Occupational Radiation Exposure and Cancer Risk Across Fluoroscopy-Guided Procedural Specialties
Received Date: January 16, 2026 Accepted Date: February 01, 2026 Published Date: February 03, 2026
doi: 10.17303/jrnm.2026.3.101
Citation: Ahmed J Marabeh, Ahmed Alzubaidi, Matthew Spaulding, Jeffrey Critchfield (2026) Occupational Radiation Exposure and Cancer Risk Across Fluoroscopy-Guided Procedural Specialties. J Radiol Nucl Med 3: 1-8
Abstract
Fluoroscopy-guided procedures (FGP) expose healthcare workers to low levels of ionizing radiation [8]. Although individual exposures are modest, cumulative lifetime dose can become clinically relevant, and a clinician’s role strongly influences overall radiation burden [1, 8]. This narrative review synthesizes research comparing occupational radiation patterns, epidemiologic cancer outcomes, and biological indicators of radiation effects across major fluoroscopy-exposed groups. Studies from 1990 to 2025 were included if they reported occupational dose estimates [1, 3, 7], cancer incidence or mortality [2, 4], or biomarkers of radiation-associated biological damage [10,11].
Interventional cardiologists demonstrated some of the highest head and neck exposures, consistent with asymmetric cranial dose measurements and reports of left-sided brain tumors [6, 11]. Radiologic technologists showed strong epidemiologic signals, including increased brain cancer mortality and higher melanoma and breast cancer incidence [2]. Interventional radiologists generally experienced moderate exposure, with modern data showing no clear rise in overall cancer mortality, although modeling studies indicate a small but measurable lifetime risk [1, 3, 4]. Vascular surgeons and peri-procedural nursing and anesthesia personnel demonstrated variable exposure patterns influenced by shielding and workflow [7, 8, 10]. Scatter measurements indicate that peri-procedural staff may receive meaningful doses when positioned near the patient during active imaging [7].
Overall, the literature shows that occupational radiation risk is not evenly distributed across fluoroscopy-exposed specialties [1, 2, 6]. These differences underscore the importance of consistent shielding, routine dosimetry, and updated studies that reflect contemporary procedures and equipment [8, 9].
Keywords: Interventional Radiology; Occupational Radiation; Fluoroscopy; Cancer Risk; Radiologic Technologists; Interventional Cardiology; Scatter Radiation
Introduction
Fluoroscopy-guided procedures have become more prevalent and essential in modern medicine due to the technology’s real-time visualization and minimally invasive nature [8]. As these procedures continue to advance with technology and frequency of use, healthcare professionals experience chronic low-dose ionizing radiation exposure [8]. Modern equipment and proper protective shielding have helped to mitigate exposure and improve safety; however, measurable exposure remains a cause for concern regarding long-term cancer risk [1, 8, 9].
Most published literature evaluates radiation exposure in single specialties rather than across the full procedural team. Interventional cardiologists often receive higher head and neck exposure due to operator position during coronary and electrophysiology procedures [6, 8, 11], while radiologic technologists accumulate substantial lifetime exposure due to their high procedural volume [2, 5]. Interventional radiologists typically work in well-shielded environments, potentially reducing measured exposure compared with other procedural specialties [1, 3, 8]. These differences illustrate why occupational cancer risk may not be uniform across fluoroscopy-guided professions.
Despite meaningful variation in workflow and shielding between specialties, there is no comprehensive synthesis comparing occupational cancer risk across all major fluoroscopy-exposed groups. A cross-specialty evaluation may help clarify which professional groups carry the greatest risk and how modern procedural environments influence long-term outcomes.
The purpose of this narrative review is to compare radiation exposure patterns, epidemiologic cancer findings, and biologic indicators of harm across interventional cardiologists, radiologic technologists, interventional radiologists, vascular surgeons, nurses, and anesthesia personnel. Understanding these differences can guide safety practices and highlight areas where further research is needed.
Methods
A focused literature search was conducted using PubMed and Google Scholar for studies published from 1990 to 2025. Search terms included interventional radiology, interventional cardiology, radiologic technologists, fluoroscopy, occupational radiation, cancer risk, scatter radiation, brain tumors, and DNA damage. A total of nine studies met inclusion criteria and were evaluated qualitatively [1-7, 10, 11]. Titles and abstracts were initially screened for relevance, followed by full-text review to confirm inclusion criteria. No language or geographic restrictions were imposed.
Review articles, guidelines, historical summaries, and studies that did not provide primary occupational dose or outcomes data were excluded from the analytic set but were used for contextual background where appropriate [8, 9]. Due to heterogeneity in study design and outcome measurement, results were synthesized qualitatively. This review is narrative in nature and does not follow a formal systematic review framework such as PRISMA.
Radiation Exposure Basics in Fluoroscopy-Guided Procedures
Scatter radiation reflected off the patient is the primary source of exposure for operators during fluoroscopy-guided procedures [8]. Dose is influenced by patient size, beam angulation, distance from the X-ray source, and fluoroscopy time [8]. It can be significantly reduced by appropriate positioning and protective equipment such as lead aprons, thyroid shields, ceiling-suspended shields, and leaded eyewear [8]. Interventional radiology procedural suites are generally better equipped with integrated fixed shielding compared to cardiology laboratories or operating rooms, which often rely on more mobile shielding [8]. Recent developments in automated exposure-modulation systems can further reduce scatter by adjusting beam output in real time [12]. These differences contribute to variation in exposure across fluoroscopy-reliant specialties.
Interventional Cardiologists
Interventional cardiologists consistently experience some of the highest cranial and upper-body exposures among physicians performing fluoroscopy, largely due to close, left-sided positioning near the X-ray source during coronary and electrophysiology procedures [6, 8, 11]. Their workstation position results in substantial asymmetric head dose [6, 11]. Several studies have reported left-sided brain tumor clustering and increased lens opacities among interventional cardiologists and associated staff, consistent with chronic occupational radiation exposure [6, 11]. Higher cumulative head dose and longer fluoroscopy times during complex procedures further contribute to their risk [6, 8].
Radiologic Technologists
Radiologic technologists participate in a high volume of fluoroscopy-guided procedures and spend substantial portions of the workday inside procedure rooms during active imaging. Unlike interventional radiologists, who perform a limited number of cases per day, technologists frequently assist in many more procedures across multiple physicians and specialties. As a result, their cumulative time exposed to scatter radiation is substantially higher, which contributes to some of the greatest occupational doses reported among imaging personnel [2, 5]. Their proximity to the patient during image acquisition, equipment adjustment, and room preparation during active fluoroscopy further increases exposure opportunities.
- increased brain cancer mortality
- higher melanoma incidence
- higher female breast cancer incidence
in technologists performing fluoroscopically guided procedures [2]. Exposure has decreased in recent decades due to improved technology and protection practices, but cumulative lifetime dose remains significant [2, 5].
Interventional Radiologists
Modern interventional radiology suites integrate optimized shielding, resulting in relatively low annual effective doses compared with other procedural specialties [1, 3, 8]. Modeled lifetime attributable cancer risks (LAR) for IR physicians range from 0.22% to 0.63% above the general population baseline, with thyroid cancer comprising a substantial portion of modeled excess risk [1].
Historical radiologists exposed before shielding advances exhibited elevated leukemia and skin cancer rates [9]. In contrast, modern epidemiologic studies do not show clear increases in cancer mortality or incidence among contemporary IR physicians [4, 8, 9]. Prospective dose measurements from early IR cohorts estimated annual fatal cancer risk at less than 1 in 10,000 per year when proper protection is used [3].
Vascular and Endovascular Surgeons
Vascular surgeons frequently perform fluoroscopy-guided procedures in operating rooms that rely on mobile C-arms, similar to those occasionally used in interventional radiology. However, the key difference is that interventional radiology suites are specifically designed for fluoroscopic work and incorporate fixed ceiling-suspended shields, table skirts, and controlled room layouts, whereas operating rooms generally lack these permanent protective structures [8]. As a result, vascular surgeons and OR staff may experience greater variability in upper-body and ocular exposure, especially during peripheral vascular interventions and endovascular aneurysm repair, where mobile shielding is less consistent and workflow often requires proximity to the patient [8, 10].
Although large-scale cancer studies in this group are limited, biomarker work in operating room personnel exposed to fluoroscopy has demonstrated increased chromosomal aberrations compared with unexposed controls [10]. Studies of posterior lens changes among fluoroscopy-exposed physicians and staff have also identified radiation-associated lens opacities, highlighting potential risk [11].
Nurses and Anesthesia Personnel
Exposure among peri-procedural nursing and anesthesia staff varies depending on their proximity to the patient during monitoring or equipment adjustments. Shielding use differs across institutions, and some workers may receive meaningful scatter dose when standing near the table during active fluoroscopy [7, 8]. Measurements show that scatter exposure to anesthesia personnel can be measurable and occasionally significant during interventional radiology and cardiology procedures, especially when protective barriers are not consistently used [7].
Cross-Specialty Comparison
Interventional cardiologists often receive the highest head and neck doses due to positioning and fluoroscopy time [6, 8, 11]. Radiologic technologists exhibit the strongest epidemiologic cancer signals among fluoroscopy-exposed healthcare groups [2]. Interventional radiologists experience moderate exposure and lower observed modern cancer incidence but retain measurable modeled lifetime risk [1, 3, 4]. Vascular surgeons and peri-procedural staff are understudied but demonstrate variable exposure patterns, with measurable scatter dose documented in anesthesia personnel during active fluoroscopy [7, 10].
Discussion
The studies reviewed here point to the same central idea: different specialties accumulate radiation differently, and it mostly comes down to the kind of work they do every day. People who stand near the patient for many cases—like radiologic technologists or interventional cardiologists—naturally pick up more scatter over the years. Meanwhile, interventional radiologists, vascular surgeons, and peri-procedural staff show broader variation depending on how their workspaces are arranged and how consistently they have access to shielding. This uneven pattern suggests that workflow choices matter at least as much as the fluoroscopy machine itself.
Looking across the literature, it’s also obvious that some groups have been studied far more thoroughly than others. Technologists and interventional cardiologists appear repeatedly in large datasets, but long-term information for nurses and anesthesia teams is still limited, even though they often work close to the table. Another challenge is that many existing studies rely on older equipment or partial monitoring, so the numbers don’t always reflect present-day fluoroscopy workflows. More consistent and modern dosimetry data would help clarify which roles still face higher risk.
At the same time, new imaging systems may help bring these exposure differences down. Some of the latest fluoroscopy platforms use AI-based beam-shaping tools that automatically tighten the X-ray field and optimize output frame-to-frame. Early work shows this approach can reduce dose without harming image quality [12]. As these systems become more widely used, especially in centers performing high volumes of cases, they may offer a realistic way to lower cumulative exposure for all team members
Limitations
This review is limited by heterogeneity across available studies, including design differences, small sample sizes, and variability in exposure measurement. Many studies rely on historical or self-reported dose data, which may not reflect current practices [1, 2, 8, 9]. Cancer outcomes such as brain tumors are rare, limiting statistical power [2, 4, 9]. Biomarker and ocular studies often include small samples and may not generalize across all specialties [10,11]. As a narrative review, article inclusion was not exhaustive. Survivor bias may also influence observed cancer outcomes, as individuals who remain in fluoroscopy-intensive careers may differ systematically from those who leave due to health concerns. In addition, publication bias toward positive or statistically significant findings may over represent associations between radiation exposure and cancer risk in the available literature.
Conclusion
Occupational radiation exposure differs meaningfully across fluoroscopy-guided procedural specialties. Interventional cardiologists and radiologic technologists exhibit the highest exposure patterns and concerning epidemiologic signals [2, 6, 11]. Interventional radiologists generally experience lower observed cancer incidence but retain measurable modeled lifetime risk [1, 3, 4]. Vascular surgeons, nurses, and anesthesia personnel have variable but non-trivial exposure profiles, particularly in settings with limited shielding [7, 10]. Improvements in shielding consistency, workflow optimization, and dosimetry use could reduce exposure across specialties. Future research should focus on large contemporary cohorts, biomarker and ocular studies, and cross-specialty comparisons to refine long-term occupational risk.
Conflicts of Interest
The authors declare no conflicts of interest.
This research received no external funding.
Author Contributions
A.J.M. conceptualized the review, conducted the literature search, drafted the manuscript, and prepared figures.
A.A. and M.S. assisted with literature review and manuscript editing.
J.C. provided senior mentorship, critical revisions, and final approval of the manuscript.
All authors reviewed and approved the final version.
- Lee WJ, Bang YJ, Cha ES, Kim YM, Cho SB (2021) Lifetime cancer risks from occupational radiation exposure among workers at interventional radiology departments. Int Arch Occup Environ Health. 94: 139-145.
- Rajaraman P, Doody MM, Yu CL (2016) Cancer risks in U.S. radiologic technologists working with fluoroscopically guided interventional procedures, 1994–2008. AJR Am J Roentgenol. 206:1101-1108.
- Niklason LT, Marx MV, Chan HP (1993) Interventional radiologists: occupational radiation doses and risks. Radiology. 187: 729-733.
- Linet MS, Kitahara CM, Ntowe E (2017) Mortality in U.S. physicians likely to perform fluoroscopy-guided interventional procedures compared with psychiatrists, 1979–2008. Radiology. 284: 482-494.
- Lee WJ, Choi Y, Ko S (2018) Projected lifetime cancer risks from occupational radiation exposure among diagnostic medical radiation workers in South Korea. BMC Cancer. 18: 1206.
- Tahiri Z, Sekkat H, Talbi M (2025) Radiation exposure in interventional cardiology: a narrative review of health effects and novel approaches to ensure radiation safety. Ther Radiol Oncol. 9.
- Fetterly KA, Mathew V, Lennon R, Bell MR, Holmes DR Jr, et al. (2008) Radiation exposure to anesthesia personnel during interventional radiology and cardiology procedures. J Vasc Interv Radiol. 19: 387-392.
- Miller DL, Vano E, Bartal G (2010) Occupational radiation protection in interventional radiology: guidelines of CIRSE and SIR. Cardiovasc Intervent Radiol. 33: 230-239.
- Linet MS, Kim KP, Miller DL (2010) Historical review of cancer risks in medical radiation workers. Radiat Res. 174: 793-808.
- Rozgaj R, Kasuba V, Sentija K, Prlić I (1993) Chromosome aberrations in operating room personnel. Am J Ind Med. 35: 642-646.
- Vano E, Kleiman NJ, Duran A (2010) Radiation cataract risk in interventional cardiology personnel. Radiat Res. 174: 490-495.
- Sánchez A, Vivas E, Sesma G (2020) Deep-learning–based real-time exposure modulation in fluoroscopy: dose reduction with preserved image quality. Med Phys. 47: 2443-2454.
FIGURE 1
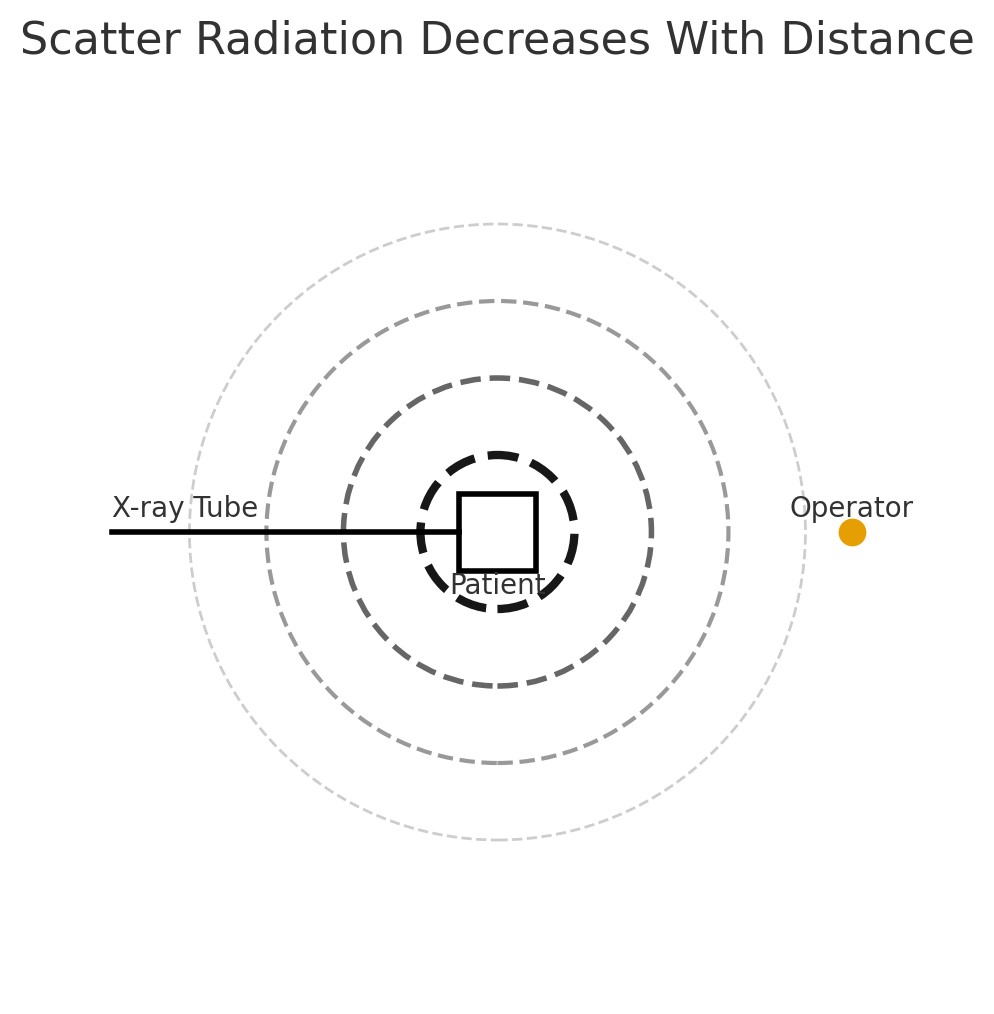
Figure 1: Conceptual Diagram of Scatter Radiation during Fluoroscopy
Figure illustrating the primary X-ray beam directed from the X-ray tube toward the patient, along with concentric rings representing decreasing scatter radiation intensity as distance increases. The operator stands in the typical position adjacent to the patient, showing how proximity influences exposure. Ceiling-suspended shielding and other barriers (not shown) can further reduce scatter dose. This conceptual schematic emphasizes the principle that scatter radiation decreases with distance from the patient.
FIGURE 2
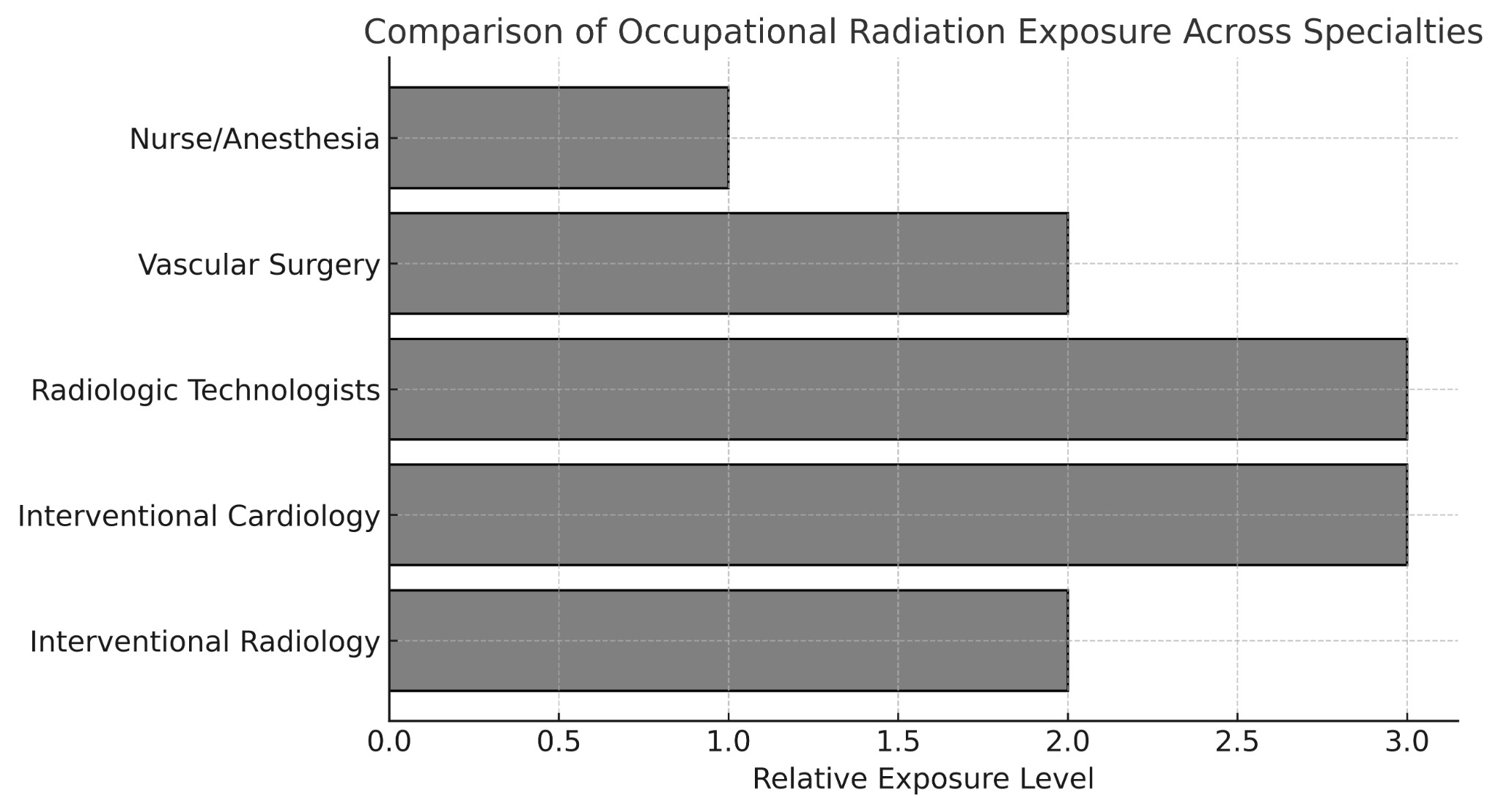
Figure 2: Relative Occupational Radiation Exposure across Fluoroscopy-Guided Specialties
Bar graph comparing approximate exposure levels among interventional radiologists, interventional cardiologists, radiologic technologists, vascular surgeons, and peri-procedural nursing/anesthesia staff. Values were derived qualitatively by synthesizing exposure trends reported in Lee et al. (1), Rajaraman et al. (2), Niklason et al. (3), Fetterly et al. (7), and Rozgaj et al. (10). These relative exposure categories reflect qualitative comparisons and are not intended to represent exact numerical dose values. Exposure categories are illustrative and intended for comparative purposes rather than representing precise dose measurements.
Tables at a glance
Figures at a glance