Hemosuccus Pancreaticus in a Patient with Hepatic Artery Variation: the Report of a Challenging Case
Received Date: May 28, 2023 Accepted Date: June 28, 2023 Published Date: July 01, 2023
doi: 10.17303/jspcr.2023.5.104
Citation: Alimohamad Moradi, Ali Gandominejad, Siavash Khaki, Niloofar Ayoobi Yazdi, Ali Jafarian (2023) Hemosuccus Pancreaticus in a Patient with Hepatic Artery Variation: the Report of a Challenging Case. J Surg Proce Case Rep 5: 1-9
Abstract
Hemosuccus pancreaticus (HP) is one of the causes of upper gastrointestinal bleeding, which is defined as bleeding from the pancreatic duct into the gastrointestinal tract. Because of the rarity of this disease, it is challenging to diagnose and ultimately treat the disease, even though early treatment can prevent the patient from the mortality and morbidity.
This study introduces an HP case in a patient with a rare hepatic artery variation. The 54-year-old man has been hospitalized several times for chronic upper gastrointestinal bleeding and complications caused by chronic anemia. Finally, the diagnosis of HP was confirmed through a triphasic computerized tomography. Because of the location of the aneurysm, the patient underwent surgical treatment.
In addition to considering HP as an uncommon cause of GI bleeding, sometimes it is recommended to discuss the diagnosed patient in a multidisciplinary team meeting to select the best treatment approach. Since it is a rare disease with many anatomical variations in aneyrsm as well as variations in hepatic arteries.
Keywords: Hemosuccus Pancreaticus; Gastrointestinal Bleeding; Aneurysm
Introduction
Hemosuccus Pancreaticus is a rare, potentially fatal cause of Obscure Gastrointestinal Bleeding. It is defined as bleeding from the pancreatic duct to the gastrointestinal tract via the ampulla of Vater [1,2]. Pancreatitis, either acute or chronic, is commonly the main cause of HP. HP can also be caused by pancreatic neoplasms, pancreatic pseudocyst, and even iatrogenic trauma [3-11]. They cause erosion of pancreatic duct and fistula formation to adjacent vascular structures.
In 1970, Sandblom described Hemosuccus Pancreaticus for the first time [2]. Because HP is a rare condition,it is almost limited to case reports in the medical literature.HP presents upper gastrointestinal bleeding, including hematemesis and more common melena. Hematemesis is less common and ruptures into the abdominal cavity or retroperitoneum are rare [12-14]. In most cases, the bleeding is intermittent, recurrent, and not severe enough to affect the patient's hemodynamics. Thus, the majority of patients show chronic anemia symptoms. However, some patients may present with severe hematemesis or shock as a first clinical manifestation and require immediate blood transfusions [12].
HP is challenging to diagnose because of its anatomical location, intermittent bleeding, and rarity. The condition is almost never identified through endoscopy and There are no significant changes in blood tests. Liver tests are usually normal except for the increase in bilirubin that occurs during pancreaticobiliary reflux. Except in cases of acute pancreatitis, serum amylase is usually normal [15].HP is caused mostly by aneurysms outside or inside the pancreas,mostly in the splenic, gastroduodenal, and pancreaticoduodenal arteries [16,17]. The purpose of this study is to introduce a rare case of HP in a patient with uncommon hepatic artery variation that made the treatment challenging.
Case Report
A 54-year-old man with type 2 diabetes presented to our emergency department with weakness, lethargy, hematemesis,melena, dyspnea, and dizziness. After initial resuscitation with normal saline and ten pack cell units, the patient underwent esophagogastroduodenoscopy (EGD) where no definite bleeding was evident, only a clean base ulcer was observed in the prepyloric region. Re-endoscopy after 48 hours also revealed no bleeding site. The sonography resulted in no significant finding, and the patient was discharged in a stable condition on antiacid medication and advised following up regularly. Three months later, the patient returned to the emergency department with weakness and lethargy. The initial hemoglobin level was 5 g/dl, and all other laboratory tests including kidney and liver function tests and coagulation profiles were normal.
The patient underwent gastroesophagogastroduodenoscopy with normal results. Then a full colonoscopy was performed. Multiple blood clots were seen all over the colon, and fresh blood was seen in the ascending colon and cecum. Some large-size diverticula without evidence of active bleeding were also seen in the right colon. After resuscitation with normal saline and blood products, the patient was discharged with close follow-up.
A week later, the patient returns to the emergency department with the same complaint. A hemoglobin of 3.4g/dl was found this time, and the laboratory tests were normal as before. The patient underwent an esophagogastroduodenoscopy after resuscitation, which was normal, but this time, our gastroenterologist also performed a push enteroscopy.In the stomach, there was no evidence of blood. Bulb and D1 to D2 of the duodenum were normal, but there were minimal clots and evidence of previous bleeding from the major papilla with no active bleeding. The patient had been consulted by the hapatopancratobilliary surgery department. Because of a history of multiple episodes of GI bleeding with unknown origins, we recommended a triphasic computerized tomography (CT) scan of the abdomen and pelvis with pancreas protocol, as well as magnetic resonance cholangiopancreatography (MRCP) (Figure1 and 2).The CT scan revealed an aneurysm in the gastroduodenal artery (GDA), and MRCP revealed an extrinsic indentation on pancreatic duct, confirming the diagnosis of HP. In addition, the CT scan demonstrated an unusual variation of the hepatic artery, in which the common hepatic artery arises from the superior mesenteric artery (Type IX Michel classification) (18). The GDA aneurysm was placed in the proximal portion of GDA shortly after it rose from the CHA (Figure3).
The patient was discussed in the hapatopancreatobilliry multidisciplinary team. A surgical procedure was preferred over angioembolization due to the proximity of the aneurysm to its origin and the risk of hepatic artery thrombosis or chemical embolization during the angiographic aneurysm occlusion.
Through a right subcostal incision, the doudenom was fully kocherized and dissected off the hepatic flexure of the colon to fully expose the pancreatic head and GDA territory.The liver hilum was explored for arterial exposure of the proper hepatic artery and its connection to the GDA, as well as the GDA and its aneurysmal sac. Upon achieving proximal and distal control, the aneurysmal sac was opened in a controlled manner, a 5 cc clot and degraded material were removed from the sac, and the roof of the arterial aneurysm sac was partially resected. The small feeding vessels were also repaired. Considering the arterial variation mentioned above, after excluding the GDA aneurysmal sac,it was necessary to reconstruct the liver arterial inflow. The end-to-side anastomosis of the proper hepatic artery to the splenic artery was done with continuous sutures of Prolene7.0. There was a cystic cavity at the pancreatic head region,which was covered with a serosal patch with the lateral duodenal wall. In addition, a rim of omental patch was prepared and applied to the site. (Figure 4).
The patient was discharged after 5 days with stable hepatic arterial flow and no local complications related to the resection of the aneurysmal sac. After a year of follow-up, CT scans, MRCP, and routine lad data were all normal,and the patient has not complained of gastrointestinal bleeding.
Discussion
HP is a rare cause of upper gastrointestinal bleeding that originates in the pancreas, pancreatic duct, or structures close to the pancreas, or vessels near the pancreas such as the splenic artery [3,4]. HP is typically caused by acute or chronic pancreatitis. Iatrogenic trauma, vascular aneurysms, and pancreatic neoplasms are also possible causes [4-12]. Acute or chronic pancreatitis can result in damage to the pancreatic duct, and pancreatic juice can rupture arteries adjacent to the pancreas, eventually resulting in HP.Additionally, pancreatic pseudocysts and pancreatic stones can cause inflammation in the pancreatic duct that ultimately results in HP [19]. It is believed that pancreatic enzymes play an important role in the formation of HP. As an example, the pancreatic pseudocyst contains lytic enzymes (e.g.Elastase) that cause damage to the arterial wall and lead to hemorrhage [20-22]. Usually, bleeding in HP occurs intermittently. In a study by Zuchelli et al., clot formation in the main pancreatic duct was found to be the cause of intermittent bleeding [23]. HP can also be caused by pancreatic neoplasms,such as pancreatic carcinoma, serous cystic neoplasm, cystic mucinous neoplasm, and endocrine tumors.As Matsumoto et al. showed pancreatic cyst tumors bleeding into the pancreatic duct could be one of the HP causes [8]. In the literature, HP has been linked to iatrogenic trauma during procedures such as T-tube implantation and endoscopic needle aspiration [24,25]. In addition, special conditions such as pancreas divisum are mentioned [26].
The formation of pseudoaneurysms and aneurysms of arteries, such as those in the spleen, the common hepatic, the gastroduodenal, and the pancreaticoduodenal,has been reported as a cause of bleeding [16]. In rare cases non-aneurysmal vascular malformations is the source of bleeding [27].
HP is a rare disease, so epidemiological studies in this area are limited. The onset age of HP varies widely, but occurs most frequently between the ages of 32 and 36 [12,15,23]. It is also estimated that HP is five times more prevalent in men. Symptoms of this disease typically include upper GI bleeding, which may manifest as hematemesis or melena. The most common symptom is melena, while hematomas are less common. Abdominal or retroperitoneal bleeding is extremely rare [12-14]. As a result of obstruction of the wirsung duct and an increase in intraductal pressure caused by blood clot formation, patients may experience colic abdominal pain. Usually, bleeding occurs intermittently and recurrently, and is not severe enough to cause hemodynamic instability. As a result, most patients develop chronic anemia. Occasionally, HP can cause severe gastrointestinal bleeding and even shock in its early stages, which requires immediate resuscitation and blood transfusions [12].It is important to ask patients about their history of pancreatitis and alcohol consumption, since pancreatitis is one of the leading causes of HP [28].
The disease is rare and insidious, and there is little information available about it, which makes it less likely to be considered as a differential diagnosis in patients with upper gastrointestinal bleeding. On the other hand, the disease manifests primarily as intermittent and chronic bleeding or just signs of chronic anemia, all of which make diagnosis challenging. Furthermore, the instruments used to diagnose upper gastrointestinal bleeding may not be able to detect HP easily. Due to the intermittent nature of bleeding in HP, the patient may have undergone numerous endoscopies without a definitive diagnosis. In most cases, laboratory tests are normal [15]. A patient with upper GI bleeding usually undergoes an upper endoscopy to rule out other causes of the condition. However, active bleeding from the ampulla of Vater is rarely observed during the endoscopy [29-31].The probability of detecting the bleeding during the endoscopy was mentioned as 30 percent [32]. Ultrasound can be useful in showing pancreatic pseudocysts and aneurysms of the arteries around the pancreas. CT angiography and contrast-enhanced abdominal CT scans are effective methods of examining the pancreas and abdominal vessels. The CT scan plays a significant role in the diagnosis of HP. The gold standard for the diagnosis and treatment of vascular disorders in HP is abdominal vessels angiography.
HP can be treated surgically or non-surgically. Radiological interventional procedures or endovascular therapies are highly effective in hemodynamically stable patients,with a success rate of 67 to 100% [33]. Endovascular treatment options include balloon angioplasty, stent placement,and emobilization. Coil embolization is the most widely used procedure, which induces thrombosis within the pseudoaneurysm in order to stop bleeding. When a patient's hemodynamics are unstable, emergency surgery may be required.
In many cases, the surgical procedure may include the resection of the pseudoaneurysm or pseudocyst. If resection is not possible, the distal and proximal portions of the involved artery can be ligated. Extra cystic ligation is an alternative treatment for pseudocysts [34]. The location of the lesion also affects the patient's prognosis. In addition to angioembolization, distal pancreatectomy may also be an appropriate treatment option when pseudoaneurysms are located in the body or tail of the pancreas. The surgical approach to pseudoaneurysms located in the head of the pancreas can be challenging and can be accompanied by a high rate of mortality and morbidity. Thus, angioembolization is the treatment of choice [15]. Sometimes it is difficult to determine the exact location of the bleeding, in which case other measures such as Intraoperative sonography and Pancreatoscopy can be used [16]. Today New therapeutic techniques have been introduced, including EUS-guided angiotherapy for the treatment of HP [35].
If left untreated, HP can cause several complications,including massive gastrointestinal hemorrhage, chronic anemia, ruptured viscera, retroperitoneal blood accumulation and in severe cases multiorgan failure and death [36].The overall mortality rate for HP is up to 9.6% [12]. Conservative treatment alone can result in an increase in mortality of up to 90% [36]. A relatively limited amount of information is available in the literature regarding the long-term outcome of HP and comparisons between surgical and nonsurgical outcomes. It is therefore important to conduct large multicenter clinical registry-based research projects in order to investigate trends and natural histories of this disease.
The location of the aneurysm in the head of the pancreas and the uncommon variation of the hepatic artery made treatment difficult in our case. Since we anticipated the need for liver vascular reconstruction, we decided that surgery was safer in this particular case.
The HP is a rare cause of GI bleeding with different anatomy of aneurysms and pseudoaneurysms and the several variations of hepatic artery, which makes treatment selection challenging. In addition to considering HP as an uncommon cause of GI bleeding, sometimes it is recommended to discuss the diagnosed patient in a MDT meeting to select the best treatment approach.
- Callinan AM, Samra JS, Smith RC (2004) Hemosuccus pancreaticus. ANZ J Surg 74: 395-7.
- Sandblom P (1970) Gastrointestinal hemorrhage through the pancreatic duct. Ann Surg 171: 61.
- PEtienne S, Pessaux P, Tuech J-J, Lada P, Lermite E,Brehant O et al. (2005) Hemosuccus pancreaticus: a rare cause of gastrointestinal bleeding. Gastroenterol Clin Biol 29:237-42.
- Panackel C, Kumar A, Subhalal N, Krishnadas D, Kumar KR V (2007) Hepatobiliary and pancreatic: Hemosuccus pancreaticus complicating calcific chronic pancreatitis. J Gastroenterol Hepatol 22: 1691.
- Jakobs R, Riemann JF (1992) Hemosuccus pancreaticus due to a pressure ulcer in pancreatolithiasis. Dtsch Med Wochenschr 117: 1956-61.
- Meneu JA, Fernandez-Cebrian JM, Alvarez-Baleriola I, Barrasa A, Morales V, Carda P (1999) Hemosuccus pancreaticus in a heterotopic jejunal pancreas. Hepatogastroenterology 46: 177–9.
- Shinzeki M, Hori Y, Fujino Y, Matsumoto I, Toyama H, Tsujimura T et al. (2010) Mucinous cystic neoplasm of the pancreas presenting with hemosuccus pancreaticus: report of a case. Surg Today 40: 470-3.
- Matsumoto Y, Miyamoto H, Fukuya A, Nakamura F,Goji T, Kitamura S et al. (2017) Hemosuccus pancreaticus caused by a mucinous cystic neoplasm of the pancreas. Clin J Gastroenterol 10: 185-90.
- Kim SS, Roberts RR, Nagy KK, Joseph K, Bokhari F,An G et al. (2000) Hemosuccus pancreaticus after penetrating trauma to the abdomen. J Trauma Acute Care Sur 49:948–50.
- Cheruvattath R (2009) Diehl DL. Hemosuccus pancreaticus after EUS-FNA of a pancreatic tail cyst. Gastrointest Endosc 70: 817.
- Garcea G, Krebs M, Lloyd T, Blanchard K, Dennison AR, Berry D (2004) Haemorrhage from pancreatic pseudocystspresenting as upper gastrointestinal haemorrhage.Asian J Surg 27: 137-40.
- Maheshwaran MU, Sathyanesan J, Ramasamy S, Palaniappan R, Manoharan G (2016) Hemosuccus pancreaticus:18-year experience from a tertiary care GI bleed centre in India.HPB 18: e784.
- Kuhn R, Janocha F, Lazar A, Rambach W, Paquet KJ (1996) Ruptured pseudoaneurysm of the splenic artery. A complication of chronic pancreatitis. Dtsch Med Wochenschr 121: 1567-70.
- Han B, Song Z-F, Sun B (2012) Hemosuccus pancreaticus:a rare cause of gastroirtestiral bleeding. Hepatobiliary Pancreat Dis Int 11: 479-88.
- Rammohan A, Palaniappan R, Ramaswami S, Perumal SK, Lakshmanan A, Srinivasan UP et al. (2013) Hemosuccus pancreaticus: 15-year experience from a tertiary care GI bleed centre. Int Sch Res Not.
- Toyoki Y, Hakamada K, Narumi S, Nara M, Ishido K, Sasaki M (2008) Hemosuccus pancreaticus: problems and pitfalls in diagnosis and treatment. World J Gastroenterol WJG 14: 2776.
- Ferreira J, Tavares AB, Costa E, Maciel J (2015) Hemosuccus pancreaticus: a rare complication of chronic pancreatitis.Case Reports bcr2015209872.
- Michels NA (1955) Blood supply and anatomy of the upper abdominal organs: with a descriptive atlas. Lippincott.
- Gutkin E, Kim SH (2012) A novel endoscopic treatment of hemosuccus pancreaticus: a stent tree tamponade. JOP J Pancreas 13: 312-3.
- Maeda A, Kunou T, Saeki S, Aono K, Murata T, Niinomi N, et al. (2002) Pseudoaneurysm of the cystic artery with hemobilia treated by arterial embolization and elective cholecystectomy. J Hepato‐Biliary‐Pancreatic Surg 9: 755-8.
- Ray S, Das K, Ray S, Khamrui S, Ahammed M, Deka U (2011) Hemosuccus pancreaticus associated with severe acute pancreatitis and pseudoaneurysms: a report of two cases. JOP J Pancreas 12: 469-72.
- Somani PO, Jain SS, Shah DK, Khot AA, Rathi PM (2013) Uncomplicated spontaneous rupture of pancreatic pseudocyst into stomach: A case report. World J Gastrointest Endosc 5: 461.
- Zuchelli T, Alsheik E, Bhandari B, Ringold D (2014) A unique case of hematemesis in a 17-year-old female. ACG Case Reports J 1: 151.
- Singh P, Gelrud A, Schmulewitz N, Chauhan S (2008) Hemosuccus pancreaticus after EUS-FNA of pancreatic cyst (with video). Gastrointest Endosc 67: 543.
- Keswani RN (2010) Hemosuccus pancreaticus after endoscopic ultrasound-guided fine needle aspiration of a pancreatic cyst. Endoscopy 42: 79-79.
- Vazquez-Iglesias JL, Durana JA, Yanez J, Rodriguez H, Garcia-Vallejo L, Arnal F (1988) Santorinirrhage: hemosuccus pancreaticus in pancreas divisum. Am J Gastroenterol (Springer Nature) 83.
- Yokoyama I, Hashmi MA, Srinivas D, Shaikh KA, Levine SM, Sorokin JJ et al. (1984) Wirsungorrhagia or hemoductal pancreatitis: report of a case and review of the literature. Am J Gastroenterol (Springer Nature) 79.
- Sul HR, Lee HW, Kim JW, Cha SJ, Choi YS, Kim GH, et al. (2016) Endovascular management of hemosuccus pancreaticus, a rare case report of gastrointestinal bleeding.BMC Gastroenterol 16: 1-4.
- Vimalraj V, Kannan DG, Sukumar R, Rajendran S,Jeswanth S, Jyotibasu D et al. (2009) Haemosuccus pancreaticusdiagnostic and therapeutic challenges. HPB 11: 345-50.
- Arnaud J-P, Bergamaschi R, Serra-Maudet V (1994) Pancreatoduodenectomy for hemosuccus pancreaticus in silent chronic pancreatitis. Arch Surg 129: 333-4.
- Risti B, Marincek B, Jost R, Decurtins M, Ammann R (1995) Hemosuccus pancreaticus as a source of obscure upper gastrointestinal bleeding: three cases and literature review. Am J Gastroenterol (Springer Nature) 90.
- Péroux JL, Arput JP, Saint-Paul MC, Dumas R, Hastier P, Caroli FX, et al. (1994) Wirsungorrhagia complicating chronic pancreatitis associated with a neuroendocrine tumor of the pancreas. Gastroenterol Clin Biol 18: 1142–5.
- Gambiez LP, Ernst OJ, Merlier OA, Porte HL, Chambon JPM, Quandalle PA (1997) Arterial embolization for bleeding pseudocysts complicating chronic pancreatitis. Arch Surg 132: 1016-21.
- Rantala A, Ovaska J (1996) Major haemorrhage associated with a pseudocyst in chronic pancreatitis: a gastro-surgical challenge. In: Annales chirurgiae et gynaecologiae 217-21.
- Will U, Mueller A-K, Grote R, Meyer F (2008) “Hemosuccus pancreaticus”–primarily ultrasound-guided successful intervention using transcutaneous fibrin glue application and histoacryl injection. Ultraschall der Medizin-European J Ultrasound 29: 260-3.
- Alshaikhli A, Al-Hillan A (2021) Hemosuccus pancreaticus.
FIGURE 1

Figure 1: Black Arrow: Coronal view of the GDA aneurysm with scant amount of hematoma around it in the pancreatic head region, White Arrow: The Proper Hepatic Artery
FIGURE 2
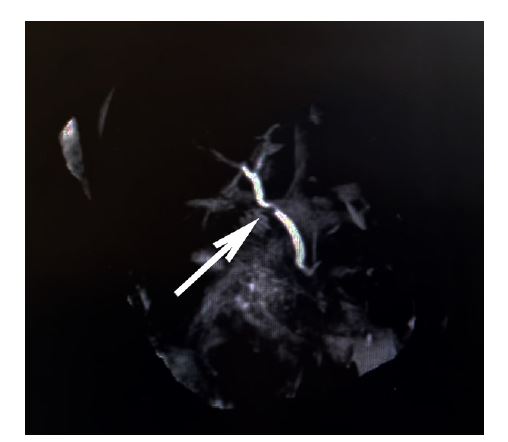
Figure 2: The MRCP shows the indentation of the aneurysm on the biliary system (Common Bile Duct)
FIGURE 3
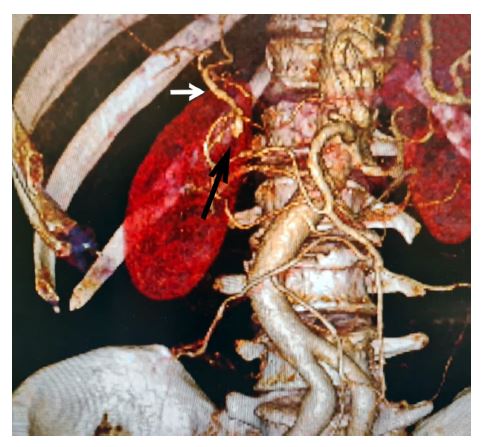
Figure 3: Three-dimensional CT angiography of GDA's aneurysmal site. Black Arrow indicated the sac, note the variation of the common hepatic artery originating from SMA, No inflow from celiac trunk. White arrow: The Proper Hepatic Artery
FIGURE 4

Figure 4: Post operation Triphasic CT scan, after reconstruction of hepatic artery, Black Arrow: End to side arterial anastomosis of proper hepatic artery to splenic artery. White arrow: The Proper Hepatic Artery
Figures at a glance