Primary Gallbladder B-Cell Lymphoma as a Finding in Post Cholecystectomy with Diffuse Gallbladder Wall Thickening: A Case Report
Received Date: March 24, 2023 Accepted Date: March 24, 2023 Published Date: March 27, 2023
doi: 10.17303/jspcr.2023.5.102
Citation: Foroutan MA, Mohammadi A, Ardeshiri MR (2023) Primary Gallbladder B-Cell Lymphoma as a Finding in Post Cholecystectomy with Diffuse Gallbladder Wall Thickening: A Case Report. J Surg Proce Case Rep 5: 1-7
Abstract
In the present paper, gallbladder lymphoma is reported in 77 years old man with the presentation of cholecystitis. Primary gallbladder lymphoma is a rare disease and over 98% of malignant tumors of the gallbladder are adenocarcinomas while less than 0.1–0.2% account for malignant lymphomas. The patient was referred to our clinic with RUQ and epigastric pain and discomfort. The sonography shows that the gallbladder was edematous and semi-contracted with diffuse wall thickening (6mm), particularly in the fundus. Primary gallbladder lymphomas are clinically represented mostly by acute cholecystitis and less as gallbladder mass. Low-grade lymphomas are radiologically represented only by the gallbladder wall's slight thickening.In our case, cholecystitis was represented by normal WBC count and aminotransferase level. Radiology reported only slight thickening of the gallbladder. The high ESR (105 mm) represented an inflammatory process, which possibly would require surgery and pathological reporting.
Keywords: Gallbladder Cancer; Lymphoma; Man
Abbreviations
GBC-Gallbladder Cancer, RUQ-Right Upper Quadrant, CT Scan-Computerized Tomography Scan
MRCP-Magnetic Resonance Cholangio pancreatography, CBD-Common Bile Duct, IHC-Immunohistochemistry, IHBD-Intrahepatic Bile Duct, PBL-Primary gallbladder lymphoma
Introduction
Primary gallbladder lymphoma is a rare disease [1], which is commonly presented as cholecystitis [2]. It is more prevalent in the elderly [3]. The mean age for this disease is within the range of 35-69 years old [3,4]. Cholecystitis is the most prevalent clinical sign [1,3]. In the present work, a 77-year-old man patient is reported with chronic abdominal pain. The initial diagnosis before surgery due to the signs, symptoms, lab findings and sonographic report,was cholecystitis. After laparoscopic cholecystectomy, the histopathological finding didn’t indicate the cholecystitis and the final diagnosis was gall bladder malignancy as lymphoma.
Case Report
A 77-year-old man was referred to our clinic with RUQ (Right Upper Quadrant) and epigastric pain and discomfort for the past 3 months. Then, some other symptoms were added such as nausea, dizziness, and vomiting, for one week of hospitalization. During this period, he had weakness but no weight loss. During hospitalization, his skin color seemed yellowish and the pain in RUQ had worsened.He possessed dyspepsia for 2 years and hypothyroidism and chronic obstructive pulmonary disease (COPD) in the past medical history. His medication was levothyroxine (100 μg) daily. Moreover, suffering from dyspnea, he used Fluticasone & Salmeterol inhaler (SEROFLO Inhaler 25/250 mcg.) for a long time. There was no history of diabetes mellitus, hypertension or any surgery. In physical examinations he was afebrile (T=37.2 C) with a blood pressure of 115/75 mmHg. pulse rate was 78 per minute and respiratory rate was 12/min with 96% Spo2. There was no cervical or axillary lymphadenopathy in physical examination, and the breathing sound was normal along with no skin lesion. His bowel sound was normal and there was no abdominal distention, although abdominal palpation in RUQ was tender without Murphy's sign.
Results of coagulation tests were normal along with normal red-cell indexes and blood levels of globulin (Table 1).
For image assessment, a chest radiograph was performed accompanied by an abdominopelvic CT scan (Computerized Tomography Scan) with IV contrast, MRCP (Magnetic Resonance Cholangiopancreatography), and abdominopelvic sonography. The span of the liver was 160mm in sonography representing fatty liver (grade 1). A simple cyst with a diameter of 25*24 mm was seen and several reactive lymph nodes were also observed in the liver hilum. In the proximity to the fundus of the gallbladder, there was a simple cyst with a diameter of 11 mm. Extrahepatic and intrahepatic bile ducts were not dilated. The gallbladder was edematous and semi-contracted with diffuse wall thickening (6 mm), particularly in the fundus. Near the side of the fundus, some cystic formation was found along with a hyperechoic lesion with a diameter of 21*6. The diameter of CBD (Common Bile Duct) was 10 mm and an aneurysmal dilatation was observed in the infrarenal portion of the abdominal aorta. Prostate and kidney were normal.
Through an esophagogastroduodenoscopy, duodenitis was found in the D1 and D2 portions. The size of the upper limit in the MRCP liver was normal. There was the signal intensity in the two parts, which could be caused by various fatty filtration. A strand-like filling defect was noted in the portal vein and the right branch, which could be partial thrombosis. The deformed configuration was found in the gallbladder with a cystic-like distal portion.
There was a wall thickening of more than 11 mm in the inferior wall (the length of 33 mm). The CBD diameter was 9mm and the pancreatic duct and IHBD (Intrahepatic Bile Duct) were slightly dilated. A small mass was noted like a lesion in D2 of the duodenum and a biopsy was taken from it.
Cardiac and respiratory consults with pulmonary function test and echocardiography were conducted before surgery. Echocardiography was normal with EF was 55%, and FEV1/FVC was 80.5% and normal.
we decided finally to perform the Laparoscopic cholecystectomy for the patient because of his pain and symptoms of chronic cholecystitis.
After the histopathologic assessment of the surgical sample, the findings were suspicious for malignant small round cell tumor in favor of malignant lymphoma. In the IHC (Immunohistochemistry) study, the CD20, LCA, CD3,CD10, BCL2, CD5 were positive but the staining of CD79a hadn`t been performed. Therefore, morphologic study and IHC staining were kept with low-grade B-cell lymphoma,most possibly extranodal marginal zone lymphoma. The biopsy of duodenal lesion had no evidence of malignancy.
In the evaluation after surgery, because of patient intolerance and denial, other evaluation such as PET Scan and bone marrow examination remained unfinished and he unfortunately refused any follow up and treatments.
Discussions
Gallbladder cancers (GBC) are rare in the fifth rank in neoplasms of the gastrointestinal tract [5]. Patients older than 60 years are affected by GBC [6]. Extranodal lymphomas account for about 1/4 of non-Hodgkin’s lymphomas[7]. They occur mostly in the gastrointestinal tract not generally in the gallbladder [7]. Primary gallbladder lymphoma (PBL) is scarce and more than 98% of malignant tumors of the gallbladder are adenocarcinomas while malignant lymphomas account for less than 0.1–0.2% [6, 8]. Clinically,primary gallbladder lymphoma appears with acute cholecystitis and less as a gallbladder mass[9]. Low-grade lymphomas present radiologically only with a slight thickening of the gallbladder wall [8].
Considering the characteristics of the disease, the absence of specificity of the clinical features, and its late diagnosis,it is difficult to prognose gallbladder cancer [10].Mostly, the diagnosis is late leading to morbidity and mortality in advanced stages [11].
In our case, cholecystitis was presented with normal WBC count and aminotransferases level. Only slight thickening of the gallbladder was radiologically reported.The high ESR (105 mm) denoted an inflammatory procedure.The most important risk factor associated with gallbladder cancer is cholecystolithiasis, whichexists in more than 70% of the cases [12]. However, there was no stone in the gallbladder in our case. It is essential to assess other risk factors including chronic infections resulting in cholangitis, environmental factors like diet, toxic ingestions, aflatoxins,vitamin deficiencies, elevated capsaicin consumption, obesity,and poor socio-economic circumstances [13] but it is unclear that the risk factors for gallbladder primary malignant lymphoma are the same as other gallbladder cancers.
Conclusions
This is an extremely rare occurrence of Primary gallbladder lymphomas which was clinically diagnosed as cholecystitis. Most of them clinically present with symptoms of cholecystitis. Primary gallbladder lymphomas are challenging due to its rarity. no population studies have been performed in our country. Gallbladder cancers are rare and evaluating the incidence is uncleared in this region.For definite diagnosis, histopathology and immunohistochemistry are mandatory. Treatment options include surgery with the use of chemotherapy in disseminated disease and inoperable cases.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. The patient understands that their name and initials will not be published and due efforts will be made to conceal the identity, but anonymity cannot be guaranteed.
Conflicts of interest
The authors declare that they have no conflict of interest.
Acknowledgment
We would like to thank the Research and Technology Deputy of Kurdistan University of Medical Sciences, Sanandaj,Iran, for its contributions to this study.
- Psarras K et al. (2014) Primary gallbladder small lymphocytic lymphoma as a rare postcholecystectomy finding.
- Sudo Y et al. (2018) Gallbladder Malignant Lymphoma Diagnosed after Surgery for Acute Cholecystitis-A Case Report 45: 85-7.
- Mani H et al. (2010) Gall bladder and extrahepatic bile duct lymphomas: clinicopathological observations and biological implications 34: 1277.
- Al-Katib S, R Colvin, FJC rir Sokhandon (2018) Intravascular Large B-Cell Lymphoma Presenting with Diffuse Gallbladder Wall Thickening: A Case Report and Literature Review.
- Apodaca-Rueda M et al. (2017) Prevalence of gallbladder cancer In patients submitted to cholecystectomy: experience of the University Hospital, Faculty of Medical Sciences,State University of Campinas–UNICAMP 44: 252-6.
- Castro FA et al. (2013) Biliary tract cancer incidence in the United States—demographic and temporal variations by anatomic site 133: 1664-71.
- Zucca E et al. (1997) Primary extranodal non-Hodgkin’s lymphomas. Part 1: Gastrointestinal, cutaneous and genitourinary lymphomas 19: 20.
- Ono A et al. (2009) Primary malignant lymphoma of the gallbladder: a case report and literature review. 82: 15-9.
- Mitra S et al. (2014) Mucosa associated lymphoid tissue lymphoma of gallbladder: a rare presentation 57: 502.
- Roa I et al. (1997) Curative resection in potentially resectable tumours of the gallbladder 163: 419-26.
- Perpetuo MDCM et al. (1978) Natural history study of gallbladder cancer. A review of 36 years experience at MD Anderson Hospital and Tumor Institute 42: 330-5.
- Diehl A, VJTL Beral (1981) Cholecystectomy and changing mortality from gallbladder cancer 318: 187-9.
- Nemunaitis JM et al. (2018) Gallbladder cancer: review of a rare orphan gastrointestinal cancer with a focus on populations of New Mexico 18: 665.
FIGURE 1
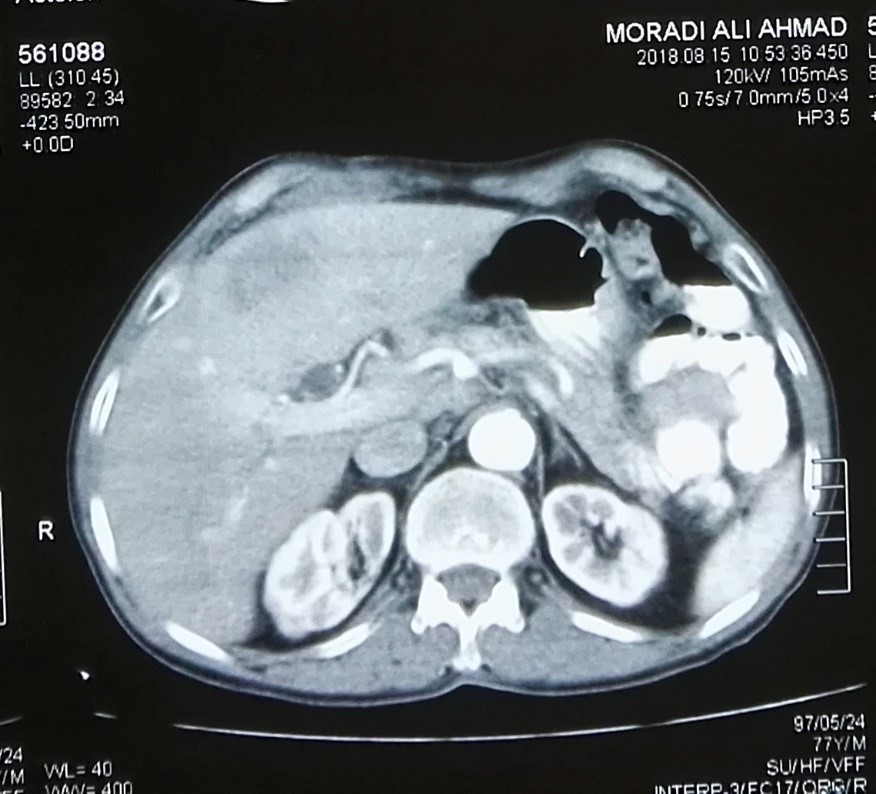
Figure1: The computed tomography demonstrating the gallbladder
Tables at a glance
Figures at a glance