnosis and improve clinical outcomes in infants with advanced neuroblastoma.
Acknowledgement
The authors would like to express their sincere gratitude to Dr. Nik Fatimah Salwati binti Nik Malek, Consultant Radiologist and Head of the Department of Radiology, Hospital Sultanah Bahiyah, Kedah, Malaysia, for her invaluable guidance, support, and contributions throughout the preparation of this case report. Verbal informed consent was obtained from the patient’s legal guardian for publication of this case report and the accompanying images. No external funding was received for this work.
- Liu S, Yin W, Lin Y, et al. (2023) Metastasis pattern and prognosis in children with neuroblastoma. World J Surg Oncol. 21: 130.
- Maher-Wiese VL, Wenner NP, Grant-Kels JM (1992) Metastatic cutaneous lesions in children and adolescents with a case report of metastatic neuroblastoma. J Am Acad Dermatol. 26: 620-8.
- Suleiman DE, Adamu ZA, Mohammed A (2023) Multiple subcutaneous nodules leading to a diagnosis of neuroblastoma in an infant: a case report. Int J Med Health Dev. 28: 77-80.
- Nowak E, Ostojska M, Osial N, Psiuk D, Nurzyńska-Flak J (2024) Skin lesions as the first manifestation of metastatic neuroblastoma in infant – case report. J Pre-Clin Clin Res. 18: 246-9.
- Chu CM, Rasalkar DD, Hu YJ, Cheng FWT, Li CK, Chu WCW (2011) Clinical presentations and imaging findings of neuroblastoma beyond abdominal mass and a review of imaging algorithm. Br J Radiol. 84: 81-91.
- Starace M, Cedirian S, Rapparini L. (2025) Clinical Aspects of Cutaneous Metastasis from Non-Cutaneous Primary Tumors. Cancers 17: 3126.
FIGURE 1
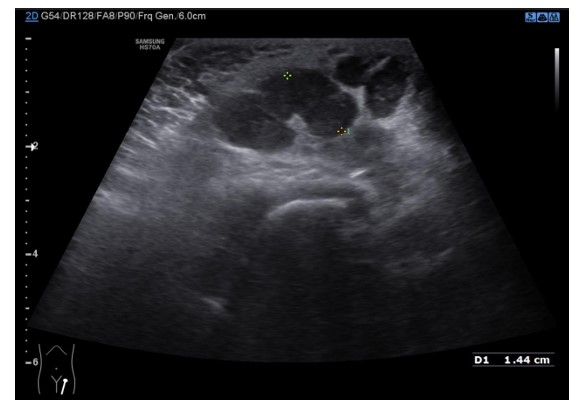
Figure 1: Ultrasound of the left labia majora demonstrating a well-defined, heterogeneous, predominantly hypoechoic solid mass. This sonographic appearance confirmed the lesion’s solid nature of the swelling, prompting subsequent tissue biopsy for definitive diagnosis.
FIGURE 2
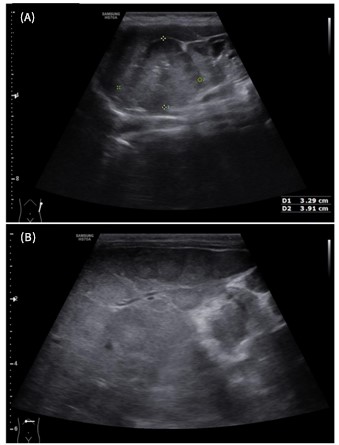
Figure 2: Abdominal ultrasound demonstrating the primary suprarenal mass and hepatic metastases. (A) Large, heterogeneous, predominantly solid mass arising from the left suprarenal region, consistent with the primary adrenal neuroblastoma. (B) Transverse ultrasound view of the liver illustrating gross hepatomegaly with numerous multifocal, hypoechoic nodules, characteristic of hepatic metastases at presentation.
FIGURE 3
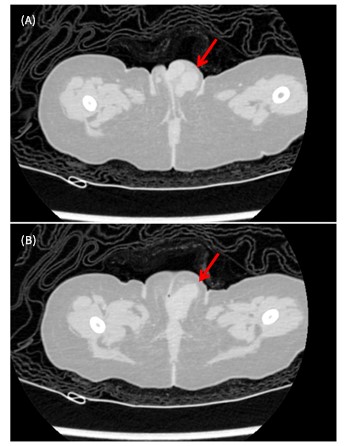
Figure 3: Comparative contrast-enhanced Computed Tomography (CT) images of the left labial metastasis. (A) Pre-treatment axial CT image demonstrating the well-defined, soft tissue density mass (arrow) within the subcutaneous tissue of the left labia majora. (B) Axial CT image of the same region obtained three months after initiation of chemotherapy, demonstrates a measurable reduction in size of the left adrenal mass (arrow), consistent with the partial systemic treatment response.
FIGURE 4

Figure 4: Comparative contrast-enhanced Computed Tomography (CT) images of the hepatic metastases. (A) Pre-treatment axial CT image of the upper abdomen illustrating significant hepatomegaly with multiple large, heterogeneous, enhancing hypodense masses, consistent with widespread metastatic neuroblastoma. (B) Axial CT image of the liver three months after commencing chemotherapy, showing a general decrease in the size and attenuation of the previously identified metastatic lesions, indicating a favorable partial systemic response to treatment.
Figures at a glance