Delayed Elimination of High-Dose Methotrexate: Risk Factors
Received Date: November 28, 2023Accepted Date: December 28, 2023 Published Date: December 31, 2023
doi: 10.17303/jpdm.2023.6.102
Citation: Bouraoui Hajer, Ben-Fredj Nadia, Ben-Fadhel Najah, Ben-Romdhane Haifa, Slama Nader (2023) Delayed Elimination of High-Dose Methotrexate: Risk Factors. J Pharmacol Drug Metab 6: 1-11
Abstract
Aim: MTX is a folate-inhibitor drug. HD-MTX (dose higher than 500mg/m2) , is specifically indicated in the treatment of leukemia, lymphoma, and osteosarcoma in both adult and pediatric patients. The achievement of optimal MTX exposure and disease remission, on the one hand, and prevention of HD-MTX toxic side effects, on the other hand, are major clinical challenges. The objective of the present study is to identify risk factors of DEM+ in pediatric and adult patients treated with HD-MTX for blood cancer.
Methods: We retrospectively analyzed data from adult and pediatric patients who received intravenous HD-MTX as part of treatment for blood cancer and underwent routine TDM
Results: A total of 395 HD-MTX samples issued from 56 patients (22 F/34 M) were analysed. The number of HD-MTX courses was 195. The median number of MTX dosages per course was two [min:1-max:7]. The cut-off value associated with a risk of DEM+ was 72h. DEM+ (Toxic Cmin after 72h of the start of MTX administration) was observed in 179 of the 395 samples (47.7%), 26 of the 195courses (13.3%) and 17 of the 56 patients (30.3%). The present study have clearly demonstrated that renal impairment, a MTX dose exceeding 2.5g/course and male gender are predictive factors of high-risk of MTX over-exposure. Consequently, these patients should be monitored closely and may require enhanced hydration, urine alkalization, and appropriate leucovorin administration, in order to optimize efficacy and safety of MTX.
Conclusion: Further studies are needed to assess quantitative relationship between MTX exposure and toxic MTX side effects occurrence.
Keywords: Methotrexate; High-Dose; Delayed Elimination; Renal Impairment; Risk Factors
Introduction
Methotrexate (MTX), is a folate inhibitor drug, widely used in rheumatoid arthritis, psoriasis and malignant diseases (1). High-dose methotrexate (HD-MTX), defined as a dose higher than 500 mg/m2 , is specifically indicated in the treatment of leukemia, lymphoma, and osteosarcoma in both adult and pediatric patients [1].
Cytotoxic action of MTX is explained by the inhibition of dihydrofolate reductase production leading to the decrease of the stocks of tetrahydrofolate, required for cell replication and DNA synthesis. This effect is concentration-dependent and mainly observed in rapidly multiplying cells, which explains the effectiveness of HD- MTX in blood cancer [1,2].
However, the effectiveness of HD-MTX could be outweighed by critical organ damage, including myelosuppression, kidney injury, liver disorder, emesis, mucositis and skin lesion, which are reported in 2% to 12% of patients [3,4]. This toxicity can lead in some cases to MTX interruption and switch to other chemotherapy agent more expensive and less effective.
For these reasons, the achievement of optimal MTX exposure and disease remission, on the one hand, and prevention of HD-MTX toxic side effects, on the other hand, are major clinical challenges.
In order to prevent severe toxicity of this drug, urinary alkalinization and hyperhydration protocols are needed to enhance the solubility and dilution of MTX in the urine [5]. Besides, leucovorin (LV) rescue administration; ie calcium folinate derivates, following HD-MTX treatment is mandatory, to prevent tissue damage [3,6]. However, excessive LV rescue may reduce anti-tumoral efficacy of MTX [7]. Therefore, monitoring the serum concentrations of HD-MTX is very useful to define the appropriate dose of LV, and therefore, to optimize the balance between efficacy and adverse events of this drug.
Previous studies have demonstrated that toxic HD-MTX effect are closely related to prolonged exposure to toxic MTX concentrations due to delayed MTX elimination [8-11]. Therefore, risk factors for delayed MTX elimination should be clarified in order to stratify patient’s risk and prevent MTX toxicity.
The objective of the present study is to identify risk factors of delayed MTX elimination (DEM+) in pediatric and adult patients treated with HD-MTX for blood cancer.
Patients and Methods
Patients and Data CollectionWe retrospectively analyzed data from adult and pediatric patients who received intravenous HD-MTX as part of treatment for blood cancer and underwent routine therapeutic drug monitoring (TDM).
These data were collected from May 2008 to December 2021 from the TDM digital database of the Pharmacology Department of Monastir (Tunisia).
For each patient, the following parameters were recorded: age, gender, weight, serum creatinine clearance (CrCl), MTX-HD dose, indication MTX-HD regimen, drug infusion time, and needed dose of LV following HD-MTX treatment.
CrCl was calculated using the Cockcroft and Gault equation. Renal function was analyzed as binary variables: patients with renal impairment if CrCl is < 80 mL/min, and those with normal renal function if CrCl is>80 mL/min.
HD-MTX RegimenHD-MTX treatment regimen was different according to the indication and patient’s age. For acute lymphoblastic leukemia (ALL) and non-Hodgkin’s lymphoma in childhood, HD-MTX was administered at a dose of 5 g/m² for 24 hours, according to European Organization for Research and Treatment of Cancer (EORTC) recommendations [12]. For ALL in adults, the Group for Research on Adult Acute Lymphoblastic Leukemia (GRAALL) protocol was applied; i.e. MTX was administered during consolidation phase, at a dose of 3 g/m2 during a 24-hour infusion [13]. Regarding treatment of childhood mature B-cell lymphoma and leukemia, MTX was administered at a dose of 8 g/m² during a 24-hour infusion in case of patients experiencing a central nervous system disturbance, and 3 g/m² during a 3-hour infusion in case of absence of central nervous system localization [12].
LV rescue began 24 hours after the MTX infusion, starting at a dose of 15 mg/m²/6h in case of childhood mature B-cell lymphoma and leukemia. This supportive treatment was introduced 36 hours after the start of the MTX infusion at a dose of 12 mg/m2 /6 h in the case of ALL and non-Hodgkin’s lymphoma in both childhood and adult patients.
MTX levels were closely monitored every 24 hours. LV was maintained until MTX serum level fell below nontoxic serum levels.
Determination of MTX Serum ConcentrationVenous blood samples were collected into tubes containing EDTA, and then the plasma was separated. Blood samples for the determination of MTX concentration were taken at 24, 48 and 72 hours after starting HD-MTX infusion. For patients with a 72-h plasma MTX concentration above 0.2 and 0.15 μmol/l, monitoring was continued every 24 hours until the plasma MTX concentrations fell below these values, in cases of 24 and 3 hours MTX infusion time, respectively.
MTX concentrations were determined using an enzyme multiplied immunoassay technique (V-Twin System, Siemens Healthcare Diagnostics). Blood samples exceeding the upper limit of the calibration range were diluted according to the manufacturer’s protocol.
Statistical Analysis
The statistical analysis was performed using MedCalc (Version 20.218). The normality of data was assessed using a Shapiro-Wilk test. Continuous variables were expressed as mean ± standard deviation if data were normally distributed and as median and range, otherwise.
For categorical data, number and percentage were provided.
Receiver operating characteristic (ROC) curve analysis was performed to define the threshold of the MTX delayed elimination. Accordingly, we classified the patients into two groups:
Delayed MTX Elimination (DEM+): patients having a toxic CMTX after the time threshold defined by ROC curve.
Non-Delayed MTX Elimination (DEM-): patients having a CMTX less than toxic value after time threshold defined by ROC curve.
To assess risk factors associated with delayed MTX elimination, a univariate analysis was performed separately for each tested factor (age, weight, gender, renal impairment, MTX dose, MTX infusion time). Differences in proportions for independent data were assessed by the χ2-test. Comparison of continuous data was performed by Student t-test for normally distributed data. Wilcoxon and Mann-Whitney U tests were applied to compare non- normal data for dependent and independent continuous variables, respectively. After evaluation of the distribution of continuous data, parametric tests were applied for normally distributed variables and non-parametric tests were applied otherwise.
All variables having a p-value < 0.20 in the univariate analyses were included in the multivariate analysis model. Actually, a logistic regression was performed to define independent risk factor for DEM+. A p-value less than 0.05 was considered as statistically significant.
Results
A total of 395 HD-MTX samples issued from 56 patients (22 Females / 34 Males) were analysed. The patient’s median age was 8.5 y [1 y- 72 y]. Among them, 37 (66.1%) were children and 19 (33.9%) were adults.
The number of HD-MTX courses was 194. The median number of MTX dosages per course was two [min: 1-max: 7].
Indications of HD-MTD were acute lymphoblastic leukaemia (31 patients (55.3%)), non-Hodgkin’s lymphoma (21 patients (37.5%)), lymphoblastic lymphoma T (1 patient (0.17%)), lymphoblastic lymphoma B (1 patient (0.17%)), osteosarcoma (1 patient (0.17%)), and cutaneous lymphoma (n=1 patient (0.17%)). The demographic and clinical parameters of these patients are summarized in Table 1.
ROC analysis of MTX time concentration (introduced as binary variable: Cmin toxic/Cmin non-toxic), has shown a significant AUC level of 0.71 (P < 0.001). The cutoff value associated with a risk of DEM+ was 72 h; i.e., persistence of toxic MTX Cmin; was ≥72 h (sensitivity: 69.0 %; specificity: 69.5 %). (Figure 1)
DEM+ MTX (Toxic Cmin after 72 h of the start of MTX administration) was observed in 179 of the 395 samples (47.7%), 26 of the 194 courses (13.4%) and 17 of the 56 patients (30.3%).
The univariate analysis showed that weight, gender, MTX dose, MTX infusion time, renal impairment and course number were found to be risk factors for DEM+ (Table 2).
The multivariate analysis showed that gender, MTX dose and renal impairment remains independent risk factors of DEM+ (Table 2). Patients with renal dysfunction were found to have 5.9 higher risk of DEM+ than those with normal renal function.
Besides, the cut-off value of dose associated with DEM+ risk was > 2.5 g/course (OR: 4.82; p: 0.001, 95 % CI: [2.24-9.15]) (Figure 2 & 3).
Discussion
In the present study, renal impairment, MTX dose and male gender were found to be independent risk factors for DEM in patients treated with HD-MTX. These findings are of a clinical importance as they identify patients at a high risk for severe toxic effects, particularly bone marrow suppression, oral mucositis and nephrotoxicity, in order to plan adequate supportive care to prevent such effects in these patients [1,8,15].
HD-MTX is the cornerstone in the treatment of ALL and non-Hodgkin’s lymphoma. This chemotherapy was introduced early since 1948, and has proven its effectiveness in these indications [1,7]. This agent inhibits the production of dihydrofolate reductase and decreases the production of purine nucleotides and thymidylate, which are both required for cell replication and DNA synthesis [2]. The pharmacokinetic of MTX is characterized by a wide intra-individual variability, thus TDM is mandatory to define LV dose and time for patient’s hospital discharge [4,11,16]. This approach could optimize the balance risk–benefit and particularly reduce toxicity of MTX, which could increase adherence and decrease mortality.
In our study, the time to achieve nontoxic MTX concentration was found to be 72 h after starting MTX infusion, as demonstrated by the ROC curve. This result is in ac-cordance with previous data considering that normal MTX elimination is defined as a CMTX-72h less than 0.15µmol/L, which is associated with optimal MTX exposure and lower incidence of MTX toxic side effects [16,17]. In this context, Cheng et al. showed that children with a 66h-MTX concentration higher than 0.2 µmol/l have a 8.2-fold increased risk of developing oral mucositis when compared with those having a 66-h MTX concentration lower than 0.2µmol/l [18]. Moreover, Xu et al. demonstrated that thrombocytopenia was significantly higher in patients with DEM+ [19]. This lets us suppose that 72 h is the time matching with LV rescue withdrawal and patient’s hospital discharge.
In the present cohort, a DEM+ was found in 13.3% of MTX courses, which is quite similar to frequencies reported previously [15,17,20]. For example, Nakano et al. found that DEM+ was observed in 7.8% of HD-MTX courses administered to 88 children with ALL or non-Hodgkin’s lymphoma. This indicates that this group was overexposed to MTX, which could result in life-threatening toxicity such as myelosuppression, digestive complications, acute hepatitis and acute kidney injuries, as have been shown in previous publications [3,8,18,20].
In order to prevent HD-MTX toxic side effects, numerous previous reports have focused on identification of DEM+ risk factors based on case-control studies. In this respect, several factors have been identified such as hypoalbuminemia, high plasma amount of bilirubin and drug interactions [21,22]. Regarding the MTX dose, most of previous studies focusing on ALL in children have shown that DEM+ is strongly associated with HD-MTX [15]. For instance, Nakano et al. showed that doses higher than 3g/course increased 10.8-fold the risk of DEM+, which is in alignment with our results [15,19]. We have indeed identified, based on ROC analysis, a cut-off level of MTX dose of at least 2.5 g/course; i.e., a patient receiving a dose higher than 2.5 g have almost 5-fold risk of DEM+, compared with lower doses. However, this cut-off dose is slightly lower than those reported previously, as approximately one-third of our patients were adults and required lower doses of MTX than those required in children
Moreover, limited data have assessed the impact of infusion time on DEM. In this respect, Woessmann et al. found that long infusion duration is a risk factor for DEM+ as a 24-hour infusion time allowed the achievement of higher MTX exposure compared with 3-hour infusion [8]. However, this hypothesis has not been supported by other studies. For instance, Reeves et al. [23] and Xu et al. [19], showed that the prolonged administration (24-hour infusion) did not increase the MTX elimination delay as compared with short infusion time (3-hour administration), as ours.
Besides, our results showed that males were twice more exposed to develop DEM+ than females. The relationship between gender and pharmacokinetic parameters or delayed excretion of MTX has been investigated in few studies with controversial results [6,22,24]. In this context, Zhang et al. did not find any significant difference of MTX DEM incidence between males and females (5.24% vs 7.89%; p = 0.059) [6]. In contrast, Liang et al. have shown that a DEM+ was 4.2-more frequent in male than in female receiving HD-MTX, which is consistent with our findings (24). Similarly, Wiczer et al. demonstrated that males have a 2.3-higher risk of nephrotoxicity, and then of DEM+ as compared with females [22].
Interestingly, renal impairment was identified as the major risk factor for DEM+ in our cohort, as patients with a CrCl ≤ 80 ml/min have a 5.9-fold risk to have a DEM+ than patients having a normal renal function. This finding is consistent with previous reports which demonstrated that DEM+ MTX were closely related to a decrease in CrCl, as more than 90% of MTX is eliminated by kidneys [3,25-27]. This could result in the accumulation of MTX and an increased risk for additional toxic side effects; such as myelosuppression, mucositis, hepatotoxicity, and, in severe cases, multi-organ failure. Thus, regular MTX concentration monitoring, increased hydration and high-dose LV are mandatory to enhance MTX excretion in patients with renal impairment and to allow administer ring subsequent HD-MTX courses.
Our study has several limitations. First, LV administered dose and associated chemotherapy were not mentioned in all patient’s records. Second, some clinical (digestives symptomatology, mucosal and cutaneous affection..) and biological parameters (albuminemia , liver enzymes) related to MTX toxic side effects were requested in patient’s information form, however clinicians do not usually precise them.
In conclusion, the present study have clearly demonstrated that renal impairment, a MTX dose exceeding 2.5 g/course and male gender are predictive factors of high- -risk of MTX over-exposure. Consequently, these patients should be monitored closely and may require enhanced hydration, urine alkalization, and appropriate LV administration, in order to optimize efficacy and safety of MTX. Further studies are needed to assess quantitative relationship between MTX exposure and toxic MTX side effects occurrence.
Declarations
Ethical Approval
Not Applicable. Indeed, this study analyses data obtained in our routine activity.
Competing Interests
No conflict of interest
Authors' Contributions
Hajer Bouraoui prepared data files. Hajer Bouraoui and Nadia Ben Fredj wrote the main manuscript and prepared figures and tables. Najah Ben-Fadhel performed statistical analysis. All authors reviewed the manuscript.
Funding
No Funding
Availability of Data and Materials
Not Applicable
- Hamed KM, Dighriri IM, Baomar AF, Alharthy BT, Alenazi FE, Alali GH, et al. (2022) Overview of Methotrexate Toxicity: A Comprehensive Literature Review. Cureus 14: e29518.
- Cronstein BN, Aune TM (2020) Methotrexate and its mechanisms of action in inflammatory arthritis. Nat Rev Rheumatol. Mars 16: 145‑54.
- Howard SC, McCormick J, Pui CH, Buddington RK, Harvey RD (2016) Preventing and Managing Toxicities of High-Dose Methotrexate. The Oncologist 21: 1471‑82.
- Traivaree C, Likasitthananon N, Monsereenusorn C, Rujkijyanont P (2018) The effect of intravenous hydration strategy on plasma methotrexate clearance during intravenous high-dose methotrexate administration in pediatric oncology patients. Cancer Manag Res 10: 4471‑8.
- Zhang W, Zhang Q, Zheng TT, Zhen JC, Niu XH (2016) Delayed High-dose Methotrexate Excretion and Influencing Factors in Osteosarcoma Patients. Chin Med J (Engl) 129: 2530‑4.
- Mikkelsen TS, Sparreboom A, Cheng C, Zhou Y, Boyett JM, Raimondi SC, et al. (2011) Shortening infusion time for high-dose methotrexate alters antileukemic effects: a randomized prospective clinical trial. J Clin Oncol Off J Am Soc Clin Oncol 29: 1771‑8.
- Woessmann W, Seidemann K, Mann G, Zimmermann M, Burkhardt B, Oschlies I, et al. (2005) The impact of the methotrexate administration schedule and dose in the treatment of children and adolescents with B-cell neoplasms: a report of the BFM Group Study NHL-BFM95. Blood 105: 948‑58.
- Misaka KO, Suga Y, Staub Y, Tsubata A, Shimada T, Sai Y, et al. (2020) Risk Factors for Delayed Elimination of Methotrexate in Children, Adolescents and Young Adults With Osteosarcoma. Vivo Athens Greece 34: 3459‑65.
- Xu W, Tang Y, Song H, Shi S, Yang S (2007) Retrospective study on elimination delay of methotrexate in high-- dose therapy of childhood acute lymphoblastic leukemia in China. J Pediatr Hematol Oncol 29: 688‑93.
- Li X, Sui Z, Jing F, Xu W, Li X, Guo Q, et al. (2019) Identifying risk factors for high-dose methotrexate-induced toxicities in children with acute lymphoblastic leukemia. Cancer Manag Res 11: 6265‑74.
- Olivier-Gougenheim L, Arfeuille C, Suciu S, Sirvent N, Plat G, Ferster A, et al. (2020) Pediatric randomized trial EORTC CLG 58951: Outcome for adolescent population with acute lymphoblastic leukemia. Hematol Oncol 38: 763‑72.
- Ben Abdelali R, Asnafi V, Leguay T, Boissel N, Buzyn A, Chevallier P, et al. (2011) Pediatric-inspired intensified therapy of adult T-ALL reveals the favorable outcome of NOTCH1/FBXW7 mutations, but not of low ERG/BAALC expression: a GRAALL study. Blood 118: 5099‑107.
- Cohen Gogo S, Landman-Parker J, Bertrand Y, Nelken B, Schmitt C, Lutz P, et al. (2008) SFCE-P19 – Cancérologie – Lymphome de Burkitt après transplantation d’organe en pédiatrie. Arch Pédiatrie 15: 1012.
- Nakano T, Kobayashi R, Matsushima S, Hori D, Yanagi M, Suzuki D, et al. (2021) Risk factors for delayed elimination of high-dose methotrexate in childhood acute lymphoblastic leukemia and lymphoma. Int J Hematol. Mai 113: 744‑50.
- Ranchon F, Vantard N, Henin E, Bachy E, Sarkozy C, Karlin L, et al. (2018) Delayed methotrexate elimination: Incidence, interaction with antacid drugs, and clinical consequences? Hematol Oncol. Avr 36: 399‑406.
- Santucci R, Levêque D, Lescoute A, Kemmel V, Herbrecht R (2010) Delayed elimination of methotrexate associated with co-administration of proton pump inhibitors. Anticancer Res. 30: 3807‑10.
- Cheng KKF (2008) Association of plasma methotrexate, neutropenia, hepatic dysfunction, nausea/vomiting and oral mucositis in children with cancer. Eur J Cancer Care (Engl). Mai 17: 306‑11.
- Xu W, Tang Y, Song H, Shi S, Yang S (2007) Retrospective study on elimination delay of methotrexate in high-- dose therapy of childhood acute lymphoblastic leukemia in China. J Pediatr Hematol Oncol. 29: 688‑93.
- Blasco H, Silly S, Tournamille JF, Gyan E, Sénécal D, André V, et al. (2008) [Not Available]. Therapie 63: 19‑28.
- Reiss SN, Buie LW, Adel N, Goldman DA, Devlin SM, Douer D (2016) Hypoalbuminemia is significantly associated with increased clearance time of high dose methotrexate in patients being treated for lymphoma or leukemia. Ann Hematol. 95: 2009‑15.
- Wiczer T, Dotson E, Tuten A, Phillips G, Maddocks K (2016) Evaluation of incidence and risk factors for high-- dose methotrexate-induced nephrotoxicity. J Oncol Pharm Pract Off Publ Int Soc Oncol Pharm Pract 22: 430‑6.
- Reeves DJ, Moore ES, Bascom D, Rensing B (2014) Retrospective evaluation of methotrexate elimination when co-administered with proton pump inhibitors. Br J Clin Pharmacol 78: 565‑71.
- Liang CA, Su YC, Lin SJ, Tsai TH (2023) Risk factors for acute kidney injury after high-dose methotrexate therapy: a single-center study and narrative review. Eur J Clin Pharmacol 79: 789‑800.
- Kawaguchi S, Fujiwara SI, Murahashi R, Nakashima H, Matsuoka S, Ikeda T, et al. (2021) Risk factors for high-- dose methotrexate-induced nephrotoxicity. Int J Hematol 114: 79‑84.
- Yang SL, Zhao FY, Song H, Shen DY, Xu XJ (2015) Methotrexate Associated Renal Impairment Is Related to Delayed Elimination of High-Dose Methotrexate. Sci World J 2015: e751703.
- Garcia H, Leblond V, Goldwasser F, Bouscary D, Raffoux E, Boissel N, et al. (2018) [Renal toxicity of high-dose methotrexate]. Nephrol Ther. Avr 14: S103‑13.
FIGURE 1
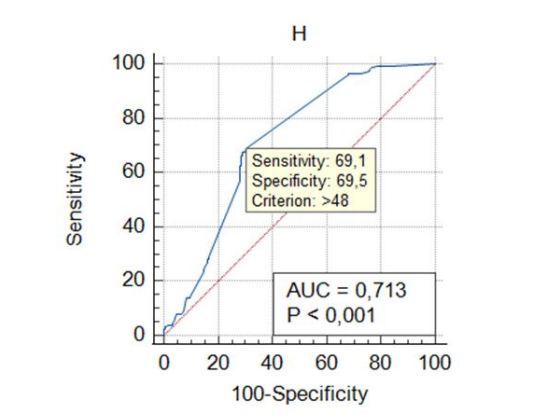
Figure 1: Receiver operating characteristic (ROC) curve analysis of delayed elimination in patients receiving HD-MTX
FIGURE 2
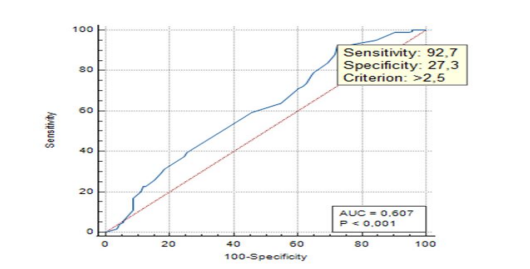
Figure 2: ROC curve analysis of MTX doses associated with delayed elimination
FIGURE 3
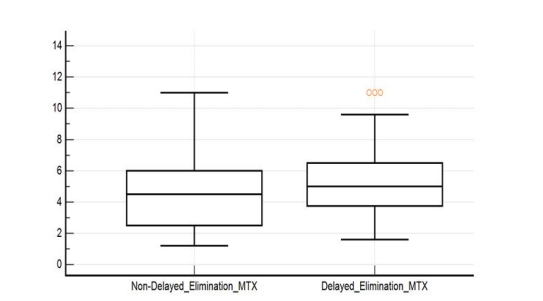
Figure 3: Comparaison of doses between patients with delayed and non- delayed elimination MTX
Tables at a glance
Figures at a glance