Rosai-Dorfman Disease of Thymus. A Rare Mediastinum Tumor: A Case Report
Received Date: April 11, 2023 Accepted Date: May 11, 2023 Published Date: May 15, 2023
doi: 10.17303/jspcr.2023.5.103
Citation: Moaath M AL Smady, Bayan A Ibrahim, Manar H Hajeer, NijmetzahraA Damlakhy (2023) Rosai-Dorfman Disease of Thymus. A Rare Mediastinum Tumor: A Case Report. J Surg Proce Case Rep 5: 1-7
Abstract
Rosai-Dorfman disease (RDD) is a rare idiopathic benign non-Langerhans histiocytic disease characterized by the histiocyte proliferation in the lymph nodes or extra nodal sites. We reported a 56-year-old woman who presented with an anterior mediastinum mass found incidentally on a contrasted CT scan that was suggestive of a thymic lesion. The patient underwent total thymectomy through a median sternotomy approach. The histopathological examination and immunohistochemistry results were consistent with RDD. In conclusion, the thymus is an uncommon but possible site for Primary RDD, and it is difficult to make a diagnosis without surgical resection and biopsy.
Keywords: Rosia Dorfman Disease; Thymus; Mediastinum; Thymoma; Lymphadenopathy
Abbreviations: Rosia Dorfman Disease (RDD), Contrased Tomography (CT), Anti Acetylcholine Receptor Achr).
Introduction
Rosai-Dorfman disease (RDD) is a rare non-Langerhans histiocytic disease that was initially recognized by Destombes in 1965 and followed by Rosai and Dorfman in 1969 as they called it “sinus histiocytosis with massive lymphadenopathy” [1]. It has an incidence rate of 1:200,000 with only about 100 reported cases worldwide [2]. Rosia Dorfman disease (RDD) is classified into familial and sporadic types and the sporadic type is classified into four groups according to the site of involvement which includes classic nodal RDD, extra nodal RDD, neoplasia-associated RDD and immune disease-associated RDD [3]. The most common subtype is the classic nodal form, which usually presents with bilateral painless cervical lymphadenopathy with constitutional symptoms like fever, weight loss, and night sweats [3]. Extra-nodal disease that involves skin,nasal cavity, bone, and central nervous system could be seen in a significant number of cases, but the thymus is an uncommon site for presentation. The diagnostic evaluation of patients suspected to have (RDD) should involve laboratory studies including erythrocyte sedimentation rate, complete blood count, and serum immunoglobulins and imaging modalities like CT/PET scans [3] Herein, we reported a rare case of isolated thymus RDD which was confusing and difficult to distinguish from thymoma.
Case Presentation
A 56-year-old non-smoking woman with a past medical history of hypothyroidism treated with levothyroxine, a liver hemangioma, and an active H.pylori infection on triple therapy presented to cardio-thoracic surgery clinic at Jordan University Hospital in Oct 2022 with an incidental finding of a thymic lesion on a PAN-CT scan done for liver hemangioma follow-up. She complained of generalized fatigue, feeling hotness with no documented fever,night sweats, poor appetite, and weight loss of 10 kg in the last two months prior to her presentation. The patient denied any symptoms of chest pain, dyspnea, cough, dysphagia,or hoarseness of voice. Her physical examination showed no obvious abnormalities, lymphadenopathy, or masses. All her laboratory tests were within normal range.The chest X-ray was unremarkable with no obvious or defined lesion. The chest CT scan with contrast (figure 1A,1B) revealed a wedge-shaped soft tissue lesion with internal vascular structures seen at the superior mediastinum at the site of presumed residual thymic tissue measured approximately 4 x 2.6 cm in axial dimensions, highly suggestive of thymic lesion.
Results
The patient was initially diagnosed to have a suspicion of thymoma. Subsequently, she was referred to a neurology specialist, and myasthenia Gravis disease was ruled out by negative anti-AchR antibodies and normal nerve conduction studies.
The patient was scheduled for surgery to reach a definitive diagnosis of the lesion. She underwent total thymectomy of both lobes through a median sternotomy approach.During the operation, the left thymic lesion was large, measured around 5*5cm in size, was resected completely and sent for histopathology.
The surgery was uneventful, passed smoothly with no postoperative complications, and she has been followed up to date with no need for additional treatment options and with no signs of disease recurrence.
Macroscopic Examination
One specimen fixed in formalin was received that measures 13.1x6.5x3.2 cm and weighs 57 grams. Upon step sectioning, the specimen was almost totally replaced by tan to white homogenous lesion.
Microscopic Examination
Routine hemotoxyline and eosin stained sections revealed diffuse effacement of the architecture by sheets of large histiocytes exhibiting enlarged, round to oval hypochromatic nuclei with abundant eosinophilic cytoplasm (Fig.2A) with surrounding lymphoplasmacytic infiltrate (Fig.2A and 2B). In areas, the histiocytes engulf lymphocytes,referred to as emperipolesis (Fig.2C and 2D). Immunohistochemical staining revealed diffuse staining of the histiocytes for S100 and CD68 stains with focal cyclin D1 staining and negative staining for CD1a (to exclude Langerhans cell histiocytosis) and pankeratin (Fig.3). The plasma cell population was polytypic and highlighted by mixed staining for kappa and lambda immunohistochemical stains. The histopathologic diagnosis was consistent with Rosai Dorfman Disease.
Discussion
Rosai Dorfman disease (RDD) is a rare idiopathic benign disorder characterized by histiocyte proliferation in the body, mainly in the cervical lymph nodes, and presents as painless lymphadenopathy with constitutional symptoms.Most commonly, it affects young adults and children under the age of 20 [4].
Approximately 40% of RDD cases can occur in at least one extra nodal organ. However, the literature review showed that isolated thymus RDD is rare and has been reported in a few number of cases [5-8].
Around 100 cases of thymectomy have been operated in Jordan University hospital over the last 5 years, this is the only discovered case of RDD in the thymus. To our knowledge, only four Cases of isolated thymic RDD have been previously reported [5-8].
Isolated thymic RDD has to be differentiated from other anterior mediastinum masses which typically includes thymic malignancies (35%), lymphoma (25%), thyroid masses (15%), teratoma (10%), malignant germ cell tumors (10%) and benign thymic lesions (5%) [9].
The pathogenesis of RDD was not well understood,but some recent studies support the theory of the neoplastic process as it displayed clonality evidence in a subgroup of cases [3]. RDD lesions have been shown to be FDG-avid similar to other benign and malignant lymphoproliferative disorders because of the intense glucose dependence of the highly proliferating histocytes [10]. Many risk factors have been reported to be associated with (RDD) development which include genetic mutation in NRAS 2 exon in familial type, viral infections (herpes, HIV), neoplasia (lymphoma sarcoma), and autoimmune diseases (lupus, autoimmune hemolytic anemia)
The evaluation of RDD involves medical history,physical examination, imaging studies, and laboratory evaluations.However, the diagnosis of extra nodal RDD through radiological imaging (CT/PET) alone is challenging. Since they demonstrated non-specific findings. Therefore, a biopsy is mandatory to confirm the diagnosis.
The histopathological characteristic of RDD is the sinus expansion with large histiocyte which has lymphocytes,red blood cells, plasma cells, or polymorphonuclear leukocytes within its cytoplasm [6]. In immunohistochemistry analysis, RDD is recognized by the accumulation of CD68-positive, S100-positive, and CD1a-negative histiocytes with frequent emperipolesis [1]. Emperipolesis which defined as the active engulfment (phagocytosis)of one cell into and through a larger one, could be a biological or a pathological process like in Rosai Dorfman disease. Thymoma was on top of our differential diagnosis, it is composed of the neoplastic thymic epithelial cells scattered in variable population of lymphocyte which can be confused with RDD. As a result, immunohistochemistry can be a useful tool in differentiating between them, as thymus cells can express carcinoembryonic antigen (CEA), cytokeratin (CK),epithelial membrane antigen (EMA) and have negative staining for S100, in contrast to RDD.
Sporadic type of RDD usually has a good prognosis,with spontaneous remission occurring in 50% of cases, and can be managed by observation [3]. Surgical treatment is recommended in unifocal extra nodal or symptomatic disease [3]. Systemic therapy, including corticosteroids, chemotherapy, and radiotherapy may be required in extra nodal multifocal irresectable disease [3]. Since the disease has a favorable outcome in most cases with the reported mortality rate of approximately 7%, most patients prefer conservative management over surgery [11]. However, the patient in our case had an extra-nodal type therefore the surgery was the treatment of choice to confirm the diagnosis and to rule out other serious conditions.
In conclusion, the thymus is an uncommon site for Primary RDD, and it is difficult to make a diagnosis without surgery. It should be considered in the differential diagnosis of anterior mediastinum masses especially if the diagnosis is suspicious after ruling out popular causes.
- Goyal G et al. (2019) “Clinicopathological features, treatment approaches, and outcomes in Rosai-Dorfman Disease,”Haematologica 105: 348-57.
- Zhang P, Liu F, Cha Y, Zhang X, Cao M (2021) Self--Limited Primary Cutaneous Rosai-Dorfman Disease: A Case Report and Literature Review. Clin Cosmet Investig Dermatol 14: 1879-84.
- Bruce-Brand C, Schneider JW, Schubert P (2020) “Rosai-Dorfman Disease: An overview,” Journal of Clinical Pathology 73: 697-705.
- Rosai-Dorfman Disease - symptoms, causes, treatment:Nord (2023) National Organization for Rare Disorders.
- Jia T et al (2022) “A rare case of thymic Rosai-Dorfman disease mimicking malignancy on 18F-FDG PET/CT,” Tomography 8: 2839-43.
- Shen C, Liao H (2021) “An extremely rare case of Rosai-Dorfman Disease in the thymus,” Journal of Cardiothoracic Surgery 16.
- Liu S, Tang E, Xu G, Lei J (2022) Rosai-Dorfman Disease in the thymus: A case report. Asian Journal of Surgery.
- Tsujimura R, Sato D, Obikane H, Kawachi R, Sugitani M et al. (2021) Hao H, Sakurai H, Yamakawa M, Masuda S. Rosai-Dorfman disease of thymus with elevated serum anti-acetylcholine receptor antibody: a case report. Int J Clin Exp Pathol 14: 1061-4.
- Almeida PT, Heller D (2022) Anterior Mediastinal Mass.
- Shaikh F, Awan O, Mohiuddin S, Farooqui S, Khan SA, McCartney W (2015) 18F-FDG PET/CT imaging of Extranodal Rosai-Dorfman Disease with Hepatopancreatic involvement A Pictorial and Literature Review. Cureus.
- Deen IU, Chittal A, Badro N, Jones R, Haas C (2022) Extranodal Rosai-Dorfman Disease- a Review of Diagnostic Testing and Management. J Community Hosp Intern Med Perspect 12: 18-22.
FIGURE 1
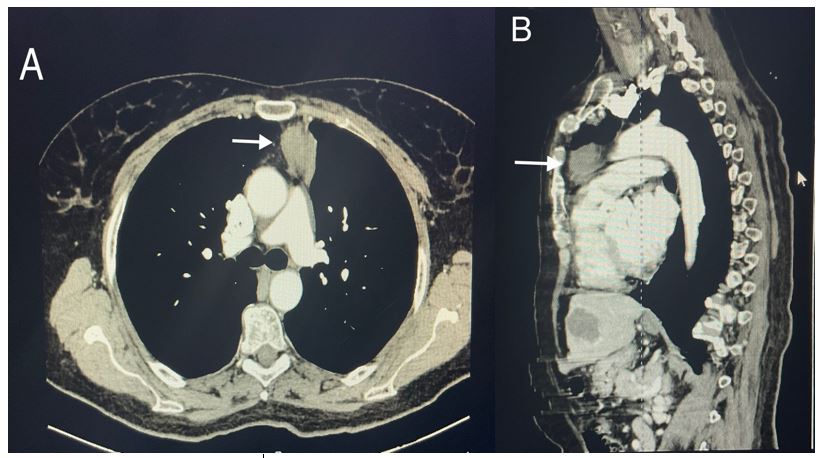
Figure 1: chest CT scan with contrast. (A) axial section, (B) Sagittal section
FIGURE 2

Figure 2A: Diffuse effacement of thymic architecture by sheets of histiocytes (hematoxylin and eosin stain, 100x) Figure 2B: Sheets of histiocytes with surrounding lymphoplasmacytic infiltrate (hematoxylin and eosin stain, 200x).
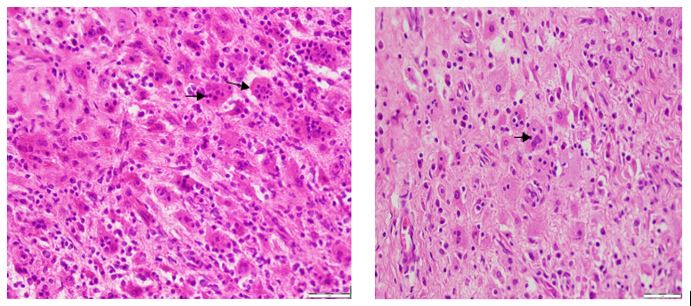
Figure 2C: histiocytes engulfing intact lymphocytes referred to as emperipolesis “arrow head” (hematoxylin and eosin stain, 400x). Figure 2D: histiocytes engulfing intact lymphocytes referred to as emperipolesis “arrow head” (hematoxylin and eosin stain, 400x).
FIGURE 3
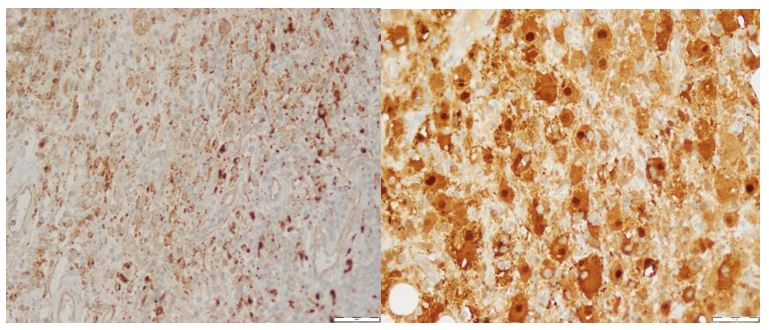
Figure 3A: Diffuse positive staining for CD68 “histiocytic marker” (CD68 immunostain, 400x). Figure 3B: Diffuse nuclear and cytoplasmic staining for S100 (S100 immunostain, 400x).

Figure 3C: Focal nuclear staining for cyclin D1 (Cyclin D1 immunostain, 400x). Figure 3D: Negative staining for CD1a (CD1a, 400x).
Figures at a glance