Solitary Cutaneous Atypical Leiomyoma: An Unusual Variant Histologic - A Diagnostic Challenge
Received Date: January 28, 2024 Accepted Date: February 28, 2024 Published Date: March 02, 2024
doi: 10.17303/jpam.2024.1.102
Citation: Elaouni Soukaina (2024) Solitary Cutaneous Atypical Leiomyoma: An Unusual Variant Histologic- A Diagnostic Challenge. J Pathol Allied Med 1: 1-5.
Abstract
Cutaneous atypical leiomyoma is an unusual benign tumor arising from arrector pili muscle that shares histological features with uterine atypical or symplastic leiomyoma defined as “leiomyoma containing giant cells with pleomorphic nuclei and little or no mitotic activity.” Due to the ominous and worrisome microscopic appearance (many large giant cells with hyperchromatic, pleomorphic, malignant looking nuclei), this variant may be misdiagnosed as a sarcoma. We report a case of a solitary cutaneous atypical leiomyoma in a 50-year-old woman without pathological history including uterine leiomyoma or renal disease, who presented with a 4-year history of a painless slow growing lesion on the right upper arm. Histological examination of the excised specimen showed a dermal lesion composed of spindle shaped cells with marked nuclear pleomorphism. No mitotic figures or necrosis were seen. The cells stained strongly positive with desmin and H- caldesmon but negative with S100, pancytokeratin and Ki 67 estimated at 2 percent . The diagnosis was felt to be in keeping with a cutaneous atypical leiomyoma or symplastic leiomyoma. It, therefore presents a diagnostic challenge to the pathologist to accurately diagnose such a tumor while ensuring that a true malignancy is not overlooked. Seven other cases have been reported so far and, in spite of its name and of being a smooth muscle proliferation, no recurrences no metastasis have been reported.
Keywords: Atypical leiomyoma; Cutaneous Form; Pathology
Introduction
Cutaneous leiomyoma is a rare, benign, smooth muscle tumor. It has been divided into different subtypes according to the skin structures from which it can derive, to know: Pilar leiomyoma which can arise from the arrector pili muscle, angioleiomyoma which can arise from the media of blood vessels and genital leiomyoma which can arise from the smooth muscle of the scrotum, labia major or nipples [1]. The cutaneous atypical leiomyoma or symplastic leiomyoma is a rarely reported variant of the pilar leiomyoma, presents usually as multiple tumors and presentation of the lesion as a solitary tumor is less common [2]. Histologically, it shows features similar to the symplastic variant of uterine leiomyoma with cytological atypia, nuclear pleomorphism and minimal mitotic activity. Despite such atypia the uterine symplastic leiomyoma has so far showed a benign course and outcome although studies to confirm prognosis for the cutaneous form are awaited.
Case presentation
A 50-Year-Old woman presented to our hospital for evaluation of a 1,7 x1 cm nodule of her right upper arm present for approximately 04 years with a slight increase in the lesion itself. Her medical and surgical history was not significant including uterine leiomyoma or renal disease and no family history of similar lesion was reported. Physical exam founded only one lesion on the right upper arm, firm brown-pink smooth papule, slightly painful and tender on palpation (Figure 1). A punch biopsy, histologically evocated a spindle cell tumor highly suspected of malignancy. Given these findings, computerized tomography (CT) scans of the chest, abdomen and pelvis were performed to exclude the possibility of visceral malignancy. Consideration was made that the cutaneous lesions could represent metastases from solid organ sarcoma. The scans revealed no evidence of malignancy. Renal function tests and urinalysis were normal. Therefore, the area was subsequently treated with conservative excision. Microscopically, it is a unencapsulated, circumscribed dermal tumor completely excised, composed of long bundles of spindle-shaped cells with large elongated nuclei, hyperchromatic with a nuclear pleomorphism, scattered monstrous cells have also been observed. Mitotic activity was low (1-2 MF / 10 HPF) with absence of necrosis (Figure 2). Smooth muscle cell differentiation is confirmed immunohistochemically by a positive staining of desmin and H-caldesmon with negative staining of CD34, S100, Pancytokeratin and Ki 67 as an index of cell proliferation estimated at 2 percent (Figure 3). Finally, a diagnosis of atypical or bizarre variant of solitary cutaneous leiomyoma was rendered. An unusual presentation of a hereditary leiomyomatosis is suggested. However, the patient refused genetic testing to specify a sporadic or familial form. No recurrence was noted in the 6-month follow-up after surgical excision.
Discussion
Cutaneous pilar leiomyomas are benign smooth muscle tumors that appear between the second and third decades of life as multiple, painful red-brown papulo-nodules. They are located on the face, back and extensor aspect of extremities. Though sporadic in the vast majority, a germline gene mutation responsible for the multiple familial form of these tumors has been identified in the gene that encodes a tumor suppressor enzyme, fumarate hydratase; this has been located in chromosome 1q42.3-43 [3]. It must be remembered that this syndrome also includes uterine fibroids and may be associated with renal cell carcinoma [3,4]. Solitary cutaneous pilar leiomyomas, like our case, are extremely rare, and usually asymptomatic and larger than those encountered in patients with the multiple form.
Pilar leiomyomas are unencapsulated, circumscribed dermal tumors composed of numerous fascicles of smooth muscle in an interlacing and whorled arrangement. An overlying grenz zone is usually present. Individual spindel cells have abundant eosinophilic cytoplasm with blunt-ended, elongated nuclei and perinuclear vacuoles. Differentiating features of genital leiomyomas or leiomyoma metastatic are the presence of a pseudocapsule, larger size, and increased cellularity. Angioleiomyomas are encapsulated tumors composed of interlacing bundles of smooth muscle cells arranged around numerous small, thick-walled blood vessels. A benign smooth muscle tumor generally exhibits an absence of mitoses and cytologic atypia. A review of 53 lesions by Raj, et al. [5]. found up to 28% of leiomyomas with less than 1 mitosis/10 high-powered field and without tumor necrosis.
A leiomyosarcoma is a malignant tumor of smooth muscle. They may be dermal or subcutaneous. Superficial leiomyosarcomas typically present as a solitary lesion on the lower extremities [6]. They are noted to frequently recur following excision; however, they rarely metastasize [7,8]. Wide local excision or Mohs micrographic surgery have been the traditional approaches to treatment of these tumors [8]. Histologically they resemble leiomyomas with anaplastic nuclei and atypical giant cells. The most important microscopic distinction between leiomyoma and leiomyosarcoma is the presence of mitoses. Criteria for the diagnosis of malignancy have varied, with at least 1 mitotic figure per 10 high-power fields favored currently. A recent review of 19 leiomyosarcomas demonstrated 9 or more mitoses per 10 high-power fields in 84% of the tumors [9].
Leiomyomas and leiomyosarcomas also occur in the uterus. A commonly described histologic variant of the uterine leiomyoma is the symplastic leiomyoma.The cardinal features of the symplastic leiomyoma are markedly pleomorphic tumor cells with atypical nuclei, some of which are multinucleated, and a low mitotic rate. Because of the prominent nuclear atypia present within the symplastic leiomyoma they may be misdiagnosed as leiomyosarcomas. Mitotic activity has been the feature most used to discriminate between the atypical leiomyoma and leiomyosarcoma. In a study by Hart and Billman8 that reassessed uterine tumors originally diagnosed as leiomyosarcomas, 13 of the original 28 tumors were reclassified as pleomorphic leiomyomas and followed a benign course. These 13 tumors had 3 or fewer mitoses/10 high-power fields whereas the other 15 tumors showed 6 or more mitoses/10 high-power fields (10).Significant mitoses without the presence of cytologic atypia or necrosis are associated with a favorable clinical outcome.Despite the increased and bizarre cellularity, the symplastic variant has demonstrated a benign course [11].
We believe that our case represents an unusual histologic variant of cutaneous pilar leiomyoma. Mahalingam and Goldberg [12] presented four cases of atypical leiomyomas that all exhibited pleomorphic cells with irregular nuclei and rare mitoses. Each of their cases had a benign course. Three of the patients underwent complete excision, whereas 1 patient underwent excisional biopsy with a positive deep margin which was not reexcised. They suggested that these atypical leiomyomas may represent the analogous cutaneous pattern to uterine symplastic leiomyomas. Our case also demonstrated nuclear hyperchromasia, which initially was felt to represent a leiomyosarcoma; however, upon further review of additional excision specimens, the pattern is felt to more accurately reflect a benign smooth muscle tumor. Although the literature indicates a benign course for these tumors, greater numbers and longer follow-up review will be required.
Conclusion
Comparative studies to assess the prognosis of cutaneous atypical leiomyoma are lacking; however, histopathologic features suggest that cutaneous atypical leiomyoma likely lies in the spectrum between the common cutaneous leiomyoma and malignant leiomyosarcoma. Although evidence of cutaneous atypical leiomyoma progressing to leiomyosarcoma has not been established, cutaneous atypical leiomyoma is frequently treated with conservative excision ensuring complete removal.
- Calonje E, Mackie RM (2004) Soft tissue tumours and tumour like conditions. In Burns DA, Breathnach SM, Cox NH, Griffiths CEM, eds. Rook’s textbook of dermatology, Vol. 7th ed. Oxford: Blackwell Publishing 53: 40.
- Raj S, Calonje E, Kraus M, Kavanagh G, Newman PL, et al. (1997) Cutaneous pilar leiomyoma: clinicopathologic analysis of 53 lesions in 45 patients. Am J Dermatopathol 19: 2.
- Ghaninejad H, Moeineddin F, Rajaee A, Asgari M, Salimzadeh A (2008) Hereditary leiomyomatosis and renal cell carcinoma syndrome: a case report. Dermatol Online J 14: 16.
- Stewart L, Glenn GM, Stratton P, Goldstein AM, Merino MJ, et al. (2008) Association of germline mutations in the fumarate hydratase gene and uterine fibroids in women with hereditary leiomyomatosis and renal cell cancer. Arch Dermatol. 2008 Dec 144: 1584-92.
- Raj S, Calonje E, Kraus M, Kavanagh G, Newman PL, et al. (1997) Cutaneous pilar leiomyoma: clinicopathologic analysis of 53 lesions in 45 patients. Am J Dermatopathol 19: 2–9.
- Orellana-Diaz O, Hernandez-Perez E (1983) Leiomyoma cutis and leiomyosarcoma: a 10-year study and a short review. J Dermatol Surg Oncol 9: 283-7.
- Spencer JM, Amonette RA (1996) Tumors with smooth muscle differentiation. Dermatol Surg 22: 761–8.
- Bernstein SC, Roenigk RK (1996) Leiomyosarcoma of the skin: treatment of 34 cases. Dermatol Surg 22: 631–5.
- Kaddu S, Beham A, Cerroni L (1997) Cutaneous leiomyosarcoma. Am J Surg Pathol 21: 979–87.
- Hart WR, Billman JK (1978) A reassessment of uterine neoplasms originally diagnosed as leiomyosarcomas. Cancer 41: 1902–10.
- Downes KA, Hart WR (1997) Bizarre leiomyomas of the uterus: a comprehensive pathologic study of 24 cases with long-term follow-up. Am J Surg Pathol 21: 1261–70.
- Mahalingam M, Goldberg LJ (2001) Atypical pilar leiomyoma: cutaneous counterpart of uterine symplastic leiomyoma? Am J Dermatopathol 23: 299-303.
FIGURE 1

Figure 1: Clinical image of the firm brown-pink smooth papule on the right upper arm (florid leiomyoma)
FIGURE 2
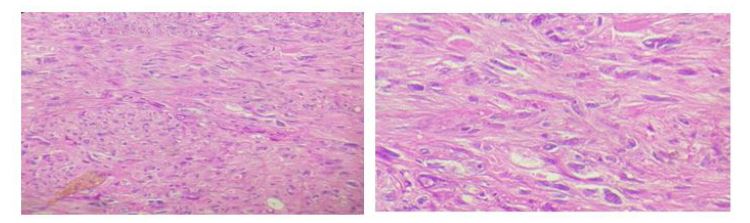
Figure 2: Histologically, the lesion showing long bundles of large spindle cells with a nuclear pleomorphism and without mitotic figures. (Haematoxylin and eosin stain (1Ox) &(40x))
FIGURE 3
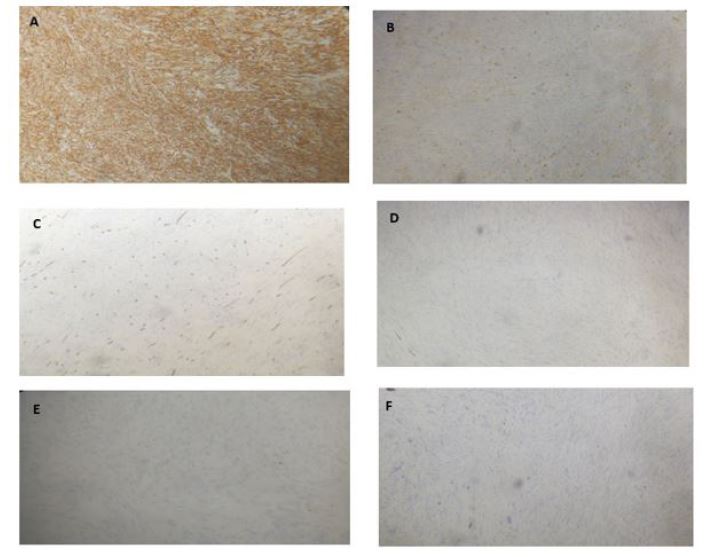
Figure 3: Immunohistochemical studies showing positive staining of H-caldesmon (A) and desmin(B) with negative staining of CD34 (C), pancytokeratin (D) , S100 (E) and a weak index of cell proliferation Ki 67 estimated at 2 percent (F)
Figures at a glance