Impact of Obesity on Respiratory Muscle Strength in Adult Females
Received Date: December 18, 2021 Accepted Date: January 18, 2022 Published Date: January 20, 2022
doi: 10.17303/jomd.2022.1.101
Citation: Jency thangasheela G (2022) Impact of Obesity on Respiratory Muscle Strength in Adult Females. J Obes Metab Dis 1: 1-12
Abstract
Introduction: Overweight or obesity can cause dangerous health problem and impair quality of life due to the change in lifestyle and lack of physical activity the problem of obesity is increasing by fast rate in 21st century. Obesity is important risk factor for diabetes, hypertension, atherosclerosis, cancer etc. it also cause disturbance in the respiratory functions.
Methodology: The number of subject involved the study is 60. Based on BMI of individuals the subjects are divided into 3 groups. Each group with 20 subjects. Maximum inspiratory pressure, maximum expiratory pressure, forced vital capacity and tidal volume are measured by using spirometer.
Result: The most common and consistent pulmonary function tests abnormality seen in obese individuals is a reduction in maximum inspiratory pressure, maximum expiratory pressure, forced vital capacity and tidal volume. Increased effort is needed to overcome respiratory system elasticity. Thus obese individuals need to do more respiratory work to maintain appropriate levels of ventilation.
Conclusions: The alterations in respiratory muscle strength by obesity were evidenced in the parameters maximum inspiratory pressure, maximum expiratory pressure, forced vital capacity and tidal volume, suggests that obesity affects to the respiratory mechanics. Overload of fat on respiratory muscles and chest region require more pressure during respiration. It may be prevented if active measure are taken to reduce weight by chance in lifestyle & food habits.
Keywords:Keywords: BMI; Respiratory Muscle Strength; Maximum Inspiratory Pressure; Maximum Expiratory Pressure; Forced Vital Capacity; Tidal Volume
Introduction
Obesity is the most common metabolic disease worldwide and its prevalence has been strongly increasing.obesity is considered as significant risk factor for cardiovascular disease, type 2 diabetes, rheumatoid arthritis and neoplasms, hypertension.obesity is also associated with the development of respiratory diseases such as a sleep apnea and hypoventilation syndrome.obesity directly affects respiratory mechanisms at rest and during exercise.obese individuals usually shows change in certain lung volumes, respiratory compliance and ventilator behavior.dyspnoea is the limiting symptom usually experienced by these individuals.
Obesity is a chronic disease characterized by the excessive accumulation of body fat that is harmful to the individuals. Usually body fat above 25% in men and body fat above 30% in women is considered to the obese.Therefore on the basis of this definition, obesity should be determined by measuring body fat. Unfortunately,measures of body composition are not universally and readily available in all clinical setting and therefore most data on the effects of obesity on health rely on the relationship of weight to height such as the BMI, which generally useful for describe different magnitudes of obesity.
Overweight or obesity can cause dangerous health problem and impair quality of life. Due to change in life style and lack of physical activity the problem of obesity is increasing by fast rate in 21st century. It causes disturbances in the respiratory functions. The most consistently reported effect of obesity on lung function is a reduction in the function residual capacity.There effect reflects a shift in balance of inflationary and deflationary pressures on the lung due to the mass load of adipose tissue around the ribcage and abdomen and in the visceral cavity.There is exponential relationship between BMI and functional residual capacity(FRC) with a reduction in FRC detectable even in overweight individuals.
In obesity the reduction in FRC may become so marked that the FRC approach residual volumes. The reasons for the reduction in total lung capacity (TLC) are not known but it is probably due to mechanical effect of adipose tissue, since TLC is increased by weight loss in both mild and morbidly obese subjects.
Deposition of fat in sub pleural space might directly reduce lung volume by reducing the volume of the chest cavity, although there is no direct evidence of any association between subpleural fat either body fat or lung volumes. Respiratory dysfunction in obese individuals may occur because of alternation of the relationship between the lungs, chest wall and diaphragm. There by causing respiratory mechanical damage and abnormalities in gas exchanges.
The respiratory muscles in obese individual have been characterized as insufficient and their endurance has also been found to be lower. This inefficiency results from reduced chest wall complaints smaller pulmonary volumes, greater metabolic demand on the respiratory musculature and increases work required for breathing. Respiratory muscle strength is divided into 2 types. Inspiratory muscle strength: maximal inspiratory pressure is most widely used measure of respiratory muscle strength in patients with suspected respiratory muscle weakness. The measured pressure is a composite of the pressure generated by the inspiratory muscles and the elastic recoil pressure of the lungs and chest wall.
Expiratory muscle strength: respiratory function improvement will be shown by increased maximum expiratory pressure and improved cough airflow measures. Respiratory muscle strength is responsible for respiratory mechanism. Expansion during inspiration and recoiling during expiration is totally depends on the respiratory muscle strength. The respiratory muscle strength was measured as maximum expiratory pressure from forced vital capacity and maximum inspiratory pressure from residual volume which are the pressure values produced during forced expiration and deep inspiration respectively. Respiratory muscles generate the pressure values produced drive ventilation.
World health organization in 2005 have estimated total numbers of overweight were 937 million and obese adults were 396 million. By 2030, the number of overweight predicted to be 1.35 billion and obese adults 573 million individuals without adjusting for secular trends. If recent secular trends continue, the numbers were projected to total 2.16 billion overweight and 1.12 billion obese individuals [1-8].
Aims of Study
The aim of study was to assess the impact of obesity on lung parameters for obese, overweight, normal female subjects
Objectives
- To find out the maximum inspiratory pressure and maximum expiratory pressure
- To find out the tidal volume and forced vital capacity.
- To find out the inspiratory and expiratory muscle strength.
Need for the Study
- The life style of society is changing from agricultural life to industrial life, where sedentary activities are increased.
- Eating habits, frequency and fat content of food has increased. It increases the prevalence of obesity.
- Surprisingly obesity is often neglected although it is associated with serious health consequences like type 2 diabetes, heart and vascular diseases, cancer and respiratory dysfunction etc. Complications of obesity on respiratory functions were studied by many researches.
- Few studies are conducted in India on obesity and respiratory muscle strength and also obtained controversial finding.
- So we are in the need to find out the relation between the obesity and respiratory muscle strength in adults.
The alterations in respiratory muscle strength by obesity were evidenced in the parameters maximum expiratory pressure and maximum inspiratory pressure suggested that obesity affects to the respiratory mechanics. Overload of fat on respiratory muscle and chest region require more pressure during respiration. It may be prevented if active measures are taken to reduce weight by change in life style and food habits.-
Children with obesity demonstrated a reduction in lung volume and capacity. Thus, anthropometric and body composition characteristics may be predictive factors for altered lung function.
Distribution also did not influence respiratory muscle strength.
Obesity places a significant on the respiratory system affecting lung volumes, respiratory muscle function, work of breathing and ventilator control. Most morbidity obese individual maintain eucapia. A group of morbidly obese individuals will develop chronic daytime hypercapnia. Described as the obesity hypoventilation syndrome.
Materials and Methodology
Materials Used
Spirometer
Study Design
Observational survey study
Study Setting
The study was conducted in cherraan’s institute of health science, Coimbatore
Study Duration
The study was conducted for a period of 6 months.
Population And Sampling
60 subjects were selected by convenient sampling method.
Inclusion Criteria
Clinically healthy, wiiling, females, paramedical students
Age between groups 18- 22.
BMI greater than >30 were classified under obese, 25 -29.9 were classified over weight,then normal weight is 18.5- 24.9
Subjective who were specially their respective age were specially selected
Exclusion Criteria
- Medical illness
- Anxious
- Apprehensive and non cooperative students
- Hereditary aspect of disease
- Respiratory infections
- Respiratory disease
- Hypertensive
- Musculoskeletal deformity
Procedure
The subjects were selected with age group between 18-22 (obesity, over weight, normal weight) from cherraan’s institute of health science for this study. The number of subject involved the study is 60. Based on BMI of individuals the subjects are divided into 3 groups.Each group with 20 subjects.
BMI greater than >30 were classified under obese, 25 -29.9 were classified over weight, then normal weight is 18.5- 24.9 Maximum inspiratory pressure, maximum expiratory pressure, forced vital capacity and tidal volume are measured by using spirometer. By using spirometry we measure the 4 values (maximum inspiratory pressure, maximum expiratory pressure, tidal volume forced vital capacity)
Maximum inspiratory pressure :
To measure the maximum inspiratory pressure. subjects should be in sitting position. The strength of the muscle is measured by breath in, and asked to breathe out as long as subject can and then suck hard on a mouthpiece for at least one second. In this method the maximum inspiratory pressure can be calculated.
Maximum expiratory pressure:
To measure the maximum expiratory pressure. subject should be in sitting position. the strength of the muscle is measured by breath out and asked to breath in as deep as the subjects can and followed by blow out as hard as subject can into a mouth piece. In this method the maximum expiratory pressure can be calculated.
Forced Vital Capacity
Forced expiratory volume is the volume of air which can be expired forcefully in a given unit of time ( after a deep inspiration ). It is also called timed vital capacity or forced expiratory vital capacity (FVC). It is dynamic lung volume. FEV1 = Volume of air expired forcefully in 1 second FEV2 =volume of air expired forcefully in 2 second FEV 3 = volume of air expired forcefully in 3 second FVC = FEV1 +FEV 2+ FEV 3
Tidal Volume
Tidal volume is the volume of air breathed in and out of lungs in a single normal quiet respiration. Tidal volume signifies the normal depth of breathing.
Spirometry
It is one of the primary pulmonary function tests used to check the health of the lungs and respiratory passage ways. When a spirometry test is performed the subjects breathes through a mechanical or electronic airflow sensor called a spirometer.
Data Analysis
The collected data was tabulated and analyzed by statistical method.
Results
The most common and consistent pulmonary function tests abnormality seen in obese individuals is a reduction in maximum inspiratory pressure, maximum expiratory pressure, forced vital capacity and tidal volume. Increased effort is needed to overcome respiratory system elasticity. Thus, obese individuals need to do more respiratory work to maintain appropriate levels of ventilation.
Subjects were screened for obesity having BMI more than 30 kg/m2 included in obese group. Subjects having BMI 25 to 29.9 kg/m2 are included in over weight group. Subjects having BMI 18.5to 24.9 are included in normal group.data collected from 3 group further statistical analysis was done of collected data of three groups.
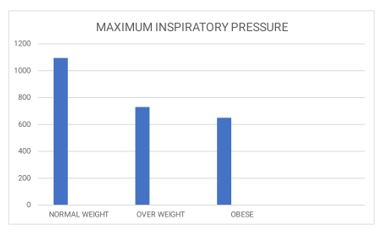
In the respiratory muscle strength parameters, mean maximum inspiratory pressure, in obese group 650 ml, in over weight group 730 ml, normal weight group 1095ml.
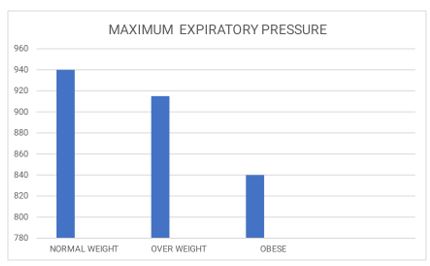
In maximum expiratory pressure, the mean valve of obese group 840 ml, in over weight group 915 ml, in normal group 940 ml.
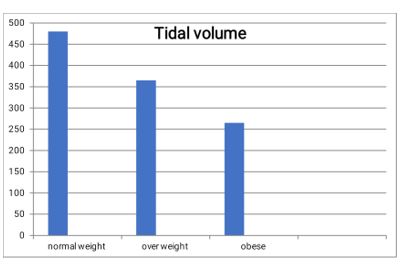
In tidal volume the mean valve of obese group 265ml, in over weight group 365 ml, normal weight group 480 ml
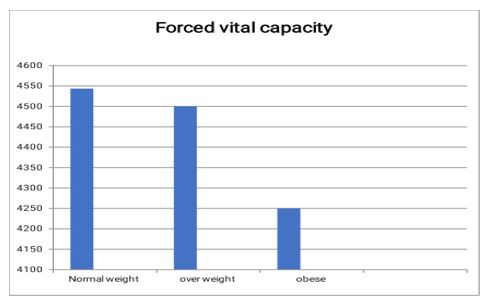
In forced vital capacity the mean valve of obese group 4250 ml, in over weight group 4500ml, in normal weight group 4543.5 ml.
Maximum inspiratory pressure -normal weight >over weight >obese. Maximum expiratory pressure -normal weight >over weight >obese. Tidal volume -normal weight >over weight >obese.
Forced vital capacity -normal weight >over weight > obese.
Hence we concluded that maximum inspiratory pressure, maximum expiratory pressure, tidal volume, forced vital capacity are increased in normal adult female when compared to the over weight and obese adult females.
Discussion
George Jung, et al.l reported decrement in the MEP and MIP due to increment in BMI. According to their studies decreased respiratory muscle functions might be due to increased elastic load by fat deposition around the chest region.
Srila Ghosh Chowdhury,the adiposity in relation with BMI or hip circumference and waist circumference or waist hip ratio leads to decrement in respiratory parameters. In our result by Pearson analysis weak positive relation between WC, HC, and W/H with MEP was existing. And moderate to intermediate positive relation of MIP with these anthropometric parameters.
Noppawan C, et al, it provides information about the pulmonary function and respiratory muscle strength in Thai obese children. FVC, FEV1 & VC was more in obese group than non obese group. Obese group was having more airway obstruction. Moreover RMS and physical activity in both groups were same.Magnani KL, et al. in their study shown no change in maximum expiratory pressure & maximum inspiratory pressure with BMI. In the obese population studied, the excess weight did not result in impairment of respiratory muscle strength.
Measurement of maximum inspiratory and expiratory pressures would help in identifying which obese individuals have respiratory impairment.
Barbalho –moulin, et al, respiratory muscle dysfunction is the main cause of pulmonary complications after abdominal surgery and because of this respiratory training is recommended. This study is informative for physical therapists and health professionals regarding the difficulties in using predictive respiratory muscle strength formulas that do not take body mass into account.Young, et al. (2003) suggested that the reduction of the ERV can lead to the increase of areas of atelectasis, harming the ventilation/perfusion mismatch and leading to arterial hypoxemia in those individuals. Some authors have suggested that obesity may promote air trapping, which impairs adequate pulmonary ventilation through the reduction of pulmonary volumes.
Teixeira, et al. 22 (2007) showed an increase in the residual volume (RV) associated with the reduction in the ERV in obese subjects who had dyspnea complaints. The authors suggested that the reduction in the ERV can be attributed to the obstruction of small airways and a consequent reduction in gas exchange.
Ladosky, Botelho, and Albuquerque12 (2001), comparing a group of obese and non-obese patients, also suggested that the reduction of the ERV may be a consequence of air trapping caused by obesity and leading to a reduction in the MVV.
In our study altered lung function in individual with obesity is due to the excessive deposition of fat in thoracic abdominal region, which alters the mobility of diaphragm muscles thoracic expansion as well as lung compliance and strength, leading to a rapid low amplitude breathing pattern with an increase in respiratory work and a reduction in maximum ventilator y capacity.
Shift in the balance of inflationary and deflationary pressure on the lung due to the mass load of adipose tissue around the rib cage and abdomen. Abdominal and thoracic fat are likely to have direct effects on the downward movements of the diaphragm and chest wall properties, while fat on the hips and thighs would be unlikely to have any direct mechanical effect on the lungs.
Reductions in lung compliance may be the results of increased pulmonary blood volume, closure of dependent airways, resulting in small areas atelectasis or increased in the obese indicating the airway caliber is reduced throughout the tidal breathing cycle. That peripheral airway obstruction may be increased in the obese.
Due to mechanical effect of the adipose tissue maximum inspiratory pressure, maximum expiratory pressure, tidal volume and forced vital capacity are decreased in obese compared to the over weight and normal weight adult females.
Hence we conclude, that the normal adult female has more effective respiratory muscle strength when compare to the over weight and obese adult females [9-15].
Conclusion
From the data presentation and analysis it is evident that
In this study we concluded that the adult female with obesity demonstrated a reduction of lung volumes and capacity. Anthropometric and body composition characteristics may be predictive factors for altered lung function.
And here by we conclude that respiratory muscle strength is increased in adult female with normal BMI.
- David Haslem, Naveed Sattar, Mike Lean (2006) ABC of obesity. Obesity – time to weak up. BMJ 333: 640-42.
- WHO (2007) Global database of BMI classification.
- Appropriate body-mass index for Asian population and its implications for policy and intervention strategies, Lancet 363: 902
- T Kelly, W Yang, C-S Chen, K Reynolds, J He (2008) Global burden of obesity in 2005 and its projection to 2030. Ij of Obe 32: 1431-7.
- SDH Malnick, H Knobler (2006) The medical complications of obesity.Q J Med 99: 565-79.
- T Troosters, R Gosselink, M Decramer (2005) Respiratory muscle assessment. Eur Respir Mon 31: 57–71.
- Pedro Caruso, André Luis Pereira de Albuquerque, Pauliane Vieira Santana, Leticia Zumpano Cardenas, Jeferson George Ferreira, Elena Prina, et. al. Diagnostic methods to assess inspiratory and expiratory muscle strength. J Bras Pneumol 41: 110-23
- EM Pazzinoto F, FS Peixoto S, C Picono M, I Rasera J, M Barbalho M (2012) Behaviour of respiratory muscle strength in morbidly obese women by using different predictive equations. Rev Bras Fisioter, São Carlos 16: 479-86.
- Wilaiwan Khrisanapant, Jaruwan Plaengde, Watchara Boonsawat, Orapin Pasurivong (2011) Obesity and Respiratory Muscle Strength in Thai women, JPBS 24: 1-11.
- Thais Ribeiro Costa, Tiago Pessoa Lima, Patrícia Lúcia Gontijo, Harley Alves de Carvalho, Flávia Perassa de Faria Cardoso,, et al.. (2010) Correlation of respiratory muscle strength with anthropometric variables of normal-weight and obese women. Rev Assoc Med Bras 56: 403-8.
- Paltiel Weiner, Joseph Waizman, Margalit Weiner, Marinella Rabner, Rasmi Magadle,, et al.. (1998) Influence of excessive weight loss after gastroplasty for morbid obesity on respiratory muscle performance, Thorax 53: 39-42.
- George Jung da Rosa, Camila Isbabel S Schivinski (2014) Assessment of respiratory muscle strength in children according to the classification of body mass index. Rev Paul Pediatr 32: 250-5.
- Srila Ghosh Chowdhury, Oona Mandal, Arunima Datta, Debjani Chakraborti (2015) Effect of Central Adiposity on Lung Function Tests in Young Adults, IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) 14: 24-28.
- Noppawan C, Suwannnee J, Pipop J Saipin P (2007) Pulmonary functions & respiratory muscle strength in Thai obese children.; Sairaj Med J 59: 125-30.
- Magnani KL, Cataneo AJ (2007) Respiratory muscle strength in obese individuals and infl uence of upper-body fat distribution. Sao Paulo Med J 125: 215.
Figure 1
Figure:
Graph 1
Graph 2
Graph 3
Graph 4
Tables at a glance
Figures at a glance