Bilateral Arcocristectomy in Cervical Spinal Stenosis via an Unilateral, Minimally Invasive Approach with a Tubular System
Received Date: August 14, 2023 Accepted Date: September 14, 2023 Published Date: September 16, 2023
doi: DOI: 10.17303/jspcr.2023.5.105
Citation: Ulrich Hubbe, Marco Bissolo, Marc Hohenhaus, Jürgen Beck, Christoph Scholz (2023) Bilateral Arcocristectomy in Cervical Spinal Stenosis via an Unilateral, Minimally Invasive Approach with a Tubular System. J Surg Proce Case Rep 5: 1-10
Abstract
Open posterior osteoligamentous decompression is a therapeutic option in cases of degenerative cervical myelopathy due to predominantly dorsal compression. This surgical approach has major disadvantages, such as neck pain due to dissection of the paravertebral muscles and potential instability of the cervical spine. To avoid these effects minimal invasive surgical techniques are increasingly common. Minimally invasive arcocristectomy can be performed using a small ipsilateral skin incision and bilateral partial superior and inferior laminectomy. We present this innovative technique together with the data of six patients. Surgery was performed in the prone position on a radiolucent carbon table with the head fixed in a Mayfield clamp. After fluoroscopic segment identification, a small lateral incision was made, and a tubular system was inserted using blunt dissection. Under the operative microscope, ipsi- and contralateral decompression was achieved through partial laminectomy and resection of the flavum ligament. This technique can also be performed for multilevel stenosis.
The retrospective evaluation of six patients showed that arcocristectomy yielded statistically significant volumetric gain in the cervical spinal canal. A statistically significant clinical improvement was also observed.
We introduce microsurgical arcoristectomy via a unilateral tubular approach as a new technique to decompress the spinal canal in selected cases of degenerative cervical myelopathy in a minimally invasive manner while preserving stability.
Keywords: Arcocristectomy; Degenerative Cervical Myelopathy; Posterior Decompression; Minimally Invasive; Tubular System
Introduction
In degenerative cervical myelopathy (DCM) due to cervical stenosis, the open posterior approach is often performed in cases of predominantly dorsal compression [1]. This approach, which is generally associated with a long posterior skin incision, can compromise the stability of the cervical spine, especially in cases of multilevel decompression. This may lead to kyphotic deformities associated with cervicalgia and the need for subsequent posterior fusion [2]. To avoid such complications several minimally invasive techniques for cervical pathology have been described in recent years and have been validated in long-term studies, with results comparable to those of traditional open approaches [3-5].
In patients with mainly posterior constriction of the spinal cord and without signs of instability or deformity, a so-called “arcocristectomy” is an alternative therapeutic option [6,7]. In this technique, the superior part of the lamina of the inferior vertebral body, the inferior part of the lamina of the superior body, and the ligamentous tissue running here are removed, leading to widening of the spinal canal avoiding the removal of the hemilamina [6]. As only a part of the vertebral arch is removed, and the spinous process, the nuchal ligaments, most of the laminae and the vertebral joints remain intact, the stability is less impaired, and instrumentation with a screw-rod system is therefore unnecessary [6,7]. This minimally invasive technique protects most of the posterior structures and likely preserves biomechanical functions [6]. This technical note describes a new technique of arcocristectomy, which was performed through a minimally invasive tubular system in patients with DCM. The clinical results of the four patients were supplemented.
Surgical Indications
The indications for arcocristectomy with a minimally invasive tubular system were monolevel or multilevel posterior compression of the spinal cord in patients with lordotic configuration of the cervical spine.
Contraindications
The contraindications for arcocristectomy with a minimally invasive tubular system were kyphotic configurations of the cervical spine, spinal cord compression due to anterior cervical stenosis, cervical stenosis with instability, and spinal cord compression due to neoplastic disease.
Instruments and Materials
When performing minimally invasive arcocristectomy using the tubular system, the following instruments and materials were required: skull clamp, intraoperative fluoroscopy, a minimally invasive tubular system, an operating microscope, bipolar forceps, a high-speed drill, a diamond ball burr, a straight Kerrison rongeur, microforceps, microscissors, and bajonetted dissectors.
Positioning and Surgical Setup
The patient was positioned prone on a radiolucent carbonic table (Figure 1a). The head was fixed using a skull clamp for optimal and stable positioning. The shoulders were gently pulled inferiorly and fixed by tape. The target segment was identified using fluoroscopy, and the incision line was marked (Figure 1b). The approach was planned at an angle of approximately 45° in the direction of the lamina on the side of the maximal stenosis. The operative field was then disinfected and the patient’s neck was draped in a standard manner.
Step by Step Instructions for the Procedure
Step 1: Incision and Insertion of the Minimally Invasive Tubular System
A transversal 18-20 mm skin incision was made along the skin cleavage lines as a 14 mm tube was found to be sufficient for the intervention. The underlying subcutaneous tissue and nuchal fascia were bluntly dissected, and the dilator of the tubular system was inserted into the paraspinal musculature in the direction of the bone of the facet joint lateral to the interlaminar window under lateral fluoroscopic guidance. At this step, it was important to find the bony contours of the adjacent laminae at the target level using the first dilator of the tubular system to identify the exact position of the interlaminar window. This maneuver was performed to prevent unintended penetration of the flavum ligament with the risk of spinal cord injury. The correct level was confirmed using lateral fluoroscopy. The next series of dilators were sequentially placed over each other. The depth markings on the dilators indicated the appropriate tube length according to the patient’s anatomy, which was then placed over the dilators. The flexible arm was secured, and the sequential dilators were removed to establish a tubular operative corridor (Figure 1c). The final position of the tube was verified by fluoroscopy (Figure 1d).
Step 2: Ipsilateral Osteoligamentous Decompression
Next, the microscope was brought above the surgical field, and the remaining muscular and connective tissues were electrocauterized and removed under sufficient magnification. After exposure of the bony structures, the superior portion of the ipsilateral inferior lamina and the inferior portion of the ipsilateral superior lamina were identified. If needed, the tube was pivoted to obtain an optimal view of the anatomical landmarks. Osteoligamentous decompression was initiated at the inferior lamina. Using a high-speed diamond ball burr, the bone of the inferior half of the ipsilateral vertebral arch was meticulously resected until only a flexible transparent layer was left; this was then elevated with a small hook and removed with a small Kerrison–Rongeur. During this procedure, the spinous process and interspinous ligament were preserved. Osteoligamentous decompression continued with removal of the inferior part of the lamina of the superior vertebra. We recommend maintaining the ipsilateral ligamentum flavum during this step. This will protect the dura, and, more importantly, the otherwise relieved dura would obstruct the view for contralateral decompression (Figure 3a).
Step 3: Contralateral Osteoligamentous Decompression
After completion of the ipsilateral bony decompression, the tube was pivoted contralaterally to expose the inferior part of the superior spinous process and the contralateral inferior part of the superior lamina (Figure 2c and 2d). The angle of the tube was parallel to the contralateral lamina, allowing vision along the gap between the posterior dura and the inner surface of the flavum ligament and the adjacent laminae. Again, the superior part of the lamina of the lower vertebra was removed, while preserving the interspinous ligament using a high-speed drill. The use of a punch was avoided, as the back of the instrument tended to punch the dura and spinal cord. Osteoligamentous decompression continued with removal of the inferior half of the ipsilateral vertebral arch (Figure 3b). Next, the superiorly and inferiorly detached flavum ligament was elevated with a hook and then removed with a small rongeur bilaterally.
Step 4: Inspection, Hemostasis, and Closure
Sufficient osteoligamentous decompression of the cervical dura was visually controlled (Figure 2e and 2f). Using microinstruments, the superior and inferior margins of the addressed segment were then palpated to identify any structures that may still cause compression (Figure 3c). After ensuring that the nerve structures were tension-free, meticulous hemostasis was performed (Figure 3d). After irrigation, the tubular system was smoothly removed and the microhemorrhages along the surgical corridor were cauterized. The wound was closed with subcutaneous sutures and dermal adhesive.
Postoperative Management
After surgery, the patient was monitored in the recovery room and transferred to the neurosurgical ward. Postoperative local pain was typically minor and was treated with non-steroidal anti-inflammatory drugs or weak opioid analgesics. The patient was mobilized on the first postoperative day. No neck collar was applied. MRI was performed for volumetric measurements of the decompression.
Complications
The possible complications of minimally invasive arcocristectomy are likely to be similar to those of other well-established surgical strategies, such as anterior cervical discectomy and fusion or posterior decompression [7]. Nerve root or spinal cord injury can occur during osteoligamentous decompression due to manipulation of the neuronal structures or as a result of postoperative bleeding. Any patient with new radicular or myelopathic symptoms after surgery should undergo MRI.
Pitfalls
The procedure should be performed by experienced surgeons and requires a great deal of expertise with tubular systems. In our view, the most technically demanding and potentially risky step is “Step 3: Contralateral Osteoligamentous Decompression.” When dissection turns to the contralateral side for arcocristectomy via a unilateral portal, the soft tissue dissection mechanism becomes a “side-to-side” movement, which is biomechanically difficult, and constrained by the tubular system. This dissection mechanism also has the potential to expose the dura and cord to damage. This is evident in the attached video from 3.30 to 4.30 min. It is essential that the first step is decompression with a diamond ball burr. Similar to hearing preservation surgery for intrameatal vestibular schwannoma, decompression is achieved before the soft tissues close to the dura are manipulated. Subsequently, these soft tissues can be lifted off the dura and the myelon within and removed. Accordingly, we do not use a punch to remove the ligaments, but a rongeur. With the diamond ball burr and the rongeur, decompression can be performed safely and sufficiently based on our previous experience. Emergency magnetic resonance imaging (MRI) is always recommended in cases of postoperative neurological deterioration, as this is the only way to reliably assess postoperative hemorrhage. Immediate surgical decompression must be performed in cases of spinal cord compression and can be performed again using the same access point. In contrast to posterior decompression with screw-rod instrumentation, and similar to Cervical unilateral laminotomy for bilateral decompression wound healing disorders are observed extremely rarely with the tubular approaches, as the muscular traumadue to the dilatation is very small and the skin wound measures < 2 cm.
Clinical data
Methods
This procedure has been carried out in our department since 2016. Currently a prospective feasibility trial, the ArcoCristectomy for CErvical Spinal Stenosis trail (ACCESS), is ongoing in our department.
The retrospective evaluation of six patients which underwent surgery from February 2016 till October 2018 was approved by the local ethics committee (EK 402/18) and was registered in the German Clinical Trials Register (DRKS00016857).
Follow-up occurred 6 weeks, and 12 months after surgery. Postoperative neck pain was assessed using the numerical rating scale (NRS). The mJOA score was used for the clinical evaluation of myelopathy.
Volumetric analysis
MRI scans were obtained pre- and postoperatively in five of six patients on a Siemens Magnetom Sempra 1.5 Tesla (Siemens Medical Solutions, Forchheim, Germany). Spine imaging was performed according to our institutional standard MRI protocol. Volumetric measurements were performed on T2 Space sequences on Brainlab Iplan using the smart brush tool (v.4.5, BrainLab, Feldkirchen, Germany). For pre- and postoperative volumetric measurements, 2- mm slices were utilized. To restrict volumes to the level of decompression, volumes were measured between the basivertebral foramen of the superior and inferior vertebra relative to the level of decompression.
Results
The mean age was 77 (range 62-84). Clinical details are summarized in Table 1. We operated the C3/C4 segment in four patients and the C5/C6 segment in two patients. In four cases, the preoperative symptoms were hypesthesia, ataxia, and mild tetraparesis due to spinal cord compression. One patient experienced incontinence and ataxia.In one case, the patient underwent surgery because of paresthesia and dysmetria. Average mJOA score at admission was 12 (SD 2; range 9-14). 1 year postoperatively this value improved to 15 ± 2. This clinical improvement was not statistically significant (p = .078).
In all patients, the average surgical time was 102 min (range, 53–181 min), and the bleeding volume was < 50 ml for each patient. None of the patients had relevant neck pain, defined as NRS score > 5 or underwent surgery for signs of instability or cervical deformity.
Volumetric analyses are summarized in Table 1. Arcocristectomy through a tubular system yielded statistically significant volumetric gain in the cervical spinal canal (p= .045)
Discussion
Different surgical options and approaches are available for DCM [2,8]. Posterior surgical approaches are often performed in cases of predominantly dorsal compression of the neurological structures [2]. The major disadvantage of this approach is neck pain due to soft tissue trauma and extensive dissection of the paravertebral muscles from the bony structures. Moreover, in multilevel decompression, there is a high risk of instability and deformities [9,10].
The concept of bilateral spinal decompression through a unilateral laminotomy approach was first described in 1997 in lumbar surgery [11,12]. Subsequently, minimally invasive options have been published to perform this technique at all levels of the spine including the cervical spine [13,14].
Recently Mielke et al. and Hur et al. reported a muscle-sparing, novel technique of bilateral osteoligamentous decompression via hemilaminectomy for DCM [14,15]. The authors demonstrated in further works that bilateral osteoligamentous decompression via hemilaminectomy can achieve a comparable degree of decompression as laminoplasty for DCM, performing only unilateral muscle detachment in addition to carefully preserving the supraand interlaminar ligaments [16].
Arcocristectomy through a classical open approach was first described in 1972 by Breig et al.and was later developed to prevent kyphotic deformities in patients with multilevel DCM [1]. When performing arcocristectomy, the upper half of the inferior cervical lamina, the lower half of the superior lamina, and the flavum ligament are removed to increase the diameter of the spinal canal without the need of a laminotomy [1].
More recently, Amaral et al. described three-to five-level acrocristectomy through an open approach in 17 patients. Postoperative imaging showed an increase in sagittal spinal canal diameter, and the clinical results were consistent. Cervical pain or deformities have not been reported [7]. Recently, Eicker et al. described a full-endoscopic arcocristectomy on ten formalin-fixed human cervical specimens. The authors described a mean increase of 4.1 mm (± 1.2 mm) in the sagittal diameter of the cervical spinal canal (p < 0.05) [6].
The purpose of the current technical note was to demonstrate the technical feasibility of arcocristectomy performed through a minimally invasive tubular system, avoiding the tissue trama of an open approach, and to report the first clinical results. Similar to the data of Amaral et al., we achieved good clinical results after spinal decompression at the 1-year follow-up in all patients. The minimally invasive tubular system enables surgeons to avoid the invasiveness of an open posterior approach, which allows for a minor incidence of postoperative neck pain and preservation of cervical spine stability. As a further advantage, this technique allows sufficient decompression of both sides of the spinal canal through a single unilateral small skin incision without removing the hemilamina. Pivotation of the minimally invasive tubular system permits decompression of adjacent levels.
Conclusions
Minimally invasive arcocristectomy is a feasible but demanding technique for effective decompression of predominantly posterior cervical spinal canal stenosis while also preserving good biomechanical stability and motion of the segment with minimal postoperative discomfort. We intend to analyze the safety and efficacy of this technique in a prospective study, in which we will attempt to refine specific criteria for this surgical technique.
Conflict of Interest
The authors report no conflict of interests. This research did not receive any specific grants, technical support or corporal support from funding agencies in the public, commercial, or not-for-profit sectors.
- Epstein NE (2003) Laminectomy for cervical myelopathy. Spinal Cord 41: 317-27.
- Hirabayashi K, Bohlman HH (1995) Multilevel cervical spondylosis. Laminoplasty versus anterior decompression. Spine 20: 1732-4.
- Minamide A, Yoshida M, Yamada H, et al. (2010) Clinical outcomes of microendoscopic decompression surgery for cervical myelopathy. Eur spine J Off Publ Eur Spine Soc Eur Spinal Deform Soc Eur Sect Cerv Spine Res Soc 19: 487-93.
- Peto I, Scheiwe C, Kogias E, Hubbe U (2017) Minimally Invasive Posterior Cervical Foraminotomy: Freiburg Experience With 34 Patients. Clin Spine Surg 30: E1419-25.
- Yabuki S, Kikuchi S (2008) Endoscopic surgery for cervical myelopathy due to calcification of the ligamentum flavum. J Spinal Disord Tech 21: 518-23.
- Eicker SO, Klingenhöfer M, Stummer W, Steiger H-J, Hänggi D (2012) Full-endoscopic cervical arcocristectomy for the treatment of spinal stenosis: results of a cadaver study. Eur Spine J 21: 2487-91.
- Amaral SH, Silva MN, Giraldi M, Viterbo MBS, Pereira CAB (2007) Multiple cervical arcocristectomies for the treatment of cervical spondylotic myelopathy: surgical technique and results. J Neurosurg Spine 7: 503-8.
- Law MDJ, Bernhardt M, White AA (1993) 3rd. Cervical spondylotic myelopathy: a review of surgical indications and decision making. Yale J Biol Med 66: 165-77.
- Kohno K, Kumon Y, Oka Y, Matsui S, Ohue S, Sakaki S (1997) Evaluation of prognostic factors following expansive laminoplasty for cervical spinal stenotic myelopathy. Surg Neurol 48: 237-45.
- Maeda T, Arizono T, Saito T, Iwamoto Y (2002) Cervical Alignment, Range of Motion, and Instability After Cervical Laminoplasty. Clin Orthop Relat Res 401: 132-8.
- Spetzger U, Bertalanffy H, Naujokat C, et al. (1997) Unilateral laminotomy for bilateral decompression of lumbar spinal stenosis. Part I: Anatomical and surgical considerations. Acta Neurochir (Wien) 139: 392-6.
- Palmer S, Turner R, Palmer R (2002) Bilateral decompressive surgery in lumbar spinal stenosis associated with spondylolisthesis: unilateral approach and use of a microscope and tubular retractor system. Neurosurg Focus 13: E4.
- Abbas SF, Spurgas MP, Szewczyk BS, et al. (2016) A comparison of minimally invasive posterior cervical decompression and open anterior cervical decompression and instrumented fusion in the surgical management of degenerative cervical myelopathy.Neurosurg Focus 40: E7.
- Hur JW, Kim JS, Shin MH, et al. (2014) Minimally invasive posterior cervical decompression using tubular retractor: The technical note and early clinical outcome.Surg Neurol Int 5: 34.
- Mielke D, Rohde V (2015) Bilateral spinal canal decompression via hemilaminectomy in cervical spondylotic myelopathy. Acta Neurochir 157: 1813-7.
- Hernández-Durán S, Zafar N, Behme D, Momber M, Rohde V, Mielke D, Fiss I (2020) Volumetric analysis of bilateral spinal canal decompression via hemilaminectomy versus laminoplasty in cervical spondylotic myelopathy. Acta Neurochir (Wien) 162: 2069-74.
FIGURE 1
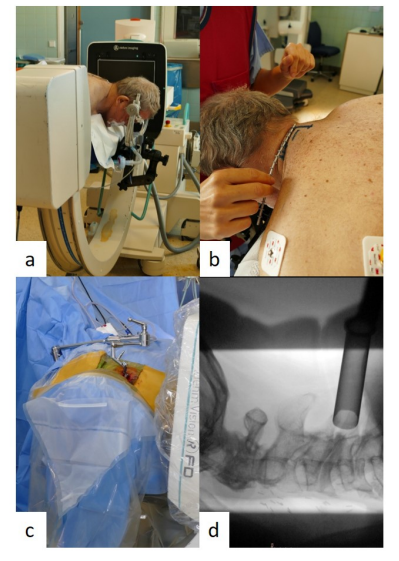
Figure 1: Positioning of the patient (a), marking of the skin incision (b), lateral fluoroscopy after tube insertion (c), verification of the correct tube position (d)
FIGURE 2
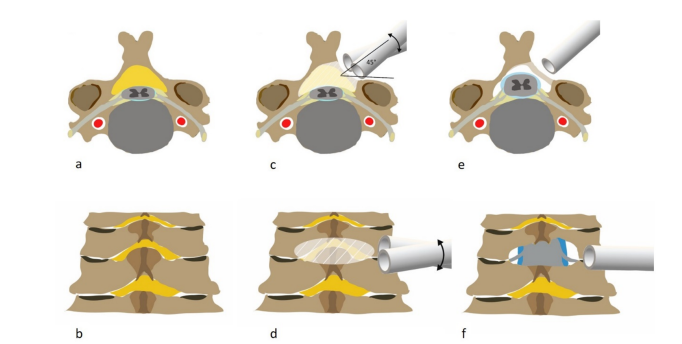
Figure 2: Posterior cervical stenosis in axial view (a). Posterior view of the cervical spine (b). Pivoting of the tubular system in axial and posterior views (c and d). The margins of bony resection are marked. Postoperative results in axial (e) and posterior (f) views, with sufficient decompression (the posterior tension band is preserved but is not illustrated for better visualization)
FIGURE 3
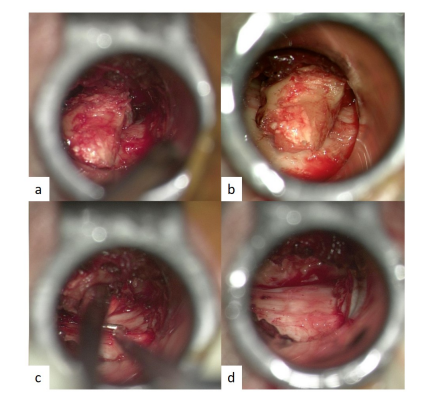
Figure 3: View through the tubular system under magnification. Results after ipsi and contralateral bony decompression (a and b). Palpation with microinstruments to assure sufficient decompression (c). Contralateral view on the decompressed dura (d)
FIGURE 4
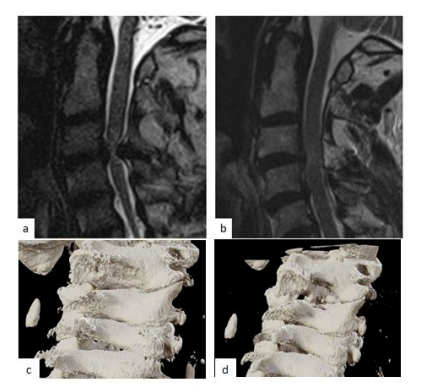
Figure 4: (a) Pre and postoperative (b) magnet resonance imaging in sagittal view and 3d reconstruction of the bony structures pre- (c) and postoperative (d) (Brainlab Iplan)
Tables at a glance
Figures at a glance