Co-existence of Papillary Thyroid Carcinoma and B Cell Lymphoma in Hashimoto`s Thyroiditis. Our approach from the Diagnosis to the Treatment
Received Date: March 01, 2024 Accepted Date: April 01, 2024 Published Date: April 04, 2024
doi: 10.17303/jspcr.2024.6.101
Citation: Daniela Xhemalaj, Eriselda Bashari (Kurushi), Elona Xhardo, Elida Mata, Marina Parllaku et al. (2024) Co-existence of Papillary Thyroid Carcinoma and B Cell Lymphoma in Hashimoto`s Thyroiditis. Our approach from the Diagnosis to the Treatment. J Surg Proce Case Rep 6: 1-6
Abstract
Papillary thyroid carcinoma (PTC) is the most common type of thyroid cancer, whereas primary thyroid lymphoma (PTL) is a rare disease, accounting for 2% to 5% of all thyroid malignancies. Despite several cases in which both PTC and PTL arise in the setting of Hashimoto’s thyroiditis (HT), the coexistence of both tumors in HT patients is very rare.
We describe a case of 75 years old -female with thyroid enlargement. Thyroid ultrasonography demonstrated an increased growth of hypoechogene nodule in the left lobe measuring 38x33 mm. A fine-needle aspiration (FNA) biopsy revealed atypical follicular epithelial cells (Bethesda system category IV /THYR-4). A total thyroidectomy was performed, that found to have concomitant papillary carcinoma and B-Cell Lymphoma in the background of Hashimoto`s Thyroiditis.
For the diagnostic workup and optional management of this rare coexistence, a multidisciplinary approach and close surveillance was needed.
Keywords: Primary Lymphoma; Hashimoto`s Thyroiditis; Papillary Carcinoma; Papillary Thyroid Carcinoma; Thyroid Ultrasonography
Introduction
Primary thyroid lymphoma (PTL) is a rare tumor accounting only about 1% to 5% of thyroid malignant tumors [1,2] or 2 cases per million [3]. PTL is more frequent in women than men, with the ratio of occurrence ranging from 2:1 to 8:1 [4,5] and is strongly associated with Hashimoto’s thyroiditis [6].
Papillary thyroid carcinoma (PTC) is the most common type of thyroid cancer, and its incidence has been increasing in the last few decades, with a large prevalence of small tumors [7].
PTC in patients affected by Hashimoto’s thyroiditis (HT) is a well-known event reported by literature [8]. PTC occurs mainly in women, accounts approximately 70% to 80% of all thyroid carcinomas and has an excellent prognosis [9].
The co-existence of PTC and PTL in the same patient is rare, and the present case report aims to describe the co-existence of PTC with B-Cell Lymphoma in a background of Hashimoto’s thyroiditis. Treatment and follow-up issues are also addressed.
Case Report
Here, we describe the case of a 75-year-old woman, with no family history of thyroid cancer, she referred recent painless enlargement in the left anterior side of the neck, complaining of mild and intermittent dysphagia to solid foods, she denied any voice change or dyspnea, while physical examination demonstrated an enlarged thyroid gland with a palpable, firm nodular lesion in the left lobe, moving with deglutition. She did not complain before, for thyroid disease.
Thyroid ultrasonography (US) demonstrated the growth of a hypoechogene nodule in the left lobe, measuring 38x33 mm.
Her serological tests at the admission were as following (Table 1):
US-guided fine needle aspiration (FNA) of the left -sided nodule and cytological examination revealed atypical epithelial cells concluding for indeterminate lesion (Bethesda System Category IV /THYR4).The patient underwent total thyroidectomy. Macroscopic examination revealed right thyroid lobe 11x6x5 cm, with multinodular nodules. Left thyroid lobe: 10 x5x3 cm, with a whitish nodule 33 mm.
Histology revealed thyroid follicles surrounded by aggregates of lymphoid infiltrates with germinal centers consistent with Hashimoto`s thyroiditis, diffuse monotonous lymphoid infiltrates with irregular nuclei, condensed chromatin and small nucleoli suggestive for Non Hodgkin Lymphoma. Immunohistochemistry showed immunoreactivity for CD 45, CD 20, CD79a,Bcl-6,PAX-5,of these cells, Ki-67-60%. Moreover, papillary carcinoma, folicular variant was discovered (Figure 1).
HPF-High Power Field
Hematological parameters were within the normal limits, hence, the final diagnosis of HT coexisting with papillary carcinoma and primary NHL (B-cell lineage) was made.
The patient was then treated with chemotherapy for the PTL, after she undergo radioactive iodine treatment for the PTC according to the guidelines [10].
In our knowledge, this is the first case of an Albanian patient diagnosed with the co-existing PTC and PTL in Hashimoto`s Thyroiditis.
The patient 5 weeks after surgery, TSH and Anti TG resulted respectively 69 mlU/L and 78mlU/L. In the scintigraphy there was minimal fixation in thyroid lodge. Iodine radioactive 100 mci and suppressive therapy with Levothyroxine 150 mcg/day was done in our case.
There is no need for calcium exogene. The chemotherapy consisted in six cycles of R-CHOP (rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone).
Discussion
Multiple primary cancers diagnosis is based on the international standards developed by Warren and Gates in 1932 [11].
Most of the HT patients, where thyroid architecture is usually altered by the chronic inflammation, can develop PTC which could be explained with the progressive rise in TSH levels caused by long-standing thyroiditis. TSH is a known growth factor for thyroid nodules [12,13].
On the other hand, several other papers report a better prognosis for PTC if it co-occurs with HT, which somehow could play a protective role against the aggressiveness of neoplasia: thyroid peroxidase antibodies (TPOAb) could probably drive a cytotoxic response against the inflammation [14,15]. Most of these lesions are detected incidentally suggesting the requirement of a routine follow-up in HT patients [16]. According to some studies, FNA has a sensitivity of > 90% in detecting these lesions [16,17]. FNA is the procedure of choice for evaluating thyroid nodules and selecting candidates for surgery [18]. In our case FNA showed an epithelial neoplasia.
HT, is also a risk factor for PTL, due to chronic antigenic stimulation of the lymphocytes in the setting of autoimmune thyroiditis predisposes the normal cells to lymphomatous transformation and further to a lymphoid malignancy and some alterations of some oncogenes like RET/PTC, which might regulate the early stages of tumor development; however many steps of oncogenic transformation are probably unknown [19].
Usually, the onset of PTL happens many years after the diagnosis of HT, but Watanabe et al. reported some cases of PTL discovered on average 18 months after the diagnosis of HT [20].
Approximately two-thirds of patients with co-existing PTL and PTC with HT were Non-Hodgkin B-cell lymphomas followed by MALT-Lymphoma and Small Lymphocytic Lymphoma [21].
The main treatment for PTC is surgery, but a comprehensive treatment strategy is needed for coexisting PTL and PTC. Some studies suggest that surgical resection, radiotherapy, and combined chemotherapy may be important factors in improving the prognosis of these patients [22]. Our patient after surgery and radioactive iodine therapy underwent chemotherapy.
Conclusion
Our case highlights the importance of regular follow-up in order to reach an early diagnosis: in particular, a sudden thyroid enlargement in elder patients with HT should lead physicians to consider PTC/PTL in the differential diagnosis.
Declaration of Conflicting Interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
- Camera A, Magri F, Fonte R, et al. (2010) Burkittlike lymphoma infiltrating a hyperfunctioning thyroid adenoma and presenting as a hot nodule. Thyroid, 20: 1033-6.
- Kalinyak JE, Kong CS and McDougall IR (2006) Burkitt’s lymphoma presenting as a rapidly growing thyroid mass. Thyroid, 16: 1053.
- Cheng V, Brainard J, Nasr C (2012) Co-occurrence of papillary thyroid carcinoma and primary lymphoma of the thyroid in a patient with long-standing Hashimoto’s thyroiditis. Thyroid, 22: 647-50.
- Thieblemont C, Mayer A, Dumontet C, et al. (2002) Primary thyroid lymphoma is a heterogeneous disease. J Clin Endocrinol Metab, 87: 105-11.
- Derringer GA, Thompson LD, Frommelt RA, et al. (2000) Malignant lymphoma of the thyroid gland: a clinicopathologic study of 108 cases. Am J Surg Pathol, 24: 623-39.
- Holm LE, Blomgren H, Lo whagen T (1985) Cancer risks in patients with chronic lymphocytic thyroiditis. New Engl J Med, 312: 601-4
- Siegel R, Naishadham D, Jemal A (2013) Cancer statistics, 2013. CA Cancer J Clin, 63: 11-30.
- Lee JH, Kim Y, Choi JW, Kim YS (2013) The association between papillary thyroid carcinoma and histologically proven Hashimoto’s thyroiditis: a meta-analysis. Eur J Endocrinol, 168: 343-9.
- Repplinger D, Bargren A, Zhang Y-W, et al. (2008) Is Hashimoto’s thyroiditis a risk factor for papillary thyroid cancer? J Surg Res, 150: 49-52.
- American Thyroid Association (ATA) (2009) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer, Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid, 19: 1167-214
- Shields W and Olive G (1932) Multiple primary malignant tumors: a survey of the literature and a statistical study. Am J cancer, 16: 1358-1414
- Banu DG, Mustafa OG, Karamanoglu Z (2004) Primary thyroid lymphoma arising in the setting of Hashimotos thyroiditis. Turk J Med Sci, 34: 395-8.
- Singh B, Shaha AR, Trivedi H, Carew JF, Poluri A, Shah JP (1999) Coexistent Hashimoto’s thyroiditis with papillary thyroid carcinoma: Impact on presentation, management, and outcome. Surgery, 126: 1070-6
- Zhang Y, Dai J, Wu T, Yang N, Yin Z (2014) The study of the coexistence of Hashimoto’s thyroiditis with papillary thyroid carcinoma. J Cancer Res Clin Oncol, 140: 1021-6.
- Azizi G, Keller JM, Lewis M, Piper K, Puett D, Rivenbark KM, et al. (2014) Association of Hashimoto’s thyroiditis with thyroid cancer. Endocr Relat Cancer, 21: 845-52.
- Cheng V, Brainard J, Nasr C (2012) Co occurrence of papillary thyroid carcinoma and primary lymphoma of the thyroid in a patient with long standing Hashimoto’s thyroiditis. Thyroid, 22: 647-50
- Melo GM, Sguilar DA, Petiti CM, Eichstaedt AG, Caiado RR, Souza RA (2010) Concomitant thyroid Malt lymphoma and papillary thyroid carcinoma. Arq Bras Endocrinol Metabol, 54: 425-8.
- Mazokopakis EE, Tzortzinis AA, Dalieraki Ott EI, Tsartsalis AN, Syros PK, Karefilakis CM, et al. (2010) Coexistence of Hashimoto’s thyroiditis with papillary thyroid carcinoma. A retrospective study. Hormones (Athens) 9: 312-7.
- Takakuwa T, Miyauchi A, Aozasa K (2009) Aberrant somatic hypermutations in thyroid lymphomas. Leuk Res, 33: 649-54
- Watanabe N, Noh JY, Narimatsu H, Takeuchi K, Yamaguchi T, Kameyama K, et al. (2011) Clinicopathological features of 171 cases of primary thyroid lymphoma: a longterm study involving 24553 patients with Hashimoto’s disease. Br J Haematol, 153: 236-43
- Ali SZ, Cibas ES (2010) The Bethesda System for Reporting Thyroid Cytopathology: Definitions, Criteria and Explanatory Notes. US: Springer.
- Deepti V, Vandana P, Shilpi A, et al. (2014) Primary thyroid lymphoma: a rare disease. J Cytol, 31: 218-20.
FIGURE 1
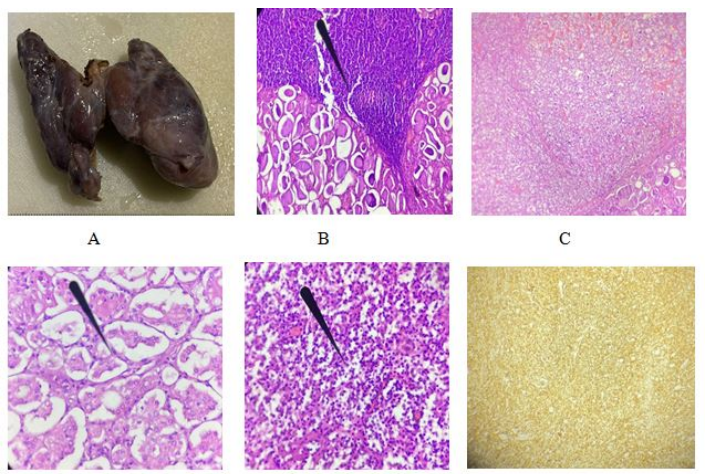
Figure 1: (A-macroscopic examination,B-Hematoxylin-Eosin staining showing Hashimoto`s tiroiditis, C-Papillary thyroid carcinoma/ H-E x10HPF,D-PTC follicular variant with nuclear features /H-Ex20HPF,E-B-Cell Lymphoma, F-CD20 + in immune cells).
Tables at a glance
Figures at a glance