Type I Transmigration of Permanent Mandibular Right Canine – Report of aRare Case
Received Date: June 07, 2023 Accepted Date: July 07, 2023 Published Date: July 10, 2023
doi: 10.17303/jpam.2023.4.101
Citation: Nagaveni NB (2023) Type I Transmigration of Permanent Mandibular Right Canine – Report of a Rare Case. J Pathol Allied Med 4:1-5
Abstract
Transmigration is a rarely seen dental anomaly and very few cases have reported in the literature. It is the phenomenon characterized by crossing of impacted canine through midline to the opposite of the mandible. Based on the degree of crossing it can be classified into many types. The most commonly affected tooth by this process is the mandibular canine. Knowledge about this anomaly is very essential among clinicians is very important to provide utmost care for the patient. The aim of this article is to present such a rare occurrence of transmigration of mandibular right canine in an Indian patient and also briefly reviews the literature pertaining to this rarest anomaly.
Keywords: Transmigration; Mandibular Canine; Impacted Canine; Classification; Dental Variation
Introduction
Developmental dental anomalies are the anomalies pertaining to the dental structure and can be seen by general practitioners during clinical practice. An awareness and knowledge of dental anomalies is essential among clinicians to rule out, proper diagnosis and also to render meticulous treatment for the patient. Transmigration of permanent tooth refers to the phenomenon of a permanent tooth crossing the midline of the jaw and migrating towards the opposite side [1]. It is a rare occurrence, with a prevalence ranging from 0.14% to 0.61% in the general population. It is important to note that transmigration is a relatively rare phenomenon, with a reported incidence ranging from 0.14% to 0.9% [2,3]. The exact cause of transmigration is unknown,but it is believed to be related to genetic factors and environmental influences such as trauma, infection, and crowding [4]. Transmigration can occur in both the upper and lower jaws, but is more common in the lower jaw, with the mandibular canine being the most frequently affected tooth [5]. The condition is often asymptomatic and may go unnoticed during clinical practice because they are always hidden and accidentally noticed on routine radiographic examination.Some cases, it can lead to complications such as impaction, resorption, and root dilaceration [6]. Early diagnosis and management of transmigration are crucial in preventing these complications and preserving dental function.Treatment options include orthodontic intervention, surgical extraction, or transplantation of the transmigrated tooth to its correct position [7].
Case Report
A 56 year female patient reported a private dental office wishing to replace her many missing teeth. Patient appeared moderately built and nourished with no signs and symptoms of any systemic or metabolic disorder. On intraoral examination, only maxillary anterior teeth including central,lateral incisors, canine, first premolar on right side, central, lateral incisors, canine and only second molar was present on the left side. In the mandibular arch, on the left side,central lateral incisors, canine, first and second premolars and second molars were present. On the right side only central,lateral incisor and both premolars were present.Mandibular right canine appeared to be missing. Patient’s oral health was poor with severe periodontal problem. On further examination of the oral cavity patient also exhibited an old broken removable partial denture along with some fixed prosthetic components. Patient had lost many permanent teeth due to periodontal problem, as a result the occlusion was not proper. An orthopantograph radiograph was taken which showed an impacted mandibular right canine(Figure 1). The canine was placed slightly angulated and deviated towards the occlusal level. The crown of the canine was facing towards midline and the root opposite side.About one third of the crown of the impacted canine crossed the midline. On left side the canine erupted in normal place in vertical position. Based on literature search the case was diagnosed as transmigration and belonged to type I category. As tooth was in asymptomatic condition no treatment was carried out. Addressing patient chief complaint a removable prosthesis was planned.
Discussion
Etiology and Prevalence
The etiology of transmigration is not well understood,but several theories have been proposed. One theory suggests that transmigration may be caused by genetic factors,as there have been reports of familial clustering of cases[8]. Another theory suggests that transmigration may be related to early loss of deciduous teeth, leading to altered growth patterns in the mandible. Additionally, some studies have suggested that transmigration may be associated with certain craniofacial anomalies, such as agenesis of the mandibular incisors [9]. Some researchers have also proposed that transmigration may be related to abnormal root development of the mandibular canines, as well as abnormal placement of the dental follicle [10]. Others have suggested that transmigration may be related to environmental factors, such as trauma or infection. The etiology of transmigration of mandibular canines is not well understood and may be multifactorial, involving genetic, developmental,and environmental factors.
Types
There are two types of transmigration of permanent teeth: complete transmigration and incomplete transmigration.Complete transmigration is when the tooth completely crosses the midline and erupts on the opposite side of the jaw. This is a rare occurrence and has been reported in only a few cases [11].
Incomplete transmigration is when the tooth partially crosses the midline but fails to completely erupt on the opposite side of the jaw. This is the most common type of transmigration and is seen more often in mandibular canines.Incomplete transmigration can be further classified into three subtypes based on the degree of migration: Type 1, Type 2, and Type 3. Type 1 is when the tooth is partially impacted in the mandible and can be seen on the opposite side of the jaw. Type 2 is when the tooth is partially impacted in the maxilla and can be seen on the opposite side of the jaw. Type 3 is when the tooth is completely impacted and cannot be seen on the opposite side of the jaw [12,13].
Diagnosis
The diagnosis of transmigration involves clinical examination and radiographic assessment [15,16]. The clinical examination includes visual inspection and palpation of the affected area to detect any abnormality in the position,shape, or mobility of the tooth. However, the radiographic assessment is considered the gold standard for the diagnosis of transmigration such as involves taking a panoramic radiograph [17].
The panoramic radiograph helps to confirm the diagnosis of transmigration by showing the position of the tooth relative to the midline and adjacent teeth, the degree of inclination, and the extent of migration [18]. In some cases,cone-beam computed tomography (CBCT) may also be used to obtain a more detailed image of the transmigrated tooth and its surrounding structures [19]. Furthermore, it is important to differentiate transmigration from other dental anomalies, such as impacted teeth, odontomas, and dentigerous cysts, which may have similar clinical and radiographic features [20]. Therefore, a thorough examination and analysis of the radiographic images are essential for an accurate diagnosis and treatment planning. Sometimes it is observed with other dental anomalies. Nagaveni et al in 2011 reported concomitant occurrence of canine transmigration and symmetrical agenesis of mandibular both central incisors [21]. Later in 2012, the same author published an unusual occurrence of a combination of dental anomalies like mandibular canine transmigration (type I), taurodontism in permanent mandibular molars, congenital agenesis of 14 numbers of permanent teeth excluding third molars, canine impaction, primary molars with pyramidal roots, midline diastema and generalized microdontia in an apparently normal 13-year-old Indian girl [22].
Treatment
The treatment of transmigration is dependent on the position and eruption status of the tooth and biological conditions. The different treatment modalities considered are surgical, orthodontic and prosthetic dental treatment. If the tooth is fully erupted and functional, no treatment may be necessary. However, if the tooth is impacted or partially erupted, surgical intervention may be required to bring the tooth into alignment. The surgical approach could be either orthodontic or oral surgical procedure [21]. Orthodontic management includes orthodontic traction, which involves applying forces to move the tooth to the normal position [11]. Oral surgical treatment involves surgical exposure of the impacted tooth and attachment of an orthodontic appliance for the alignment of the tooth [22]. If there is enough space for the transmigrated canine, and when mandibular incisors are in a normal position, transplantation is suggested.
- Olate S, Lyrio MC, de Moraes M (2015) Transmigration of mandibular canines–a systematic review. Dent Traumatol 31: 1-6.
- Alqerban A, Jacobs R, Fieuws S, Willems G (2014) Transmigration of mandibular canines: prevalence, aetiology and treatment. A systematic review. Eur J Orthod 36: 263-71.
- Grover PS, Lorton L (1985) The incidence of unerupted permanent teeth and related clinical cases. Oral Surg Oral Med Oral Pathol 60: 170-5.
- Al-Nimri KS (2008) Transmigration of mandibular canines: a review of the literature and a report of five cases. J Contemp Dent Pract 9: 1-10.
- Ballal S, Sachdeva GS, Kandaswamy R (2008) Transmigration of mandibular canines: a report of six cases and review of literature. J Conserv Dent 11: 37-42.
- Xie Q, Shen G, Chen Y et al. (2012) Transmigration of impacted mandibular canines: a retrospective study of 272 patients and literature review. J Oral Maxillofac Surg 70:438-44.
- Kapila S, Conley RS, Harrell WE Jr. (1999) The current status of transmigration of mandibular canines: a review.Am J Orthod Dentofacial Orthop 116: 610-4.
- Becker A, Chaushu S (2015) Etiology of maxillary canine impactions: a review. Am J Orthod Dentofacial Orthop 147: 555-62.
- Kaczor-Urbanowicz KE, Zadurska M, Antoszewska--Smith J, Kozakiewicz M (2016) Transmigration of mandibular canines: a retrospective analysis of 15 cases and a review of literature. Adv Clin Exp Med 25: 343-8.
- Soares EC, Moura LB, Moura MS, Farias LC, Oliveira BH, Santos VdeC (2010) Transmigration of canine - review of literature and case report. J Oral Maxillofac Res 1: 4.
- Bhaskar DJ, Gupta KK (2011) Transmigration of mandibular canine: a review of literature and report of two rare cases. Natl J Maxillofac Surg 2: 200-3.
- Khandelwal V, Gupta S (2011) Incomplete transmigration of mandibular canine: a case report. J Oral Maxillofac Surg 69: 327-30.
- Parolia A, Kundabala M, Dahal M (2009) Transmigration of mandibular canine: report of two cases and review of literature. Med Oral Patol Oral Cir Bucal 14: 469-72.
- Lai CS, Bornstein MM, Mock L, Keglevich T, Buser D(2008) Transmigration of mandibular canines: a report of six transmigrated teeth and review of the literature.Quintessence Int 39: 45-51.
- Yan B, Shao J, Jia Q, Chen Z (2008) Transmigration of mandibular canines: a report of six cases and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 106: 27-32.
- Subramaniam P, Babu KL, Sunny J, Rajaraman V (2014) Bilateral transmigration of mandibular canines - a case report. J Clin Diagn Res 8: 19-20.
- Gungor K, Celikoglu M, Yildirim E, Ozkan BT (2010) Transmigration of impacted mandibular canines: report of six cases and review of literature. Quintessence Int 41:613-9.
- Sujatha GP, Reddy SK, Reddy LV, Ravikumar P (2007) Transmigration of impacted mandibular canine: a case report. J Indian Soc Pedod Prev Dent 25: 93-6.
- Garg R, Tandon S (2002) Transmigrant mandibular canines: a report of two cases. J Clin Orthod 36: 149-52.
- Arslan A, Demirbas AE, Deger Y, Ozturk F (2015) Bilateral transmigration of mandibular canines: a rare case report.Case Rep Dent 354231.
- Nagaveni NB, Radhika NB, Umashankara KV,Satisha TS (2011) Concomitant occurrence of canine transmigration of symmetrical agenesis of mandibular incisors – A case report. Bangladesh J Med Sci 10: 133-6.
- Nagaveni NB (2012) An unusual occurrence of multiple dental anomalies in a single non-syndromic patient: A case report. Case Report Dent 426091: 4.
FIGURE 1
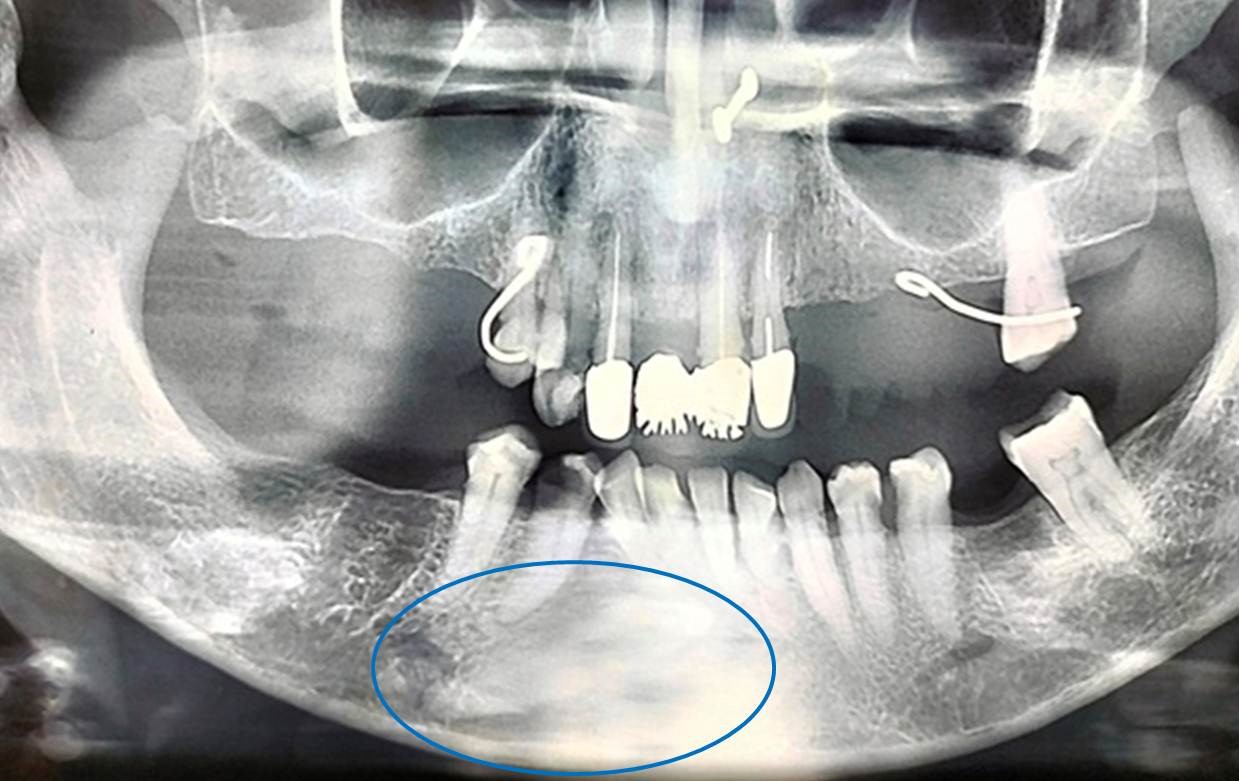
Figure 1:Orthopantomograph showing transmigrated mandibular right canine-Type I (blue circle)
Figures at a glance