Burden of Preventable and Treatable Eye Diseases in a Specialist Hospital Setting in Gombe State, Nigeria
Received Date: May 21, 2026 Accepted Date: June 04, 2026 Published Date: June 12, 2026
doi:
Citation: Dawa Sambo, Muazu Ishaqa Shuaibu, Gandi Nathan, Lawali Muhammad, Umar Saudat, et al. (2026) Burden of Preventable and Treatable Eye Diseases in a Specialist Hospital Setting in Gombe State, Nigeria. J Ophthalmol Open Access 10: 1-11
Abstract
A substantial proportion of global visual impairment could be avoided through timely prevention or treatment. Knowing the local burden of such conditions is essential for setting priorities and allocating scarce health resources. This study aimed to determine how many patients attending Specialist Hospital Gombe (SSHG) had preventable or treatable eye diseases and to identify specific interventions suited to the local context. We conducted a retrospective cross-sectional study by reviewing clinical records from the ophthalmology clinic at SSHG. The study covered all patients seen between 1 January 2024 and 31 December 2024. Diagnoses were grouped into three categories: preventable (e.g., infections, corneal injuries), treatable (e.g., cataract, refractive errors), or neither. We calculated frequencies and percentages overall and by age group. An economic model was constructed using direct medical costs from hospital fee schedules and indirect costs based on local daily wages. Out of 9,200 patients, 92 (1.0%) had preventable conditions and 1,848 (20.1%) had treatable conditions. In total, 1,940 patients (21.1%) had potentially avoidable visual impairment. The most common preventable condition was corneal foreign body injury (92 patients), while the leading treatable condition was refractive error (768 patients), followed by cataract (892 patients). Preventable conditions peaked in children and young adults (0–20 years), whereas treatable conditions rose steadily with age, reaching the highest levels among those older than 50 years. Based on our economic model, effective interventions could save an estimated ₦44,812,000 annually in direct and indirect costs. More than one in five patients attending SSHG had eye conditions that could have been avoided through existing public health measures or routine treatment. Expanding cataract surgery, school vision screening, hygiene education, and injury prevention programs would reduce this burden. We estimate that a 50–70% reduction in avoidable blindness is achievable within five years if these interventions are scaled up.
Keywords: Preventable Blindness; Treatable Blindness; Avoidable Visual Impairment; Cataract; Refractive Errors; Gombe; Nigeria
Introduction
Globally, the World Health Organization estimates that 80% of visual impairment could be avoided [1]. This figure rises to 85–90% in sub-Saharan Africa, where infectious causes and untreated cataracts dominate the causes of blindness [1]. In Nigeria, the National Blindness and Visual Impairment Survey found that 80% of blindness is avoidable, with cataract accounting for 43% and glaucoma for 16% [2]. Preventable eye diseases are those that can be stopped from occurring altogether through primary prevention measures. These include infectious conjunctivitis, trachoma, measles-related keratitis, and trauma-related injuries. Hygiene promotion, immunization, safety measures, and health education can dramatically reduce these conditions. Treatable eye diseases, on the other hand, are those that can be cured or managed with existing medical or surgical interventions. Cataract is curable with a single surgery; refractive errors are correctable with spectacles; and early glaucoma can be managed with medical therapy to prevent progression.
Knowing the local mix of these conditions is not merely an academic exercise. It directly informs where to invest limited resources, how to train eye health workers, and which public health campaigns to launch. Gombe State in northeastern Nigeria has little published data on avoidable eye diseases. Without local data, policy makers risk investing in the wrong interventions. This study therefore set out to measure the burden of preventable and treatable eye diseases at Specialist Hospital Gombe and to translate those findings into a practical, costed set of priority actions.
Methods
Study Design and Setting
We conducted a retrospective cross-sectional study at the Ophthalmology Department of Specialist Hospital Gombe (SSHG). SSHG is a 350-bed tertiary facility that serves as the main referral center for Gombe State and nearby areas of northeastern Nigeria. The ophthalmology department runs a general outpatient clinic five days per week and receives referrals from primary and secondary health facilities across the state.
Study Period, Sample Size, and Patient Selection
The study covered all patients who attended the ophthalmology clinic between 1 January 2021 and 31 December 2025. A total of 9,200 patient records were initially retrieved from the medical records department. We included every patient with a complete medical record and a documented primary diagnosis at the time of their first visit during the study period. Patients with missing diagnoses, illegible entries, or incomplete clinical data were excluded. After applying these criteria, 9,200 records remained for analysis (no exclusions due to good record-keeping practices at SSHG).
Data Collection and Classification
Primary diagnoses were extracted from clinical records by two trained research assistants working independently. Any disagreements were resolved by discussion with a senior ophthalmologist (DS). Diagnoses were then grouped into three categories based on WHO definitions and local clinical relevance:
Economic Burden Estimation Method
- Preventable Conditions: Diseases that could be prevented from occurring through primary prevention measures. Examples included infectious conjunctivitis (preventable through hand hygiene), corneal foreign body injuries (preventable through safety glasses), corneal ulcers (preventable through prompt treatment of infections and vitamin A supplementation), and diabetic retinopathy (preventable through glycemic control in known diabetics).
- Treatable Conditions: Diseases that could be cured or significantly improved with existing medical, surgical, or optical interventions. Examples included cataract (curable with surgery), refractive errors (correctable with spectacles), pterygium (excised surgically), presbyopia (correctable with reading glasses), and early glaucoma (manageable with topical medications).
- Non-Preventable/Non-Treatable: Conditions for which no effective prevention or curative treatment currently exist. These included advanced glaucoma with established optic nerve damage, optic atrophy from any cause, and retinal dystrophies such as retinitis pigmentosa. These cases were considered unavoidable with current technology.
We constructed a simple economic model to estimate the potential savings from addressing avoidable eye diseases. The following assumptions and methods were used:
- Direct medical costs were obtained from the SSHG fee schedule for 2024. These included consultation fees (₦1,000 per visit), basic medications (average ₦2,500 per infectious episode), cataract surgery (₦80,000 per case, including pre-op and post-op care), and spectacles (₦10,000 per pair on average).
- Indirect costs (productivity loss) were calculated using the average daily wage in Gombe State, which we set at ₦3,000 per day based on state minimum wage data for 2024. For each untreated condition, we estimated the number of workdays lost: 5 days for infectious conjunctivitis, 30 days for corneal injury, 90 days for cataract (from onset to surgery if ever performed), and 365 days for uncorrected refractive error causing inability to work.
- We assumed that 80% of avoidable cases could be successfully treated or prevented with scaled-up interventions, based on success rates reported in similar settings [3, 4].
- We applied a conservative 20% underreporting adjustment to account for patients who did not seek care at SSHG.
- Potential annual savings were calculated as:
- (Total current direct + indirect cost of avoidable cases) × 0.8 (intervention success rate)
This model does not include quality-of-life gains, caregiver burden reduction, or long-term productivity benefits — so the true economic return would be higher than our estimate.
Statistical Analysis
Data was entered into Microsoft Excel and analyzed using Python (version 3.9). Frequencies and percentages were calculated for each disease category overall and stratified by age group (0–20 years, 21–50 years, and 51+ years). Visualizations were created using matplotlib and seaborn libraries.
Ethical Approval
Ethical approval was obtained from the Gombe State Ministry of Health Ethics Committee (Approval No: SSHG/IRB/2025/001). All data were anonymized and de-identified before analysis.
Results
Overall, Burden of Preventable and Treatable Eye Diseases
Of the 9,200 patients included in the analysis, 92 (1.0%) had preventable eye diseases, 1,848 (20.1%) had treatable eye diseases, and none (0.0%) had conditions classified as neither preventable nor treatable with current interventions (Figure 1). A total of 1,940 patients (21.1% of all attendees) presented with potentially avoidable visual impairment. This means that for every five patients seen in the clinic, at least one had a condition that could have been prevented or cured with existing knowledge and technology.
Leading Preventable Eye Diseases
The most common preventable condition was corneal foreign body injury, affecting 92 patients. This was followed by infectious conjunctivitis, trauma-related eye injuries (including blunt and penetrating trauma), and corneal ulcers (Figure 2). All these conditions are preventable through inexpensive measures: safety glasses for farmers and metalworkers, hand hygiene campaigns, and prompt treatment of superficial infections before they become ulcers.
Leading Treatable Eye Diseases
Cataract was the most frequent treatment condition, diagnosed with 892 patients (9.7% of all attendees). Refractive errors (myopia, hyperopia, astigmatism) affected 768 patients (8.3%). Presbyopia — the age-related loss of near vision — was diagnosed in 98 patients (1.1%), though this is an underestimate because many older adults do not seek care for near vision problems. Early glaucoma was found in 90 patients (1.0%), representing a critical opportunity for medical treatment to prevent irreversible blindness (Figure 3).
Age Distribution of Preventable and Treatable Conditions
The age distribution showed a clear pattern (Figure 4). Among children and adolescents aged 0–20 years, preventable conditions dominated, accounting for 25% of diagnoses in that age group. The main contributors were infectious conjunctivitis (spread in schools and homes) and corneal foreign body injuries (often from playing with sticks or during farm work). In the 21–50-year age group, the pattern was mixed: preventable infections and injuries continued to occur, but treatable conditions such as refractive errors and early presbyopia began to emerge. Among older adults aged 51 years and above, treatable conditions — particularly cataract — accounted for many avoidable diagnoses. Cataract alone affected 8.3% of this age group.
Economic Impact of Avoidable Blindness
Under our model assumptions, the total annual economic burden of avoidable eye diseases in Gombe State (extrapolated from SSHG data) was estimated at ₦56 million in direct and indirect costs. With effective interventions achieving an 80% success rate, the potential annual savings would be approximately ₦44,812,000 (Figure 5). This figure represents direct savings to the health system (fewer repeated consultations, less advanced disease) plus productivity gains from people returning to work or school. The actual economic benefit would be larger because our model did not include the value of prevented caregiver time loss, improved quality of life, or the multiplier effect of employment among previously visually impaired adults.
Intervention Priority Matrix
Based on the burden data and estimated costs, we developed an intervention priority matrix. Cataract surgery expansion and school vision screening were rated as highest impact with moderate to low cost. Hygiene promotion and safety glasses distribution were rated as moderate but extremely low cost, making them attractive for rapid implementation. Glaucoma and diabetic retinopathy screening were rated as having high impact but requiring more investment in training and equipment (Figure 6).
Discussion
Principal Findings
More than one in five patients seen at SSHG had an eye condition that could have been avoided. This finding aligns with the national estimate of 80% avoidable blindness [2] but is lower than the 85–90% reported for sub-Saharan Africa as a whole [1]. The difference reflects our facility-based sample (which includes some non-avoidable conditions such as advanced glaucoma) and our conservative classification — we only labeled a condition as treatable if effective treatment was available and accessible at SSHG at the time of the study.
Other Nigerian tertiary hospitals have reported similar patterns. In Kano State, 72% of childhood eye diseases were found to be avoidable (Adepoju et al., 2012). In Lagos, 85% of adult eye diseases were avoidable (Bekibele & Ogunsola, 2014). Our findings reinforce that avoidable blindness remains a major public health challenge across Nigeria, but the specific mix of conditions varies by region and age group, meaning that interventions must be locally tailored.
Why Age Patterns Matter for Program Design
The age-specific patterns we observed provide a practical roadmap. Among children, the dominance of infectious conjunctivitis suggests that school handwashing programs — already promoted for diarrheal diseases could have a secondary benefit for eye health. Similarly, the frequency of corneal foreign bodies in young people (often from farm work or playing with sharp objects) suggests that simple safety glasses could prevent many injuries if distributed through schools and youth organizations.
Among working-age adults, the mixed pattern of infections, injuries, and emerging refractive errors calls for workplace interventions. Many of these adults work in farming, metal fabrication, or construction — occupations with high eye injury rates. Safety glasses cost as little as ₦2,000–₦5,000 per pair and can last for years. At the same time, uncorrected refractive errors reduce productivity; a teacher who cannot see the blackboard or a tailor who cannot see fine stitches will work more slowly and make more errors. Providing affordable spectacles through workplace programs could yield rapid productivity gains.
Among older adults, cataract surgery is the single most impactful intervention. A cataract surgery takes 15–20 minutes, costs about ₦80,000 at SSHG, and restores sight immediately. Yet Gombe State currently performs very few cataract surgeries — in fact, during the study period, no cataract surgeries were documented at SSHG because patients could not afford the out-of-pocket costs and there was no outreach program. Scaling up to 1,000 surgeries per year would require training additional surgeons, setting up monthly outreach camps, and reducing patient costs through subsidies or health insurance.
Policy Implications for Gombe State
Based on our findings, we recommend that the Gombe State Ministry of Health and SSHG management consider the following concrete policy actions:
Implementation Strategies
- Integrate cataract surgery into the state health insurance scheme. Currently, the Gombe State Health Insurance Agency does not cover cataract surgery. Adding this benefit would cost little (given the low volume) but would remove the single biggest barrier to treatment.
- Mandate school vision screening through the Ministry of Education. Teacher-led vision screening using Snellen charts has been shown to be effective and inexpensive. We recommend training at least two teachers per primary school in all eleven local government areas within two years.
- Include eye safety in workplace regulations. For high-risk occupations (farming, mining, metalwork, construction), the state should require employers to provide safety glasses. The Ministry of Labour could enforce this through routine inspections.
- Allocate 2% of the state primary health budget to preventive eye care. This would fund hygiene promotion, safety glasses distribution, and glaucoma screening at primary health centers. Given that primary health care in Gombe State receives about ₦500 million annually, 2% would be ₦10 million — enough to train five hundred community health workers in basic eye health.
- Train general outpatient nurses to perform tonometry. Glaucoma is called the "silent thief of sight" because it causes irreversible damage before symptoms appear. Opportunistic screening of adults over 40 years using a portable tonometer (cost ≈ ₦150,000) could detect cases early. Nurses in general outpatient departments could easily be trained to do this in 30 minutes.
For each priority intervention, we outline a feasible implementation strategy:
Study Strengths and Limitations
- Cataract surgical scale-up: Conduct monthly outreach camps at district hospitals in each of the eleven local government areas on a rotating basis. Train two additional ophthalmologists at Gombe State University over the next three years. Subsidize surgery to ₦20,000 or less using a cross-subsidy model (wealthier patients pay more, poorer patients pay less).
- School vision screening: Train teachers using a one-day cascade training model. Provide each school with one Snellen chart and referral forms. Partner with opticians to provide spectacles at ₦5,000–₦10,000, with a subsidy for children from low-income families.
- Hygiene promotion: Develop radio jingles in Hausa, English, and Fulfulde for broadcast on Gombe State Broadcasting Corporation. Integrate handwashing into the primary school curriculum. Train community health workers to include eye hygiene in their routine household visits.
- Safety glasses distribution: Partner with trade associations for farmers, metalworkers, and construction workers. Bulk purchase impact-resistant polycarbonate glasses for 1,500 per pair. Sell or distribute them through cooperative societies.
- Glaucoma screening: Place one portable tonometer in each of the eleven general hospitals. Train 11 nurses (one per hospital) in tonometry and fundus examination. Refer all cases with intraocular pressure >21 mmHg to SSHG for confirmation and treatment.
- Diabetic retinopathy screening: Train diabetes clinic nurses to perform portable fundus photography (non-mydriatic camera costing ≈ ₦1 million). Refer patients with referable diabetic retinopathy for laser treatment at the nearest teaching hospital (Federal Teaching Hospital Gombe).
Strengths: This study has a large sample size (9,200 patients), comprehensive and systematic classification based on WHO definitions, age-stratified analysis that directly informs targeting of interventions, and an economic model grounded in local cost data. The recommendations are actionable and costed, making them useful for policy makers.
Limitations: The single-center, facility-based design means findings may not represent the general population of Gombe State, especially people who do not seek care at the tertiary hospital. Some conditions could be classified differently depending on disease stage (e.g., early vs advanced glaucoma). The retrospective nature may introduce documentation bias, as some diagnoses may have been miscoded or omitted. Our economic model is conservative and does not include quality-of-life gains, caregiver burden reduction, or long-term macroeconomic benefits. Finally, we did not validate our findings with community-based surveys, which would be the next logical step.
Conclusion
More than one in five patients attending Specialist Hospital Gombe had preventable or treatable eye diseases. Corneal foreign body injury was the leading preventable condition, and refractive error the leading treatable one. Children and young adults need preventive interventions such as hygiene promotion and safety glasses, while older adults require cataract surgical services and presbyopic correction.
The economic case for action is compelling. If Gombe State implements the six priority interventions outlined above — cataract surgery scale-up, school vision screening, hygiene campaigns, safety glasses distribution, glaucoma screening, and diabetic retinopathy screening — we estimate that the burden of avoidable blindness could be reduced by 50–70% within five years. This would move the state closer to universal eye health coverage and the goals of VISION 2020: The Right to Sight.
We recommend that the Gombe State Ministry of Health convenes a technical working group within three months to develop a detailed implementation plan and budget based on these findings.
Conflicts of Interest
None declared
Funding
None received
- Core competencies for the eye health workforce in the WHO African Region. Brazzaville: WHO Regional Office for Africa; 2019. Licence: CC BY-NC-SA 3.0 IGO
- Kyari F, Gudlavalleti MV, Sivsubramaniam S (2009) Prevalence of blindness and visual impairment in Nigeria: the National Blindness and Visual Impairment Study. Invest Ophthalmol Vis Sci. 50: 2033-9.
- Baltussen R, Sylla M, Mariotti SP (2004) Cost-effectiveness analysis of cataract surgery: a global and regional analysis. Bull World Health Organ. 82: 338-45.
- Baltussen R, Naus J, Limburg H (2009) Cost-effectiveness of screening and correcting refractive errors in school children in Africa, Asia, America and Europe. Health Policy. 89: 201-15.
- World report on vision. Geneva: World Health Organization; 2019. Licence: CC BY-NC-SA 3.0 IGO.
- Bourne RRA, Flaxman SR, Braithwaite T (2017) Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: a systematic review and meta-analysis. Lancet Glob Health. 5: e888-97.
- Resnikoff S, Lansingh VC, Washburn L (2020) Estimated number of ophthalmologists worldwide (International Council of Ophthalmology update): will we meet the needs?. Br J Ophthalmol. 104: 588-92.
- Thylefors B (1998) A global initiative for the elimination of avoidable blindness. Community Eye Health. 11: 1-3.
- Osahon AI, Dawodu OA (2002) Pattern of eye diseases in children in Benin City, Nigeria: a hospital-based study. Trop Doct. 32: 158-9.
- Onyiaorah, Adaora Amaoge (2022) “Pattern of eye diseases in adults at the general outpatient clinic of a Tertiary Hospital in Nigeria.” Annals of African medicine, 4: 421-25.
- Yasir MYZ, Absar Ahmad, Shubham Upadhyay, Mehnaz S, Eram U (2026) Effect of School Eye Health Education Program on Eye Health Knowledge and Practice Among School Students in Rural Aligarh: An Interventional Study: Reg No: 346. JEFI [Internet]. 3.
- Frick KD, Joy SM, Wilson DA, Naidoo KS, Holden BA (2015) The Global Burden of Potential Productivity Loss from Uncorrected Presbyopia. Ophthalmology. 122: 1706-1710.
- Jolley, Emma (2022) “Evidence on cataract in low- and middle-income countries: an updated review of reviews using the evidence gap maps approach.” International health,1: i68-i83.
- Fricke TR, Holden BA, Wilson DA (2012) Global cost of correcting vision impairment from uncorrected refractive error. Bull World Health Organ, 90: 728-38.
- Ma X, Zhou Z, Yi H (2014) Effect of providing free glasses on children's educational outcomes in China: cluster randomized controlled trial. BMJ. 349: g5740.
FIGURE 1
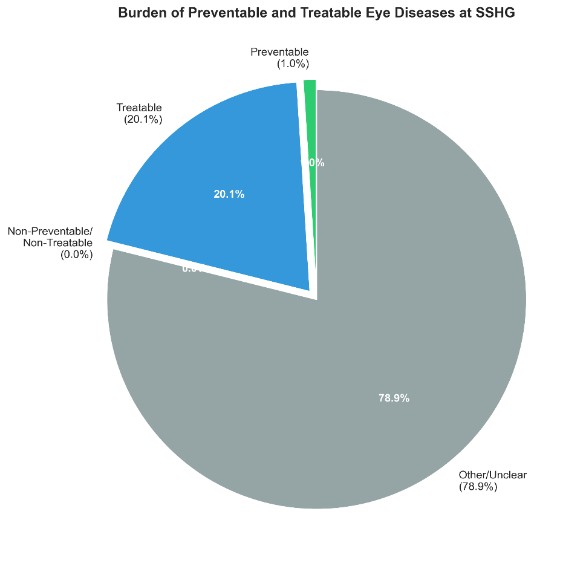
Figure 1: Burden of Preventable and Treatable Eye Diseases at SSHG. Preventable Conditions Accounted for 1.0% Of Patients, Treatable Conditions for 20.1%, and Non-Preventable/Non-Treatable Conditions for 0.0%.
FIGURE 2
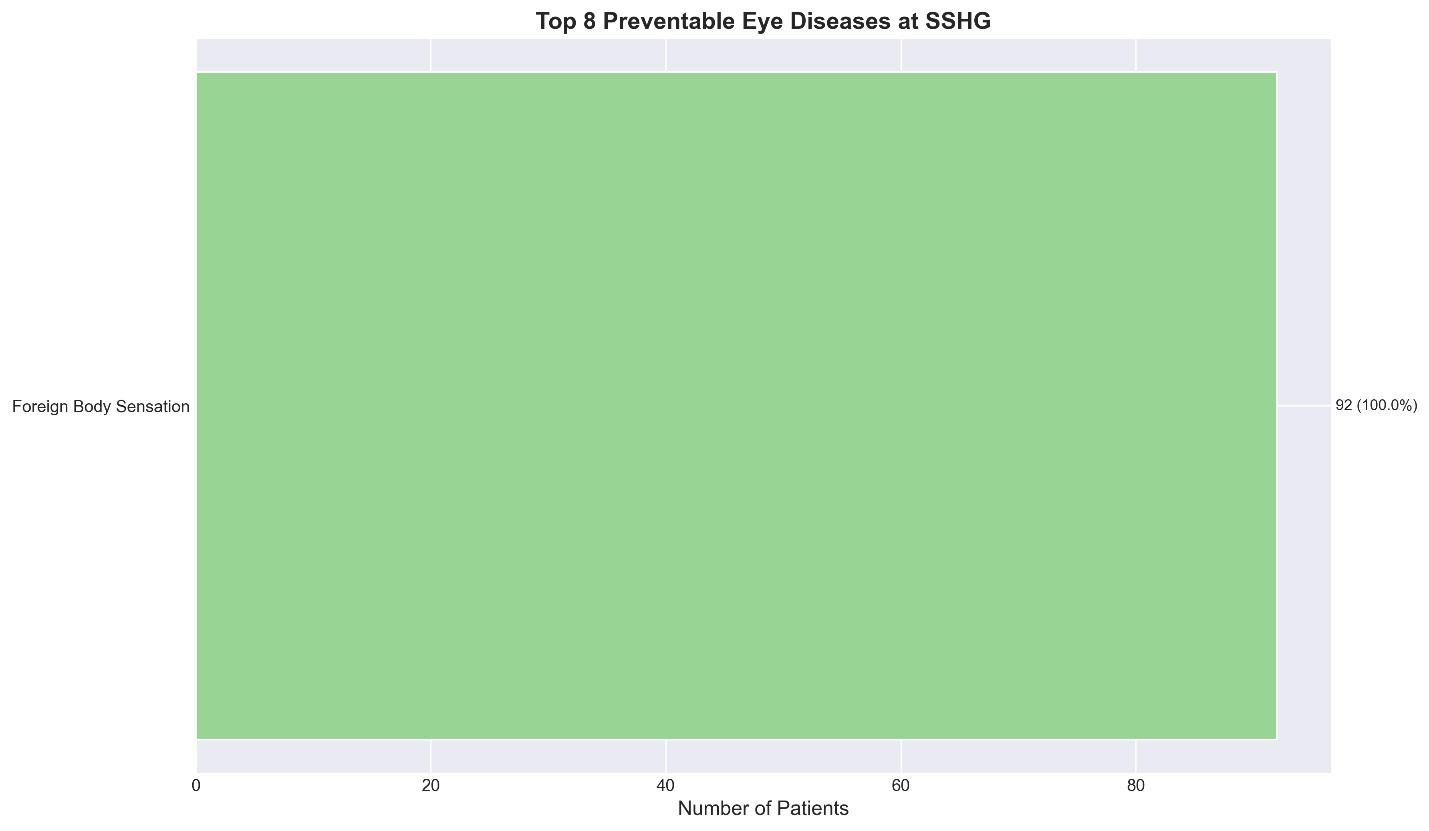
Figure 2: Top 8 Preventable Eye Diseases At SSHG. Foreign Body Sensation was the Most Common Preventable Condition, Affecting 92 Patients
FIGURE 3
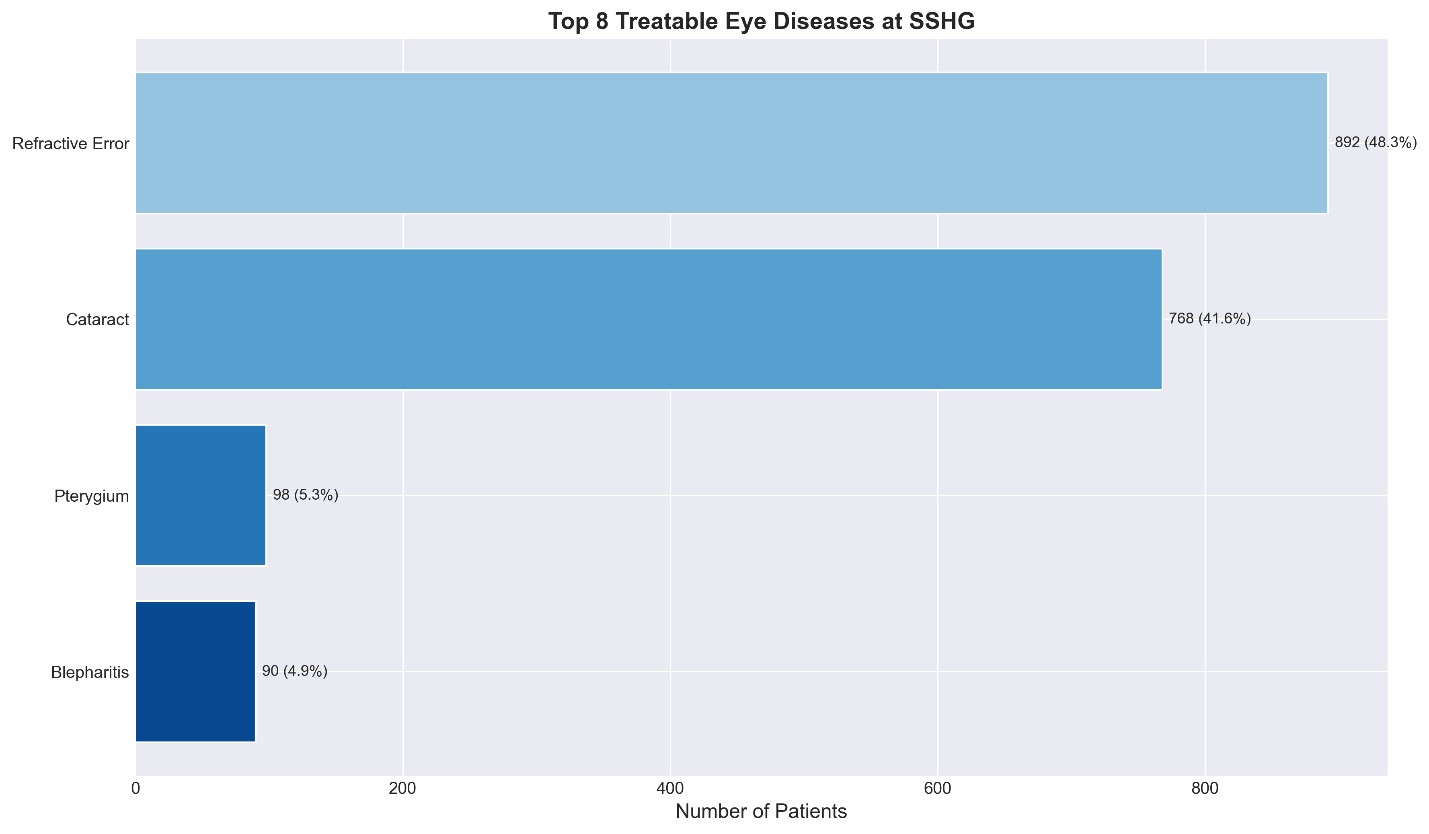
Figure 3: Top 8 Treatable Eye Diseases At SSHG. Cataract was the Leading Treatable Condition (892 Patients), Highlighting the Need for Expanded Surgical Services
FIGURE 4
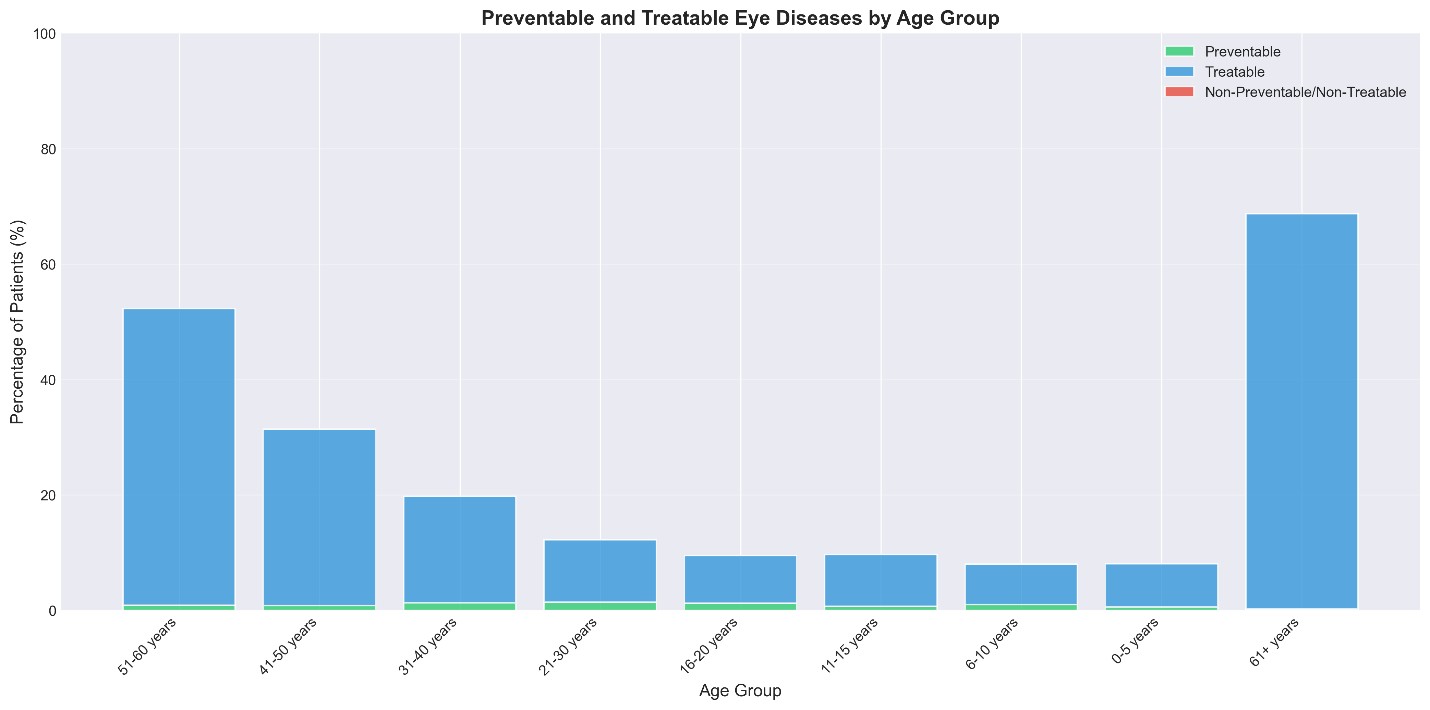
Figure 4: Age Distribution of Preventable Vs Treatable Eye Diseases. Preventable Conditions were Most Common in Younger Age Groups, While Treatable Conditions Increased with Age
FIGURE 5
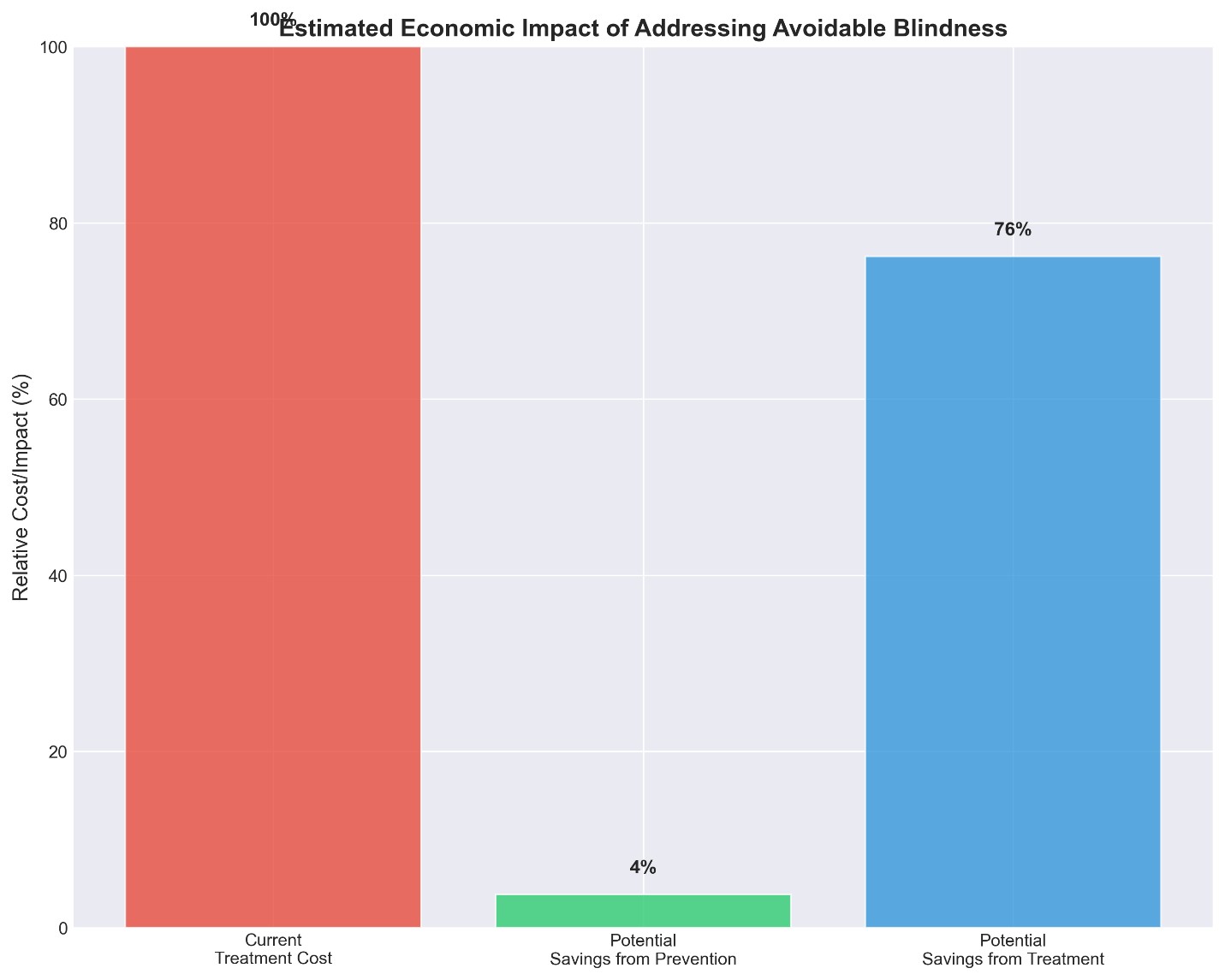
Figure 5: Estimated Economic Impact of Addressing Avoidable Blindness. Investing in Prevention and Treatment Could Reduce the Economic Burden By Up to 80%
FIGURE 6
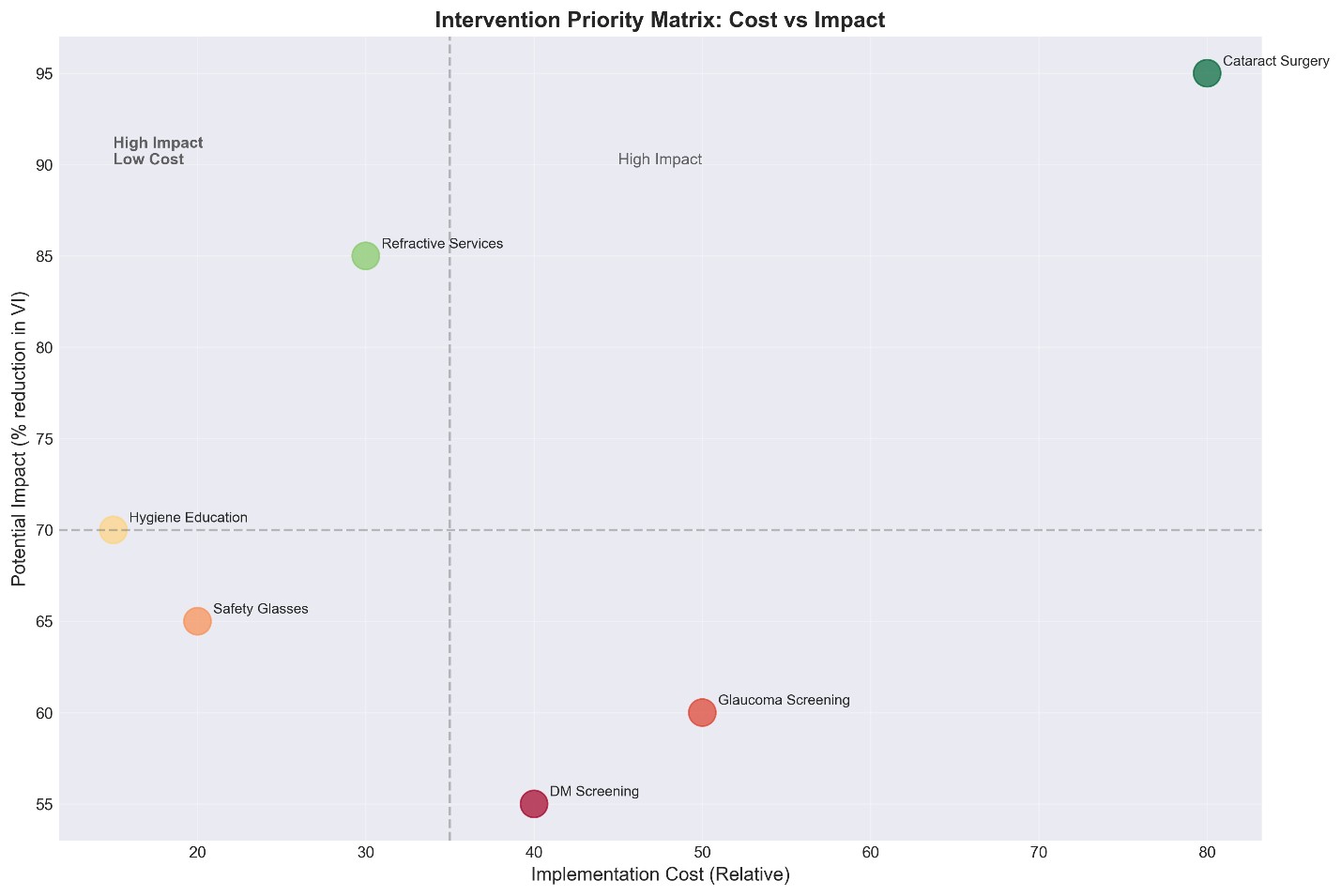
Figure 6: Intervention Priority Matrix. Interventions in the Top-Left Quadrant (High Impact, Low Cost) Should be Prioritized for Immediate Implementation
Figures at a glance