Safety, Tolerability, and Adherence of Antiretroviral Regimens Containing Long-acting HIV Fusion Inhibitor Albuvirtide for HIV Post-Exposure Prophylaxis
Received Date: September 20, 2021 Accepted Date: October 20, 2021 Published Date: October 21, 2021
doi: 10.17303/jpdm.2021.4.104
Citation: Jingmin Nie (2021) Safety, Tolerability, and Adherence of Antiretroviral Regimens Containing Long-acting HIV Fusion Inhibitor Albuvirtide for HIV Post-Exposure Prophylaxis. J Pharmacol Drug Metab 4: 1-12.
Abstract
Background: There have been no prospective clinical studies investigating adherence and safety of HIV post-exposure prophylaxis (PEP) in China. Tolerability, adherence, and transmitted drug resistance are concerns, especially when single tablet regimen (STR) usage is low. The present study aimed to explore the safety, tolerability and adherence of co-administration of albuvirtide (ABT) with other non-STR antiretrovirals for HIV PEP.
Methods: This was a prospective, open-label, multicenter cohort study. The subjects were stratified into 3 groups based on their preference: ABT+DTG (Group 1), ABT+TDF+3TC (Group 2), and DTG+TDF+3TC (Group 3). All enrolled subjects received PEP within 72 hours after exposure and continued for 28 days and were followed-up for 12 weeks.
Results: A total of 330 participants were enrolled into the three groups. Most participants were male (87.2%). Sexual exposure was the most frequent mode of exposure (91.9%). The average time from exposure to treatment was 26.8 ± 19.5 hours. There were no statistically significant differences between the three study groups with respect to completion of oral medication at 28 days. Compared to the oral drugs, the 28-day completion rate and adherence of ABT was significantly higher, being 88.9% vs. 64.0%, and 94.4% vs. 75.7% respectively (p<0.0001). Subjects in the ABT-containing Group 1 and Group 2 exhibited higher adherence than those in all oral drug regimen Group 3 (p<0.05). None of the participants reported serious adverse events led to withdrawal from the study. All the drug regimens were found to be safe and well-tolerated. No HIV incident case was observed during study period.
Conclusion: ABT-containing regimens (ABT+DTG or ABT+TDF+3TC) offer a good option for HIV PEP due to higher completion rates than the DTG+TDF+3TC regimen. The overall safety was comparable and acceptable among three groups.
Keywords: HIV; Post-Exposure Prophylaxis; Safety; Adherence; Albuvirtide
Introduction
Global HIV/AIDS statistics estimates approximately 38 million people living with HIV worldwide up to the end of 2019, with about 1.7 million new infections and 690,000 deaths occurring in 2019 [1,2]. In China, the HIV morbidity, mortality, and rates of new infection have increased from 0.235/100,000, 0.057/100, and 1.020/100,000 in 2004 to 3.990/100,000, 1.034/100, and 6.442/100,000 in 2016, respectively despite of the country’s unremitting efforts [3]. Currently, some of the strategies developed specifically for HIV prevention in China include treatment as prevention (TasP), active work towards the WHO 90-90-90 targets, pre-exposure prophylaxis (PrEP) and post-exposure prophylaxis (PEP), detection and treatment of sexually transmitted infections (STIs), prevention of mother-to-child transmission, condom use promotion, and safe blood donation [4]. Antiretroviral therapy (ART) is considered the best option for TasP and PEP to prevent HIV transmission and infection [5].According to recommendations of the International Antiviral Society-USA panel and China AIDS Guidelines (2018 edition), ART should be provided immediately to newly exposed individuals to ensure HIV-negative serostatus. Dolutegravir (DTG), lamivudine (3TC), tenofovir disoproxil fumarate (TDF), bictegravir (BIC), and emtricitabine (FTC) are the recommended drugs for HIV PEP by current guidelines [6,7]. Three-drug regimens, including three-drug single tablet regimens (STRs), are usually recommended as PEP regimens for high-risk individuals. However, STRs are not widely available in China and adherence is always a concern when using non-STR three-drug ART for HIV PEP. Additionally, given the importance of PEP and more than 100,000 new reported HIV infections annually in China, there is no prospective PEP clinical study reported up to date [3].
The effectiveness of PEP has been demonstrated in several previous studies, but poor adherence and low completion rates were concerning observations in those studies which warrant further improvement [8-10]. There is a demand for PEP regimens that could overcome challenges of poor adherence, severe AEs, and dosing convenience. Two previous studies using co-formulated single-tablet regimens (elvitegravir/cobicistat/tenofovir disoproxil fumarate/emtricitabine) of HIV PEP found that majority of participants achieved a higher drug completion rate (>70%) and favorable drug tolerance [11,12]. However, the usage of these single-tablet regimens was low in China.
Using parenteral long-acting antiretrovirals, may be another strategy for improving adherence, tolerability, and convenience,and thereby have the potential to enhance expected outcomes. Preliminary animal PrEP studies have shown that long-acting cabotegravir can prevent simian/HIV acquisition from rectal, vaginal, and intravenous challenge [13]. Another study has demonstrated that monthly administration of long-acting cabotegravir and rilpivirine was non-inferior to daily oral administration of TDF/FTC for PrEP in mice [14]. In HPTN083 and HPTN084 studies, cabotegravir showed superiority to oral TDF/FTC for HIV PrEP in male having sex with men (MSM) and cisgender women [15,16].
Albuvirtide (ABT) is a long-acting 3-maleimimidopropionic acid (MPA)-modified peptide that binds to human serum albumin and inhibits HIV fusion. The binding of ABT with serum albumin to form a conjugate is responsible for its extended half-life of 12 days [17,18], and reduces the need for frequent intravenous administration [19]. The phase 3 TALENT study indicated that the dual regimen of ABT (weekly infusion) and LPV/r (oral daily) was well tolerated and non-inferior to the WHO-recommended second-line three-drug regimen in HIV patients with first-line treatment failure [20]. ABT is approved by China National Medical Products Administration (NMPA) for marketing in 2018. In real-world practice, it is widely used in patients with HIV-1 infection and has been proven with good safety and effectiveness. Due to the unique features of ABT, such as long-acting, intravenous administration, not metabolized by CYP450 liver enzymes and subsequently less drug-drug interactions, the real-world clinical application has extended to special populations with higher unmet medical needs such as patients with hepatic impairment or renal impairment, perioperative use for abdominal surgery, hospitalized patients with critical conditions and treatment-naïve HIV-infected patients with or without AIDS [21-23].
The present study aimed to explore the safety, tolerability, adherence, and effectiveness of co-administration of ABT with other non-STR antiretrovirals for HIV PEP. Subjects were treated with 2 injections (1st and 15th day) of ABT combined with 1 integrase inhibitor (INSTI) or 2 nucleotide/nucleosides (NRTIs). Comparing to the traditional three-drug non-STR PEP treatment, we hypothesize that ABT-containing regimens may offer a better option by reducing pill burden, and improving adherence, and the potential benefits of ABT use in PEP may be associated with the fact that it blocks viral fusion and acts early in the viral life cycle, reaches inhibitory drug concentration rapidly in blood by injection, and it exhibits high resistance barrier and long half-life.
Methods
Study design and participants
This was a prospective, open label, multicenter cohort study conducted at three clinical centers in China, including Chongqing Public Health Medical Center, Kunming Third People’s Hospital, and The First Hospital of Changsha. Randomized design was not used to minimize the complexity of this cohort study. The three treatment options were offered, and participants chose based on their preference.
The study was registered in Chinese Clinical Trial Registry with registration number (ChiCTR1900022881, http://www.chictr.org.cn/showprojen.aspx?proj=37395) and was approved by the Ethics Committees at each of the participating centers, and the study was conducted in accordance with the tenets of the Declaration of Helsinki. All participants provided written informed consent.
Subjects with HIV exposure visiting these clinical centers between May 2019 and December 2019 were enrolled for the study. All subjects were asked to provide their history of exposure. A rapid HIV antibody examination was performed for all subjects within 72 hours of exposure to initiate the first preventive drug use. The inclusion criteria included: (1) persons above 18 years of age; (2) with a history of HIV exposure within 72 hours through damaged skin-stabbing or cuts and/or contaminated skin/mucous membrane or unprotected sexual intercourse with a suspected or confirmed HIV positive person; (3) tested negative for HIV antibody and urine pregnancy testing after exposure; (4) and provided signed informed consent. Urine pregnancy tests were performed only for women. Persons with known HIV infection (HIV-positive) or with known hepatitis B virus (HBV) infection, persons who had exceeded the exposure time limit of 72 hours, persons who were known to have allergic reactions or were intolerant to PEP drugs or excipients, and women who were pregnant, breastfeeding or planning a pregnancy were excluded from the trial.
The subjects were stratified into 3 groups based on their preference: ABT+DTG (Group 1), ABT+TDF+3TC (Group 2), and DTG+TDF+3TC (Group 3). All enrolled subjects received PEP within 72 hours after exposure and continued for 28 days and were followed-up for 12 weeks. The primary measurements were the 28-day drug completion rate and adherence, HIV sero-conversion and occurrence of adverse events.
Study Procedure
Based on the principle of starting prophylactic medication as early as possible after high-risk HIV exposure, the collection of high-risk exposure history, informed consent, HIV antibody test results, urine pregnancy test results (only for women), vital signs and physical examination was completed rapidly, and the first preventive medication was administered within 72 hours after exposure.
The drugs utilized in the present study and their respective dosages were as follows: ABT, 320mg, given intravenously on day 1 and day 15; DTG, 50mg, taken orally, once a day for 28 days; TDF, 300mg, orally once a day, for 28 days, and 3TC, 300mg, orally once a day, for 28 days. Post-exposure prophylactic therapy was initiated in all the subjects within 72 hours of exposure. Medication was continued for 28 days, and subjects were followed up for 12 weeks.
The results of laboratory examinations at the Day 1 visit (blood cell count, biochemistry, urinalysis, HBV markers, hepatitis C antibody, and syphilis markers) were used as baseline data. Follow-up visits were conducted on Day 14, Day 28, Week 8, and Week 12 to evaluate blood testing results and urinalysis, drug adherence, adverse reactions, anti-HIV antibody test, vital signs, and physical examination.
Based on drug distribution records, study doctors calculated the percentage of subjects who completed the 28-day ABT and oral prophylaxis drug regimens. The 28-day individual adherence rates to ABT and each of the oral drugs were calculated concurrently, and the adherence rates to each regimen were calculated at the same time. In the two-drug regimen of Group 1, each drug was weighted as 1/2 weights, while in the three-drug regimens of Groups 2 and 3, each drug was weighted as 1/3 weights. The effectiveness of prophylaxis was evaluated by calculating the HIV infection rates at 28 days and 12 weeks. Safety evaluation included recording and evaluating the incidence of adverse events and adverse reactions, physical examination, and the results of laboratory tests such as hematology, blood biochemistry, and urinalysis.
Outcomes
The primary measurements were the 28-day drug completion rate, adherence, HIV sero-conversion and occurrence of adverse events. The percentage of subjects who had completed 28 days of ABT and oral PEP medications was calculated based on drug distribution records. The 28-day drug adherence rate to ABT and the oral drugs was calculated, and the regimen adherence rate of the three groups was calculated. The formula used to calculate drug adherence (%) was consumed doses/prescribed doses ×100%. Safety endpoints included the recording and evaluation of the occurrence of adverse events. The HIV sero-conversion included the HIV infection rate at day 28 and week 12.
Statistical Analysis
Continuous data sets were expressed as percentages, mean ± standard deviation, median (upper range and lower range), and classified data sets as percentage and event frequency. The Chi-squared test and Fisher’s Exact test were performed to compare categorical variables. Continuous variables were compared using the paired t-test and the F-test (ANOVA-analysis of variance) was used for multiple comparisons with T correction. Statistical significance was set at a p-value of 0.05, and CIs at 95%. All statistical analyses were performed using SAS software (version 9.5, SAS Institute Inc., Cary, NC). The Safety Set (SS) included all subjects who received the assigned PEP medications. The Full Analysis Set (FAS) included all subjects except those with negative HIV exposure sources and Hepatitis B Infection.
Results
Study participants and baseline characteristics
A total of 330 subjects were enrolled and stratified into three groups: Group 1 (ABT+DTG), Group 2 (ABT+TDF+3TC), and Group 3 (DTG+TDF+3TC), with 126, 104 and 100 subjects in each group respectively. The safety set (SS) included all 330 participants. The full analysis set (FAS) comprised 297 participants, with 99 subjects each per group, after excluding 4 subjects whose exposure source was confirmed to be negative and 29 cases who were confirmed to have hepatitis B infection. Figure 1. illustrates the distribution of subjects in the study.
The participants were mostly men (87.2%), their mean age was 31.58±8.82 years, and 92.2% of them were of the Chinese-Han ethnicity. There were no significant differences in mean height or weight between the study groups. With regards to mode of exposure, sexual exposure was calculated to have highest proportion in all three groups (90.9%, 88.8% and 95.9%, respectively). Vaginal intercourse was the most prevalent mode of sexual exposure, at proportions of 70.7%, 59.6%, and 56.3%, respectively. The overall average exposure time was 26.8 ±19.5 h. More than half of the study participants in each of the three groups-initiated PEP therapy within 24 hours of exposure (51.5%, 58.2%, and 58.5%, respectively) (Table 1).
The percentage of subjects who completed Day 15 visits in the three groups was 89.9%, 85.9%, and 64.6%, respectively. And the percentage of subjects who completed Day 28 visits in the three groups were 55.6%, 52.5%, and 53.5%, respectively. Those who completed Week 12 visits were 55.6%, 57.6%, and 52.5% in the three groups, respectively. Compared to Day 15 visits, there was a decrease in the proportion of subjects who completed Day 28 and Week 12 visits (Figure 1).
Drug Completion
Of the total of 297 participants included in the FAS, 91.9% of Group 1 participants and 85.9% of Group 2 participants completed 2 infusions of ABT. The proportion of subjects who completed 14 days of oral drug prophylaxis in each of the three groups was 91.9%, 85.9% and 80.8%, respectively. Overall, 64.0% (190/297) of the subjects completed 28 days of oral drug prevention with proportions of 63.6%, 64.6%, and 63.6% in each of the three groups, respectively. There was no significant difference in the rates of oral medication completion over 28 days between the three groups. The 14-day and 28-day completion rate of ABT was significantly higher than the oral drug completion rate (p<0.0001) for all subjects (Table 2).
Drug Adherence
In the FAS population, the 28-day drug adherence rate to ABT, oral medication, and combination therapy was 94.4±15.8%, 75.7±36.0%, and 80.5±31.4%, respectively. A significantly higher adherence rate to ABT than to oral drugs was observed in all subjects (p<0.0001) and in subjects of Group 1 and 2. For the oral medication, the adherence rates in Group 1 and 2 were slightly higher than Group 3, but without statistically significant difference. Group 1 participants and Group 2 participants exhibited higher adherence to their respective therapeutic regimens, compared to Group 3 participants, with a statistically significant difference in between Group 1 and 3 (p<0.01) (Table 3).
HIV Infection Rate
Among the 297 participants in the FAS, 73.1% (217/297) underwent HIV antibody testing during the period between Day 15 and Week 12 after the administration of the first prophylactic drug, but none of the participants were found to be positive.
Adverse Events
None of the participants in the SS reported adverse events that would have led to withdrawal from the study. In Group 1 (ABT+DTG), 28.6% subjects had 54 adverse events of severity grade 1 to 2. Common adverse events were dizziness (7.9%), diarrhea (6.4%), and fatigue (4.8%). In Group 2 (ABT+TDF+3TC), 49 adverse events of severity grade 1 to 2 were observed in 34.6% subjects. Notably, one subject (1.0%) developed tuberculosis, but this diagnosis was deemed to be unrelated to the drugs used in our study. Common adverse events were dizziness (7.7%), diarrhea (4.8%), and abnormal liver functions (4.8%). In Group 3 (DTG+TDF+3TC), 28% subjects had 42 adverse events of severity grade 1 to 2. Common adverse events were elevated triglycerides (7.0%), dizziness (7.0%), and fatigue (5.0%) (Table 4).
Discussion
To the best of our knowledge, our study is the first prospective study in China aiming at providing clinical evidence of injectable antiretroviral containing PEP regimens. Results of our study revealed that the 28-day completion rate and drug adherence rate of ABT was significantly higher than that of the oral drugs, that no subjects tested seropositive for HIV at the termination of the study, and that co-administration of ABT with oral drugs was found to be safe, effective, and well tolerated.
In our cohort, sexual exposure was the predominant mode of exposure, while occupational exposure accounted for only 2.7%. Among those with sexual exposure, vaginal intercourse was the most prevalent sexual method of exposure in our study. This observation differs from that of a prospective study conducted in Paris wherein the primary mode of sexual exposure was anal sex in 65% of patients, while vaginal intercourse accounted for only 26% of cases [24]. However, an observational, cross-sectional study of 678 patients in Spain found vaginal intercourse (99.2%) to be the commonest sexual method of HIV exposure [25].
Our study showed that the 14-day and 28-day completion rate of ABT was significantly higher than the oral drug completion rate for all subjects. The adherence rates to prescribed regimens in Groups 1 and 2 were higher than that in Group 3, with a statistically significant difference. A significant increase in adherence rates to ABT than to oral drugs was noticed in all subjects. Comparing the adherence of all subjects to ABT and oral drugs, we found that the adherence rate to ABT was higher, with a statistically significant difference in adherence rates. This is an expected outcome that replacing 2 NRTIs with an injectable (ABT) may facilitate the PEP drug completion rate. The above findings also suggested that biweekly administration of ABT was well-accepted by most of the participants and could significantly improve drug completion rate. In addition, a significant reduction in the proportion of subjects who completed the oral medication for 14 days was observed in Group 3 as compared to Group 1, indicating that the higher pill burden contributed to the lower completion rate in Group 3.
A similar study conducted in Barcelona, Spain, in which 157 patients with potential sexual exposure to HIV, reported a higher non-completion rate using lopinavir/ritonavir (47%) versus elvitegravir/cobicistat (33%). Significantly poor adherence to PEP and more adverse events were reported in the lopinavir/ritonavir group versus the elvitegravir/cobicistat group (47% vs 9%, p=0.0001 and 90% vs 49%, p=0.0001, respectively) (10). This observation further emphasizes the fact that using a larger number of individual oral medications for PEP is potentially likely to be responsible for poor drug compliance.
In the present study, the completion rate of all subjects for preventive oral drugs was 64.0%, and drug adherence was observed to be 75.7%, indicating that a large proportion of subjects were unable to consume oral drugs on a regular basis, or discontinued the medication. ABT is a long-acting injectable drug approved for antiretroviral use in China [26]. In our study, ABT was administered on the 1st and 15th day. The low-frequency administration, and compulsory hospital infusion resulted in a 28-day drug completion rate (88.9%) and adherence rate (94.4%) of ABT to be significantly more favorable than that of oral drugs. The combination of ABT with DTG showed the highest completion and adherence rates. This signifies that a simplified two-drug regimen which includes a long-acting injectable drug has the potential to improve drug adherence in participants requiring post-exposure prevention. As ABT requires once biweekly administration due to its extended half-life, poor adherence associated with a three-drug regimen may thus be avoided [27].
It is important to note that, in our study, 55.2% (164/297) participants completed the 12-week follow-up visits. Hence only 73.1% of participants were subjected to HIV antibody testing between Day 15 and Week 12 after the administration of first prophylactic drug. This emphasizes the importance of patient education and effective involvement of the attending doctor in HIV PEP treatment. None of the participants were subsequently found to be infected with HIV.
No serious adverse reactions, injection site reactions, AE, and SAE that could lead to withdrawal from the study were observed in subjects in our study. The most common adverse events and reactions were dizziness, diarrhea, and fatigue of severity grade 1 to 2. The study drugs were well-tolerated. Our results showed that subjects had good overall safety and tolerance to the three regimens.
The challenges associated with the clinical utilization of long-acting drugs are the logistics of distribution and scheduling, relevant costs, and maintenance of the drug at an ideal temperature. Setting up additional clinics, mobile units, home visits, and organizations at community level may help to address these implementation issues. Thus, HIV PEP treatment could become increasingly accessible to participants. In the present study, the 28-day completion rate of oral drugs was 64.0% and the HIV antibody detection rate was 60-70%, suggesting that organizing HIV post-exposure prevention education and awareness programs, drug adherence supervision, and high-risk drug monitoring may effectively improve compliance and ensure better prevention and management of HIV.
The efficacy and safety of an ABT-containing 2-drug combination (ABT+lopinavir/ritonavir) have been demonstrated in randomized clinical trials and post marketing studies [20-23]. With the advantages of long-acting, minimal drug-drug interactions, high barrier to resistance and early blockade of cell fusion mechanism, ABT-containing 2-drug combinations are being considered as a promising HIV PEP option, especially in regions that single-tablet regimens (STR) are not widely available.
The current study had some limitations. Firstly, there were no objective measurements of plasma drug concentration, which would have been able to determine drug compliance more accurately. Secondly, our cohort had a high proportion of participants not presenting for follow-up visits and the high lost-to-follow-up rate observed in our study may have negatively impacted on the regimen completion rate and the individual medication compliance rates seen in our study. The reasons for this are complex and may be related to preservation and maintenance of privacy and confidentiality and may contribute to the unfortunately low PEP follow-up rate in China. And thirdly, our study design was not randomized controlled and selection bias cannot be avoided. Regimen selection was based on participant’s preference, which introduces bias and the results may skew, especially with regards to patient-reported tolerability.
In summary, this study showed ABT-containing regimens (ABT+DTG or ABT+TDF+3TC) offered a good option for HIV PEP due to higher completion rates than the DTG+TDF+3TC regimen. The overall safety was comparable and acceptable among three groups.
Acknowledgement
We are grateful to Vijay Harypursat of the Division of Infectious Diseases at Chongqing Public Health Medical Center for his language editing.
Conflicts of Interest
The authors declare no conflicts of interest.
- Mahy M, Marsh K, Sabin K, Wanyeki I, Daher J, et al. (2019) HIV estimates through 2018: data for decision-making. AIDS (London, England) 33: S203–S211.
- Global HIV & AIDS statistics (2020) fact sheet | UNAIDS
- Qiao YC, Xu Y, Jiang DX, Wang X, Wang F, et al. (2019) Epidemiological analyses of regional and age differences of HIV/AIDS prevalence in China, 2004-2016. Int J infectious dis 81: 215–20.
- Wu ZY, Scott SR (2020) Human immunodeficiency virus prevention strategies in China. Chinese med J 133: 318–25.
- Kouanfack C, Meli H, Cumber SN, Bede F, Nkfusai CN, et al. (2019) Non-Occupational HIV Post-exposure Prophylaxis: A 10-Year Retrospective Review of Data Following Sexual Exposure From Yaounde Central Hospital, Cameroon. Int J MCH and AIDS 8: 138–45.
- Saag MS, Gandhi RT, Hoy JF, Landovitz RJ, Thompson MA, et al. (2020). Antiretroviral Drugs for Treatment and Prevention of HIV Infection in Adults: 2020 Recommendations of the International Antiviral Society-USA Panel. JAMA, 324(16), 1651–1669.
- AIDS and Hepatitis C Professional Group, Society of Infectious Diseases, Chinese Medical Association, & Chinese Center for Disease Control and Prevention (2018). Chinese guidelines for diagnosis and treatment of HIV/AIDS. Chinese J Internal Med 57: 867–84.
- Mayer KH, Mimiaga MJ, Gelman M, Grasso C (2012) Raltegravir, tenofovir DF, and emtricitabine for postexposure prophylaxis to prevent the sexual transmission of HIV: safety, tolerability, and adherence. Journal of acquired immune deficiency syndromes 59: 354–9.
- Milinkovic A, Benn P, Arenas-Pinto A, Brima N, Copas A, et al. (2017) Randomized controlled trial of the tolerability and completion of maraviroc compared with Kaletra® in combination with Truvada® for HIV post-exposure prophylaxis (MiPEP Trial). The J antimicrobial chemotherapy 72: 1760–8.
- Inciarte A, Leal L, González E, León A, Lucero C, et al. (2017) Tenofovir disoproxil fumarate/emtricitabine plus ritonavir-boosted lopinavir or cobicistat-boosted elvitegravir as a single-tablet regimen for HIV post-exposure prophylaxis. J antimicrobial chemotherapy 72: 2857–61.
- Mayer KH, Jones D, Oldenburg C, Jain S, Gelman M, et al. (2017) Optimal HIV Postexposure Prophylaxis Regimen Completion With Single Tablet Daily Elvitegravir/Cobicistat/Tenofovir Disoproxil Fumarate/Emtricitabine Compared With More Frequent Dosing Regimens. Journal of acquired immune deficiency syndromes 75: 535–9.
- Valin N, Fonquernie L, Daguenel A, Campa P, Anthony T, et al. (2016) Evaluation of tolerability with the co-formulation elvitegravir, cobicistat, emtricitabine, and tenofovir disoproxil fumarate for post-HIV exposure prophylaxis. BMC infectious dis 16: 718.
- Whitfield T, Torkington A, van Halsema C (2016) Profile of cabotegravir and its potential in the treatment and prevention of HIV-1 infection: evidence to date. HIV/AIDS (Auckland, N.Z.) 8: 157–64.
- Kovarova M, Swanson MD, Sanchez RI, Baker CE, Steve J, et al. (2016) A long-acting formulation of the integrase inhibitor raltegravir protects humanized BLT mice from repeated high-dose vaginal HIV challenges. The Journal of antimicrobial chemotherapy 71: 1586–96.
- HPTN 083 (2021) Study information.
- HPTN 084 (2021) Study information.
- Chong H, Yao X, Zhang C, Cai L, Cui S, et al. (2012) Biophysical property and broad anti-HIV activity of albuvirtide, a 3-maleimimidopropionic acid-modified peptide fusion inhibitor. PloS one 7: e32599.
- Xie D, Yao C, Wang L, Min W, Xu J, Xiao J, et al. (2010) An albumin-conjugated peptide exhibits potent anti-HIV activity and long in vivo half-life. Antimicrobial agents and chemotherapy 54: 191-6.
- Saag MS (2012) New and investigational antiretroviral drugs for HIV infection: mechanisms of action and early research findings. Topics in antiviral medicine 20: 162–7.
- Su B, Yao C, Zhao QX, Cai WP, Wang M, et al. (2020) Efficacy and safety of the long-acting fusion inhibitor albuvirtide in antiretroviral-experienced adults with human immunodeficiency virus-1: interim analysis of the randomized, controlled, phase 3, non-inferiority TALENT study. Chinese medical J 133: 2919-27.
- Yang J, Wei G, He Y, Hua X, Feng S, Zhao, Y., Chen, T., Wang, H., & Guo, L. (2020). Perioperative Antiretroviral Regimen for HIV/AIDS Patients Who Underwent Abdominal Surgery. World journal of surgery, 44(6), 1790–1797.
- He S, Liu H, Yao Y, et al. (2020). The clinical effect of albuvirtide program in severe AIDS patients. Sichuan Medical Journal, 41: 893-7.
- Feilong Xu (2021) Long-acting HIV fusion inhibitor albuvirtide is a safe and effective treatment in HIV patients with severe liver impairment, HBV co-infection and high HIV RNA copies. J HIV AIDS Infect Dis 8: 1-9.
- Valin N, Fonquernie L, Daguenel A, Campa P, Anthony T, et al. (2016) Evaluation of tolerability with the co-formulation elvitegravir, cobicistat, emtricitabine, and tenofovir disoproxil fumarate for post-HIV exposure prophylaxis. BMC infectious diseases, 16: 718.
- Santa-Bárbara RC, Hueso-Montoro C, Martín-Salvador A, Álvarez-Serrano MA, Gázquez-López M, et al. (2020). Association between Sexual Habits and Sexually Transmitted Infections at a Specialised Centre in Granada (Spain). Int J environ res public health 17: 6881.
- Berruti M, Riccardi N, Canetti D, Lo Caputo S, Taramasso L, Di Biagio A (2021) Injectable Antiretroviral Drugs: Back to the Future. Viruses 13: 228.
- Zhang H, Jin R, Yao C, Zhang T, Wang M, et al. (2016) Combination of long-acting HIV fusion inhibitor albuvirtide and LPV/r showed potent efficacy in HIV-1 patients. AIDS Res therapy 13: 8.
FIGURE 1
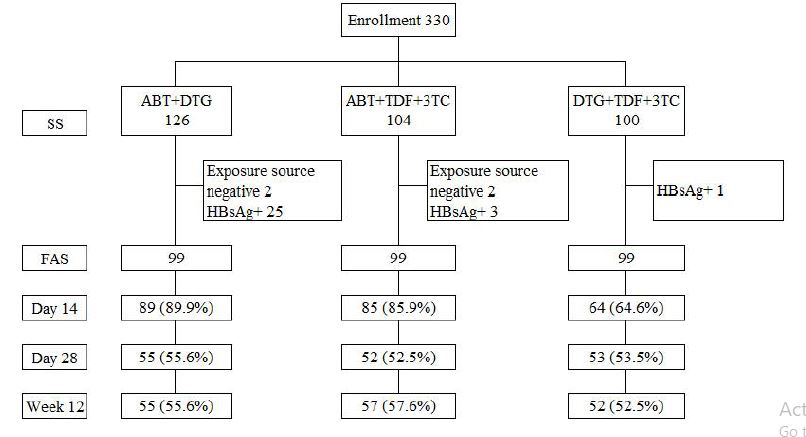
Figure 1: Distribution of subjects in the study
Tables at a glance
Figures at a glance