Lemmel Syndrome: An Unusual Case of Periampullary Duodenal Diverticula with Cholelithiasis
Received Date: October 20, 2024 Accepted Date: November 20, 2024 Published Date: November 22, 2023
doi: 10.17303/jrnm.2024.1.105
Citation:Prateek Bommu, Sumit Kumar, Arya Agnihotri, Saurav Bhagat, Vishal Gupta et al. (2024) Lemmel syndrome: An unusual case of periampullary duodenal diverticula with cholelithiasis. J Radiol Nucl Med 1: 1-8
Abstract
Lemmel syndrome is a rare condition caused by a periampullary duodenal diverticulum (PAD) compressing the intrapancreatic common bile duct and characterized by obstructive jaundice. PAD are outpouchings of the duodenum near the ampulla of vater, where the pancreatic duct and bile duct enter the duodenum. The prevalence of PAD has been reported to be as high as 65% in the elderly population. They are usually asymptomatic, but they may cause complications such as diverticulitis, cholangitis, pancreatitis, perforation, or hemorrhage. The diagnosis of Lemmel syndrome can be made by different imaging techniques, such as barium studies, ERCP, computed tomography, or magnetic resonance cholangiopancreatography. The treatment of Lemmel syndrome depends on the severity of the symptoms and the underlying cause of the diverticulum. Surgical or endoscopic interventions may be required to relieve the biliary obstruction and prevent further complications. We here report a case of a 50-year-old female patient who presented with fever, intermittent diarrhea, and upper abdominal pain for 2 months. Her laboratory report revealed raised TLC along with higher bilirubin levels. An initial ultrasound revealed two well-defined anechoic round-to-oval lesions adjacent to the duodenum with dirty air shadowing and a dilated common bile duct. We ordered CT of the upper abdomen with oral contrast and MRCP, which revealed two periampullary diverticula compressing the distal common bile duct.
Keywords:Periampullary Duodenal Diverticula; Lemmel Syndrome; Upper Abdominal Pain; Icterus; Computed Tomography; MRCP; Common Bile Duct; Cholelithiasis
Introduction
In 1710, Pierre Jean Baptiste Chomel, a French pathologist, provided the first description of a duodenal diverticulum comprising 22 calculi, probably of biliary origin [1,2]. Baldwin was the first to observe a common bile duct (CBD) emptying into a duodenal diverticulum in five autopsies [3]. In 1934, Lemmel was the first to propose a relationship between duodenal diverticula and pancreaticobiliary disease when he identified two symptom complexes that he considered indicative of but not unique to the periampullary diverticulum (PAD). He described an association between PAD and the onset of liver and bile duct disease, as well as damage to the pancreas and pancreatogenic diarrhea, and created the term 'papillen syndrom' [4]. Diverticula arising within a 2-3 cm radius of the ampulla but not containing it are referred to as “juxta papillary diverticula”. They do not normally cause symptoms on their own [5]. In the setting of Lemmel syndrome, periampullary diverticula without choledocholithiasis can cause obstructive jaundice [6]. The role of cross-sectional imaging in illustrating acute or subacute abdominal conditions as well as the acute abdomen caused by common intra-abdominal pathology have both been extensively covered in the medical literature, but the role of imaging in the diagnosis of symptomatic duodenal diverticula are underreported, primarily because there are no specific pathognomonic symptoms and signs. The prevalence of PAD has been reported to be as high as 65% in the elderly population [7]. The pathogenesis of PAD in particular may involve herniations of mucosa through mural weak points, presumably at sites where the common bile duct and pancreatic duct enter the submucosa. Multiple colonic diverticula may also coexist in up to 30% of patients [8].
Several unusual mechanisms have been proposed as possible etiopathological factors for Lemmel syndrome. First, direct mechanical irritation or diverticulitis of the PAD leads to chronic ampullary inflammation which can lead to chronic fibrosis of the papilla (papillitis chronica fi- brosa) [9]. Second, the PAD may cause dysfunction of the sphincter of Oddi [10]. Third, the distal common bile duct or ampulla may be directly compressed by a PAD, which is distended by enteroliths or foreign bodies, thereby obstructing the passage of bile into the bile duct or hepatic duct, causing cholestasis, jaundice, gallstones, cholangitis, and pancreatitis [4,11]. PAD usually manifests as an outpouching of the mucosa and muscularis mucosae, caused either by progressive weakening of intestinal smooth muscle or increased intraduodenal pressure [12].
On CT or MRI, PAD often appears as a thinwalled, rounded mass with fluid collection in the periampullary region along the medial border, containing air and/or fluid or oral contrast. Lack of either oral contrast or gas within these lesions makes it difficult to distinguish from cystic pancreatic masses, and further evaluation with an upper gastrointestinal barium study may prove diagnostic [13]. PAD may cause complications such as diverticulitis, cholangitis, pancreatitis, perforation, or hemorrhage. The risk of complications such as perforation of the PAD can lead to severe life-threatening peritonitis and may require urgent surgical intervention [2]. Lemmel syndrome should be considered as a differential diagnosis in patients presenting with acute abdominal pain and/or obstructive jaundice, even though it is a rare cause. A high index of suspicion is required for a timely accurate diagnosis of Lemmel syndrome, as signs and symptoms are often similar to other intra-abdominal processes, and cases that are undiagnosed can lead to further complications. It may be challenging to diagnose Lemmel syndrome, but it is also essential for avoiding improper treatment. The detection of PAD is the preliminary step in the process of diagnosis.
Case History
A 50-year-old Indian female presented to the Department of Surgery with chief complaints of fever, nausea, intermittent diarrhea, and upper abdominal pain for 2 months. The fever started initially with continuous high-- grade fever which ran for a few days followed by an intermittent low-grade fever over a period of a month which was controlled with over-the-counter antipyretics. There was slow onset mild right upper quadrant abdominal pain and discomfort which progressed to moderately severe pain associated with nausea after a few days. Over-the-counter drugs temporarily alleviated these symptoms, but they persisted. She was diagnosed with type 2 diabetes 6 years earlier, which is under control. Her current medication includes metformin twice daily. The rest of her history was unremarkable.
On physical examination, the patient is overweight with a body mass index of 28.9 kg/m2. She had right upper quadrant discomfort and icterus, and her vitals were stable. Laboratory tests revealed an increased total leukocyte count of 250000/dL (normal range, 4000-10000/ dL), an increased C-reactive protein level of 120 mg/L (normal range, 0.2-0.9 mg/L), and an obstructive pattern on liver function tests, with a total bilirubin level of 3 mg/dL (normal range, 0.4-1.9 mg/dL), an alkaline phosphatase level of 250 U/L (normal range, 39-99 U/L), and an aspartate aminotransferase level of 120 U/L (normal range, 12–42 U/L). The elevated lab values such as total leukocyte count and C-reactive protein, raised the suspicion of infective or in ammatory etiology. e elevated bilirubin, alkaline phosphatase, and aspartate aminotransferase which all indicated cholestasis leading to obstructive jaundice.
An abdominal radiograph showed a nonspecific bowel gas pattern with no signs of bowel obstruction and no free air under the diaphragm. An ultrasound, along with NCCT upper abdomen (with oral contrast) and MRCP, was performed for further evaluation.
Imaging Findings
Ultrasound, MRCP, and computed tomography of the upper abdomen with oral contrast were performed on this patient.
An ultrasound examination showed multiple echogenic calculi in the gall bladder lumen and neck. Ultrasound reveals two well-defined anechoic round-to-ovoid lesions with gas shadows adjacent to the duodenum and abutting the distal common bile duct. The common bile duct showed proximal dilatation and tapered distally. However, no calculus could be traced in the common bile duct. The pancreas was normal in size, shape, and echogenicity. No mass could be traced at the pancreatic head. These findings raised the suspicion of duodenal pathology causing compression over the common bile duct.
The patient had a slightly raised serum creatine level; hence, intravenous iodine-based contrast was avoided and only oral gastrograffin was administered.So, we performed Computed tomography of the upper abdomen with oral contrast. It revealed two duodenal diverticula of varying sizes (the largest one being 28 mm in diameter and the smaller one being 14 mm in diameter) in the periampullary region containing an air-fluid level and oral contrast material, as shown in (Figure 1). It was observed to be obstructing the distal common bile duct, resulting in a moderate degree of proximal biliary ductal dilatation. No other periampullary pathology was observed.
MRCP showed multiple T2-weighted SPAIR hypointense filling defects in the gall bladder lumen with moderate dilation of the common bile duct and sudden narrowing of the distal common bile duct. No calculus was seen in the common bile duct. These findings also correlate with the suspicion of a periampullary pathology. The axial and coronal images revealed two periampullary diverticula of varying sizes surrounding the common bile duct, causing extrinsic compression of the distal common bile duct with a luminal diameter of 2.8 mm at this level. We observed proximal dilatation of the common bile duct along with mild to moderate intrahepatic biliary radical dilatation. No calculi were seen in the common bile duct. Incidentally, we found a large staghorn calculus in the renal pelvis, which caused gross hydronephrosis of the right kidney (Figure 2 and Figure 3).
During the hospitalization, the surgical team inserted a nasogastric tube for decompression and suction with lavage. She was managed with intravenous analgesics followed by a course of intravenous ceftriaxone. No evidence of a systemic inflammatory response was identified; moreover, adequate evolution ensued. A laparoscopic cholecystectomy with transduodenal diverticulectomy was also proposed by the surgical gastroenterology department, which was further refused by the patient. The patient was followed up after two months as she improved clinically, and the laboratory values revealed normalization of the previously elevated liver function test values and other inflammatory markers.
Discussion
Periampullary duodenal diverticula typically occur along the medial aspect of the second or third part of the duodenum and are commonly recognized as an incidental finding in cross-sectional imaging [13]. They are rarely symptomatic, and complications occur in less than 5% of cases, which include bleeding, perforation, cholangitis, pancreatitis, bezoar or enterolith formation, and obstructive jaundice [14]. The majority of these diverticula are diagnosed incidentally and are asymptomatic, but at times, pancreaticobiliary and/or non-pancreaticobiliary complications may occur.
A significant number of cases have been reported in recent years in Asia and Europe of periampullary diverticula. In these patients, the prevalent complaint continues to be acute recurrent abdominal pain in the epigastrium or hypogastrium, nausea, vomiting, fatigue, and unintentional weight loss. In 2018, Frauenfelder et al. reported two female patients with Lemmel syndrome who both presented with pain in the epigastrium and elevated bilirubin. In one of the patients, CT with oral contrast revealed a small periampullary duodenal diverticulum with an air-fluid level adjacent to the distal part of the CBD [15]. In 2016, a similar case of PAD was reported in the United States in a young female who suffered from unintentional weight loss and fatigue for three months. They performed contrast-enhanced computed tomography (CT), which revealed a large PAD with mucosal enhancement and fat stranding consistent with diverticulitis. However, the bilirubin values were in the normal range, and she was managed conservatively [6]. In our case, it was a female patient who presented with upper abdominal pain and high bilirubin values. Using CT with oral contrast and MRCP, we found two periampullary diverticula compressing the distal CBD.
When a biliary obstruction is present, excision of the diverticulum can be done, but the procedure is difficult and associated with significant mortality [16]. Various management options exist, ranging from endoscopic extraction of entrapped material and extracorporeal shock wave lithotripsy to laparoscopic diverticulectomy. Duodenectomy, Diverticulum resection, and Roux en Y hepaticojejunostomy with or without duodenojejunostomy have been reported as surgical interventions in some cases [17,18]. In certain clinical scenarios, the surgical excision of the diverticulum is indicated. When there is a biliary obstruction, the diverticulum can be excised, but the surgical procedure is difficult and has a significant mortality [18]. Conservative treatment includes nasogastric decompression and broad- -spectrum antibiotics in case of perforation. Therefore, duodenal diverticula are usually not treated unless there are complications. If conservative treatments fail, transduodenal diverticulectomy is often performed [16]. Some authors prefer treatment options such as ERCP with sphincterotomy and biliary stent placement which are associated with a reduced risk of morbidity and mortality [11]. Few authors recommend only conservative treatment with bezoar extraction in cases where food is impacted in the diverticulum [19].
Love et al.'s current literature state that 88.2 percent of cases had mentioned the treatment and outcomes. In those cases, the presenting illness did not result in any long-term complications or deaths. 67 percent of patients had IV antibiotic treatment, and 70 percent of these cases had fever as a presenting symptom; twenty percent of cases were afebrile, and one case did not specify whether fever was present or absent. In 46.7 percent of these patients, endoscopic intervention-such as diverticular lavage, pancreaticobiliary stent implantation, or sphincterotomy—was carried out and proved to be an effective treatment [20]. Our patient had shown improvement with nasogastric tube decompression with suction and lavage followed by a course of antibiotics and antipyretics/analgesics. The laboratory values revealed normalization of the previously elevated liver function test values and other inflammatory markers.
An important consideration is that not all forms of Lemmel syndrome can be attributed to extrinsic compression of the common bile duct by periampullary diverticula. Depending on the underlying etiopathogenesis, the treatment modality may vary.
Conclusion
Lemmel syndrome is a rare cause of obstructive jaundice and should be included in the differential diagnosis of biliary obstruction. The role of imaging in the diagnosis of Lemmel syndrome is critically underreported due to the absence of specific pathognomonic symptoms and signs. An awareness of the condition and a high index of suspicion is required to establish an accurate diagnosis, as Lemmel syndrome can mimic several benign and malignant pathologies in the periampullary region.
Acknowledgment
I thank the following individuals for their expertise and assistance throughout all aspects of our study and for their help in writing the manuscript.
I would like to express my deep gratitude to Assistant Professor Dr Saurav Bhagat my research supervisor, for his patient guidance, enthusiastic encouragement, finding out the diagnosis, and useful critiques of this research work. I am particularly grateful for the assistance given by Dr. Sumit Kumar in manuscript writing, editing, and keeping my progress on schedule. I wish to acknowledge the help provided by Dr. Arya Agnihotri in organizing the patient clinical and laboratory data and also the case imaging data. Dr. Fathima Febin Salu and Dr. Saurabh Pandey provided me with very valuable information in writing the manuscript and factual review.
I would also like to extend my thanks to the technicians of the laboratory of the Radiology department for their help in offering me the resources to write the manuscript for the case report.
Conflict of Interest Statement
In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work.
Funding
All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work.
- Lotveit T, Skar V, Osnes M (1988) Juxtapapillary duodenal diverticula. Endoscopy 1: 175-8.
- Thorson CM, Paz Ruiz PSP, Roeder RA, Sleeman D, Casillas VJ (2012) The perforated duodenal diverticulum. Arch Surg 147: 81-8.
- Baldwin WM (1911) Duodenal diverticula in man. Anat Rec 5: 121-40.
- Lemmel G (1934) Die Klinishe Bedeutung der duodenal divertikel. Arch Verdauungskrht 46: 59-70.
- Lobo DN, Balfour TW, Iftikhar SY, Rowlands BJ (1999) Periampullary diverticula and pancreaticobiliary disease. Br J Surg 86: 588-97.
- Desai K, Wermers JD, Beteselassie N (2017) Lemmel syndrome secondary to duodenal diverticulitis: A case report. Cureus 9: e1066.
- Khan BA, Khan SH, Sharma A (2017) Lemmel’s syndrome: A rare cause of obstructive jaundice secondary to periampullary diverticulum. Eur J Case Rep Intern Med 4: 000632.
- Kua JE, Seah A, So JB (2005) Periampullary diverticulum: a case of bleeding from a periampullary diverticulum. Ann Acad Med Singap 34: 636-8.
- Manabe T, Yu GS (1977) Duodenal diverticulum causing intermittent- persistent cholestasis. Associated with papillitis chronica fibrosa. N Y State J Med 77: 2132-6.
- Tomita R, Tanjoh K (1998) Endoscopic manometry of the sphincter of Oddi in patients with Lemmel’s syndrome. Surg Today 28: 258-61.
- Rouet J, Gaujoux S, Ronot M, Palazzo M, Cauchy F, Vilgrain V, et al. (2012) Lemmel’s syndrome as a rare cause of obstructive jaundice. Clin Res Hepatol Gastroenterol 36: 628-31.
- Rizwan MM, Singh H, Chandar V, Zulfiqar M, Singh V (2011) Duodenal diverticulum and associated pancreatitis: case report with brief review of literature. World J Gastrointest Endosc 3: 62-3.
- Macari M, Lazarus D, Israel G, Megibow A (2003) Duodenal diverticula mimicking cystic neoplasms of the pancreas: CT and MR imaging findings in seven patients. AJR Am J Roentgenol 180: 195-9.
- Figueroa-Rivera I, Class-Vazquez W, Martin J (2017) Lemmel’s syndrome: A rare phenomenon causing obstructive jaundice: 1330. Official journal of the American College of gastroenterology ACG 112: 722-3.
- Frauenfelder G, Maraziti A, Ciccone V, Maraziti G, Caleo O, Giurazza F, et al. (2019) Computed tomography imaging in Lemmel syndrome: A report of two cases. J Clin Imaging Sci 9: 23.
- Karayiannakis AJ, Bolanaki H, Courcoutsakis N, Kouklakis G, Moustafa E, Prassopoulos P, et al. (2012) Common bile duct obstruction secondary to a periampullary diverticulum. Case Rep Gastroenterol 6: 523-9.
- Yoneyama F, Miyata K, Ohta H, Takeuchi E, Yamada T, Kobayashi Y (2004) Excision of a juxtapapillary duodenal diverticulum causing biliary obstruction: report of three cases. J Hepato-Bil Pancreat Surg 11: 69-72.
- D’Alessio MJ, Rana A, Martin JA, Moser AJ (2005) Surgical management of intraluminal duodenal diverticulum and coexisting anomalies. J Am Coll Surg 201: 143-8.
- Saranovic D, Djuric-Stefanovic A, Milovanovic A, Kratovac-Dunjic M, Masulovic D, Ivanovic A (2009) Education and imaging. Hepatobiliary and pancreatic: juxtapapillary duodenal diverticulum causing cholestasis. J Gastroenterol Hepatol 24: 496.
- Love JS, Yellen M, Melitas C, Yazici C, Zar F. Diagnosis and management of Lemmel syndrome: an unusual presentation and literature review. Case Rep Gastroenterol 16: 663-74.
FIGURE 1

Figure 1: NCCT upper abdomen with oral contrast. It shows two contrast- lled diverticula (white arrows) with an air- uid (contrast) level. Also, note hyperdense calculi (white arrowhead) in the lumen of the gall bladder
FIGURE 2
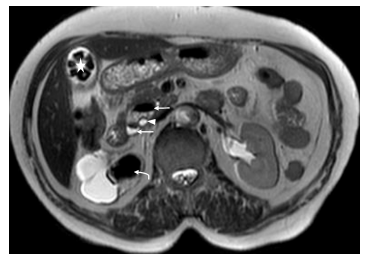
Figure 2: MRCP. T2 weighted axial image shows two periampullary diverticula (white arrows) around the common bile duct (white arrowhead) causing narrowing of the distal common bile duct with a luminal diameter of 2.8 mm at this level. Also, note the cholelithiasis (white star). Incidental nding of a large obstructive calculus (white curved arrow) in the right renal pelvis, which is causing gross hydronephrosis
FIGURE 3
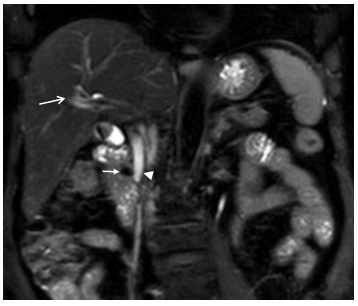
Figure 3: MRCP. T2-weighted SPAIR coronal image shows the smaller periampullary diverticulum (white arrow) with signi cant narrowing of the distal common bile duct (arrowhead) with a luminal diameter of 2.8 mm at this level. Also, note the mild to moderate degree of intrahepatic biliary radical dilatation (long white arrow)
Figures at a glance