Ectopic Gallstone Obstructing Proximal Jejunum: an Unusual Cause of Intestinal Obstruction
Received Date: December 30, 2025 Accepted Date: January 17, 2026 Published Date: January 21, 2026
doi: 10.17303/jrnm.2026.3.102
Citation: Arun sharma, Shivali arya, Kamaldeep Singh, Manphool Singha (2026) Ectopic Gallstone Obstructing Proximal Je-junum: an Unusual Cause of Intestinal Obstruction. 3: 1-6.
Abstract
Gallstone ileus is a rare cause of intestinal obstruction occurring secondary to the erosion of larger gallstone into the intestinal lumen via cholecysto-enteric fistula. It generally affects elderly female patients with comorbidities and poses a significant diagnostic challenge due to inconsistent symptoms and lack of specific findings. Moreover, it produces intermittent or tumbling obstruction with waxing and waning of symptoms as the stone passes through the intestinal tract. A high index of suspicion is required for its early diagnosis and should be considered particularly in cases of intestinal obstruction in patients with known history of gallstones. Surgical management is the mainstay of treatment which depends upon the clinical condition of the patient. Here, we describe a case of gall stone ileus in an elderly female patient with ectopic gallstone obstructing the proximal jejunum which was managed surgically.
Keywords: Gallstone Ileus; Ectopic Gallstone; Intestinal Obstruction; Jejunal Obstruction; Rigler’s Triad; Cholecysto-Duodenal Fistula.
Introduction
Gallstones can cause various complications including rare gallstone ileus. Gallstone ileus is an uncommon entity occurring as a result of an internal fistula between the gallbladder and the intestine. Gallstones account for 1-4% of intestinal obstructions, most commonly involving the distal ileum [1-3]. Gallstone ileus resulting in jejunal obstruction is less common and the reported cases usually involve the distal jejunum. The reported mortality in gallstone ileus patients ranges from 12-18%, owing to old age and co-morbidities in such patients [4]. We present a case of ectopic gallstone obstructing proximal jejunum in an elderly female patient which was managed surgically.
Case Report
A 65-year old frail lady presented to the emergency department with complaints of abdominal distention, multiple episodes of bilious vomiting and constipation for 7 days. On general physical examination, patient was dehydrated and had tachycardia of 110-120 bpm. Abdomen was distended and non-tender with normal bowel sounds. Patient had history of hypertension for 20 years, on antihypertensives, underwent coronary artery bypass surgery 10 months back. The patient also had chronic cholecystitis with wall-echo-shadow complex documented on previous ultrasound report. Erect abdominal radiograph (Figure 1) showed dilated stomach, duodenum, and proximal jejunal loop with presence of air-fluid levels. No free air under the diaphragm was seen. Ultrasound abdomen revealed multiple echogenic foci in the biliary radicals with reverberation artefacts. Multiple air foci giving reverberation artifacts were also seen in the gall bladder fossa. Proximal small bowel loops were dilated. There was no prior history of endoscopic retrograde cholangiopancreatography procedure. Contrast enhanced CT (Figure 2) of the abdomen revealed partially distended gall bladder with a focal discontinuity in the wall of the fundus showing fistulous communication with the D2 segment of the duodenum suggestive of cholecysto-duodenal fistula. There was bilobar pneumobilia and common bile duct was filled with air throughout its course. Few air foci were seen inside the gall bladder and in the gall bladder fossa. The stomach, duodenum, and the proximal jejunal loops were dilated with a maximum small bowel caliber of 3.7cm. There was a calcified dual-rim oval structure suggestive of ectopic gallstone, measuring ~5x3.5x2.7 cm impacted in the jejunum. Bowel loops distal to this were collapsed.The patient underwent exploratory laparotomy via midline incision. There was gross dilatation of stomach extending till proximal jejunum which was ~4 cm dilated. At ~50 cm distal from duodenojejunal flexure, impacted stone was felt causing the transition point, distal to which rest of the small bowel was collapsed. A longitudinal enterotomy of ~3cm was done just distal to the stone and a large black pigmented gallstone was retrieved (Figure 3). Enterotomy was closed transversely using interrupted 3-0 polyglactin suture. No other ectopic gallstone was seen. Gallbladder fossa was frozen and the gall bladder could not be visualised due to dense adhesions with the duodenum. In view of poor cardiac reserve and the old age, cholecystectomy and fistula repair was not done in this setting. The patient had an uneventful post-surgical clinical course and is on follow up. Patient will be planned for cholecystectomy and fistula repair after optimisation and risk reduction.
Discussion
Gallstone ileus is a rare complication of gallbladder stones. This rare entity has been shown in 0.3-0.5% of gallstone patients with a predilection for female patients with nearly one fourth of such non-strangulated mechanical obstruction seen in the geriatric age group [4- 6]. Gallstone ileus is seen in patients suffering from frequent bouts of acute calculus cholecystitis with larger gallstones. The presence of large stones and frequent inflammation of the gallbladder leads to erosion of the gall bladder wall and surrounding organs. This results in the formation of fistula, commonly being cholecysto-duodenal, cholecysto-colic, and cholecysto-gastric fistulas. The gallstone passes through the fistula, commonly into the small intestine, rarely into the colon. Stones < 2.5cm pass spontaneously, whereas stones larger than 2.5cm get impacted, commonly at the ileo-caecal valve causing intestinal obstruction [7]. Although these stones can lead to obstructions of the proximal ileum, jejunum, and the sigmoid colon, rarely the stone can impact in duodenum causing Bouveret's syndrome [8]. Prior reports more commonly describe distal jejunal obstruction rather than more proximal as in present case [9, 10].
The presentation of gallstone ileus can be nonspecific due to inconsistent symptoms and lack of specific findings. The awareness and the knowledge regarding this condition is useful in suspecting this rare entity and look specifically for presence of gallstones as a cause of intestinal obstruction, particularly in patients with known history of cholelithiasis. The classical Rigler’s triad including pneumobilia, intestinal obstruction, and an aberrant gallstone can only be found in 11.11% and 14.81% of cases on ultrasound and plain radiograph respectively [11]. In our case, the old aged lady with history of cholecystitis presenting as intestinal obstruction, lead to the suspicion of gallstone ileus. Further radiological investigations including contrast enhanced CT lead to the accurate diagnosis of ectopic gall stone impaction in the proximal jejunum. Diagnostic radiology evaluation generally involves imaging with a plain radiograph of the abdomen in erect posture, utrasonography and contrast enhanced CT. The Rigler’s triad can be recognized on plain radiographs, though infrequently in cases of radiolucent stones. Ultrasonography in such cases can help to depict contracted gallbladder with remnant stones, although gaseous distension limits its efficacy. A combination of radiography and ultrasonography increases the sensitivity of diagnosing this condition. CT allows better demonstration of the location, size, and the number of aberrant gallstones in addition to the evaluation of adjacent bowel and direct visualization of the biliary-enteric fistula using multiplanar reconstructions [12]. The management varies according to the condition of the patient and ranges from shock-wave lithotripsy to surgical exploration. There can be one-stage or two-stage surgical procedures involving enterotomy and removal of the stones (enterolithotomy), enterolithotomy plus cholecystectomy, and repair of the fistula with or without bowel resection [9-10, 13]. Enterolithotomy is usually considered in the elderly patients with multiple comorbidities while enterolithotomy, fistula closure, and cholecystectomy are performed in relatively young, hemodynamically stable patients. The study comparing enterolithotomy alone versus single-stage cholecystectomy in the management of gallstone ileus showed no difference in terms of complications, readmissions, and mortality [14]. However, patients managed with both enterolithotomy with cholecystectomy had a longer hospital stay and higher hospital costs compared with enterolithotomy alone [14].
Conclusion
The radiologist and the surgeons should be aware of gallstone ileus as a cause of obstruction while dealing with elderly patients. A high index of suspicion is required to diagnose this rare cause of intestinal obstruction. Early diagnosis and surgical intervention can be life-saving in such patients.
- Hussain J, Alrashed AM, Alkhadher T, Wood S, Behbehani AD, et al. (2018) Gall stone ileus: Unfamiliar cause of bowel obstruction. Case report and literature review. Int J Surg Case Rep. 49: 44-50.
- Chatterjee S, Chaudhuri T, Ghosh G, Ganguly A (2008) Gallstone ileus--an atypical presentation and unusual location. Int J Surg. 6: e55- 6.
- Turner AR, Sharma B, Mukherjee S, Gallstone Ileus. (2022) In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; Jan-PMID: 28613584.
- Doko M, Zovak M, Kopljar M, Glavan E, Ljubicic N, et al. (2003) Comparison of surgical treatments of gallstone ileus: preliminary report. World J Surg. 27: 400-4.
- Nuño-Guzmán CM, Marín-Contreras ME, Figueroa-Sánchez M, Corona JL (2016) Gallstone ileus, clinical presentation, diagnostic and treatment approach. World J Gastrointest Surg. 8: 65-76.
- Bouziane M, Bouknani N, Kassimi M, Habi J, Guerroum H, et al. Gallstone ileus: An unusual cause of intestinal obstruction. Radiol Case Rep. 17: 129-132.
- Syme RG (1989) Management of gallstone ileus. Can J Surg. 1989. 32: 61-4.
- Adnan AI, Vaz OP, Lapsia S, Sultana A, et al. (2022) Bouveret's Syndrome: A Case Series and Literature Review on a Gallstone Disease Causing Gastric Outlet Obstruction. Cureus. 14: e27519.
- Alamoodi M (2023) Distal jejunal gallstone ileus-an unusual cause of bowel obstruction: a case report. J Surg Case Rep. 17: 557.
- Fatimah N, Ahmed AS, Warraich MU, Butt UI, Ahmad QA, et al. (2018) Stone in the distal jejunum presenting as small bowel obstruction: A case report. Int J Surg Case Rep. 52: 20-22.
- Lassandro F, Gagliardi N, Scuderi M, Pinto A, Gatta G, et al. Gallstone ileus analysis of radiological findings in 27 patients. Eur J Radiol. 50: 23-9.
- Lassandro F, Romano S, Ragozzino A, Rossi G, Valente T, et al. (2005) Role of helical CT in diagnosis of gallstone ileus and related conditions. AJR Am J Roentgenol. 185: 1159-65.
- Ravikumar R, Williams JG (2010) The operative management of gallstone ileus. Ann R Coll Surg Engl. 92: 279- 81.
- Khurshid MH, Hejazi O, Spencer AL, Nelson A, Stewart C, et al. (2025) A little goes a long way: A comparison of enterolithotomy versus single-stage cholecystectomy in the management of gallstone ileus. J Trauma Acute Care Surg. 98: 649-65.
FIGURE 1
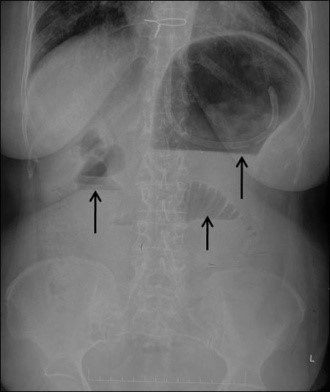
Figure 1: Plain radiograph of the abdomen in erect posture showing dilated stomach, duodenum, and the proximal jejunal loops with presence of air-fluid levels (black arrows).
FIGURE 2
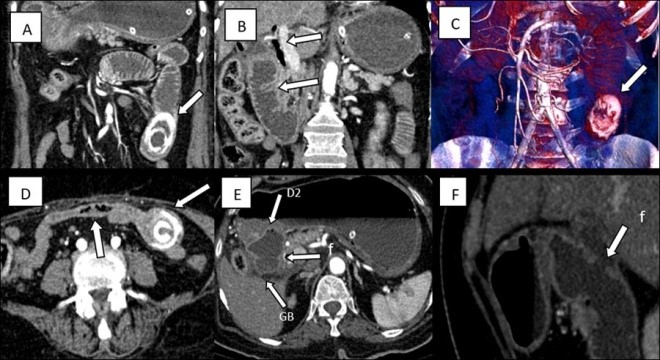
Figure 2(A-F):Contrast-enhanced CT images of the abdomen showing an ectopic gallstone impacted in proximal jejunum (A) with proximal dilated bowel and pneumobilia (B). Volume rendered CT image showing ectopic gall stone with dilated proximal small bowel(C). Bowel loops distal to the impacted gall stone are collpased (D) with delineation of the cholecysto-duodenal fistula (denoted by f) in the axial (E) and the sagittal (F) sections.
FIGURE 3

Figure 3(A-C): Intraoperative pictures showing impacted gall stone causing obstruction in proximal jejunum (A), longitudinal enterotomy with delivered stone (B) and retrieved black pigmented gall stone (C).
Figures at a glance