Breast Ductal Adenoma: Confusion with Carcinoma is Real
Received Date: January 16, 2023 Accepted Date: February 16, 2023 Published Date: February 18, 2023
doi: 10.17303/jpam.2023.3.102
Citation: Yasmine Laraqui, Ismail Boujida, Khouloud Raissouni, Soumaya Echcharif, Selma Bekkarsabein et al. (2023) Breast Ductal Adenoma: Confusion with Carcinoma is Real. J Pathol Allied Med 3: 1-5.
Abstract
Breast ductal adenoma is a rare benign tumor of the breast that frequently occurs in women over 50 years-old, arising from small to medium-sized ducts. There are many overlapping clinical, radiological and histological features with invasive breast carcinoma, making the diagnosis difficult. We report here a case of a 59-year-old woman presented with a breast palpable mass, in whom, the histological and immunohistochemical studies led to the diagnosis of ductal adenoma.
Keywords: Breast; Adenoma; Invasion.
Introduction
Adenomas of the breast are rare benign tumors including three subtypes: tubular, lactating and ductal.Ductal adenoma is a solid benign tumor involving small or medium-sized ducts. It usually occurs in patients over 50 years. It may evolve by sclerosis of intraductal papillary lesion. Ductal may mimic carcinoma, clinically and radiologically. This is why meticulous histological study is essential to identify this lesion as benign and avoid confusion with carcinoma that is obviously of great practical importance.
Case report
A 59-year-old woman presented with a palpable mass of the right breast, first noted ten years earlier.
There was no history of breast pain or nipple discharge.
Clinical examination revealed a 4 cm sized firm mass without nipple retraction or skin change. There was no associated axillary lymphadenopathy, and the left breast was normal.
A mammography showed a nodule of fluid density with ill-defined margin and lobulated in places. Sonography showed a hypoechoic, ill-defined nodule. These radiological findings suggested malignancy (ACR 5).
Microbiopsy was made twice and came back in favor of tubular adenoma, supported by immunehistochemical study (Figure 1a).
Due to the discrepancy between histological and radiological findings, an excisional biopsy was performed.Macroscopically, the nodule was unique, firm, round,whitish, well circumscribed and measuring 7 cm in maximum diameter.
Histological examination showed proliferative glandular structures bordered by epithelial and myoepithelial cells within a central area of dense scar-like fibrosis. The stroma was fibrous and abundant,compressing the epithelial structures and reducing their lumen giving an appearance of pseudo-invasive streaks (Figure 1b). Adjacent breast parenchyma exhibited apocrine metaplasia (Figure 1c).
We have completed by immunohistochemical study to identify the epithelial and myoepithelial cells by using myoepithelial markers like SMA (Figure 2a) and p63 (Figure 2b). SMA was also positive for stromal myofibroblasts.
Ductal adenoma diagnosis was retained. Postsurgery evolution was favorable.
Discussion
Ductal adenoma is a rare and benign breast proliferation. It mainly occurs in the sixth decade of life. It was initially described in 1984 and called “sclerosing papilloma” in WHO 2012. Ductal adenoma is a solid benign tumor involving medium- sized and small ducts, but rarely involves large sized ducts. They are usually unilateral, but may be bilateral in patients with Carney syndrome [1].
Ductal adenoma may simulate carcinoma, clinically and radiologically. This is why the correct histological diagnosis is primordial for a good patient care and to avoid confusion with carcinoma.
Ductal adenoma most likely derives from intraductal papilloma due to a myofibroblastic proliferation resulting in loss of the arborizing papillary architecture.Besides, the studies have confirmed the existence of AKT1 mutations in both entities, supporting the close relationship between them [2].
Clinically, ductal adenoma usually presents as a palpable mass or with nipple discharge when large ducts are involved. The diagnosis can be made after several weeks or even several years.
Mammography usually reveals a round mass, well delineated with smooth margins, sometimes with calcifications. Breast ultrasound shows well-defined and hypoechoic nodule with posterior enhancement [3].
Macroscopically, the lesion may present as single or multiple rounded lesions, measuring between 0.5 to 5 cm. On cut surface, they are lobulated, whitish, with central gray softening, and with gritty texture.
Histological study shows an adenomatous benign proliferation surrounded by a dense fibrous wall. It is composed of glands arranged in organized parallel pattern,with centrifuge radiations from the center to the periphery. The glandular structures are bordered by a double layer of epithelial and myoepithelial cells, with moderate atypia and rare mitosis. They are separated by a fibrous stroma that may compress and obliterate them. This “pseudo invasive” aspect can lead to a misdiagnosis because it can mimic invasion in a core biopsy [1].
So, differentiation into epithelial and myoepithelial cells is the most important feature to affirm the benign nature of this lesion.
The adjacent breast parenchyma may show sclerosing adenosis, cystic duct ectasia or apocrine metaplasia which support the diagnosis. It is present in over half of cases, like we have seen in our presented case.
The immunohistochemical study can be used to confirm the presence of both tubular luminal cells (cytokeratin +) and tubular basal cells (PS100+, SMA+,p63+). Stromal spindle cells are SMA+ and Vimentin +.Negativity of p53 and low Ki67 support the benign nature of this lesion [2].
All this reflects the importance of providing a detailed interpretation of the histological feature to distinguish ductal adenoma from invasive breast carcinomas (Table 1: Ductal adenoma VS invasive carcinoma) and allow the patient a correct treatment which consists of a simple surgical excision.
Conclusion
Ductal adenoma is an uncommon benign tumor and can clinically, radiologically and even histologically simulate malignancy. Therefore, a careful interpretation of histological findings is essential to minimize the very real danger of confusion with carcinoma.
Declarations
Funding
No external funding sources are relevant to this submission.
Ethics approval and consent to participate
This case report was approved by the Ethics Committee of Faculty of medicine and pharmacy Mohammed V University Rabat.
Additional patient consent for this retrospective study was not required.
Consent for publication
Written informed consent for publication of their clinical details and/or clinical images was obtained from the patient. A copy of the consent form is available for review by the Editor of this journal.
Competing interests
The authors declare that they have no competing interests.
- Azzopardi JG, Salm R (1984) Ductal adenoma of the breast: a lesion which can mimic carcinoma. J Pathol. Sept 144: 15-23.
- Kaya H (2018) Ductal Adenoma. In: van Krieken JHJM, éditeur. Encyclopedia of Pathology [Internet]. Cham: Springer International Publishing;
- Weerakkody Y (2018) Ductal adenoma of the breast | Radiology Reference Article | Radiopaedia.org [Internet].Radiopaedia;
FIGURE 1
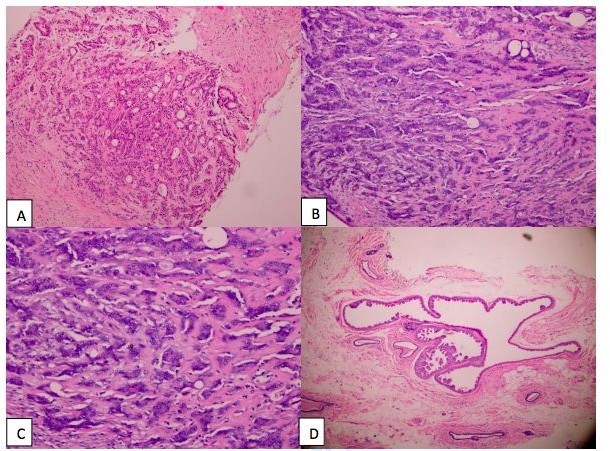
Figure 1a: Tubular proliferation showing proliferative glandular structures bordered by a double layer of epithelial and myoepithelial cells (Haematoxylin and eosin x100)
Figure 1b: Proliferative glandular structures bordered by epithelial and myoepithelial cells within a central area of dense scar-like fibrosis. (Haematoxylin and eosin x100)
Figure 1c: The stroma was fibrous and abundant compressing the epithelial structures and reducing their lumen giving an appearance of pseudo-infiltrative streaks. (Haematoxylin and eosin x200)
Figure 1d: Adjacent breast parenchyma exhibited apocrine metaplasia (Haematoxylin and eosin x100)
FIGURE 2
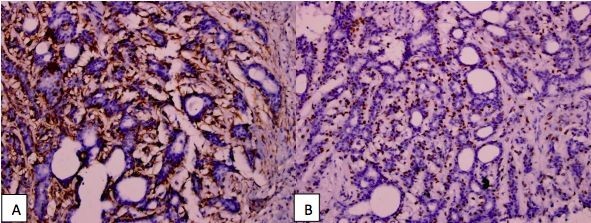
Figure 2a: positive staining of tubular basal cells and stromal myofibroblasts with SMA antibody
Figure 2b: positive staining of tubular basal cells with p63 antibody.
Tables at a glance
Figures at a glance