Evaluation of Clinical and Imaging Findings in a Patient Diagnosed with Breast Schwannoma: A Case Report
Received Date: March 01, 2024 Accepted Date: April 01, 2024 Published Date: April 04, 2024
doi: 10.17303/jspcr.2024.6.102
Citation: Halit Ozgul, Remzi Can Cakir, Omer Celik, Emre Atmaca (2024) Evaluation of Clinical and Imaging Findings in a Patient Diagnosed with Breast Schwannoma: A Case Report. J Surg Proce Case Rep 6: 1-6
Abstract
Introduction: Schwannoma is a benign neoplasm of the peripheral nerve sheath. It typically develops in the head, neck, and extremities. The breast is a rare site of schwannoma occurrence.
Case Report: A 39-year-old female patient presented to our clinic with complaints of pain and palpable hardness in the left breast. Ultrasound examination revealed a well-circumscribed, oval lesion containing cystic areas. According to the biopsy, there were vascular structures within the slightly cellular fibrolipomatous stroma. A 13x28-mm, well-circumscribed, oval opacity was detected in the mammography. On magnetic resonance imaging, there was a well-circumscribed, round lesion in the left breast (BI-RADS category 4a findings). In the second biopsy, although it was considered that there might be neoplasia of neural origin, the total excision of the described lesion was recommended for a definitive/differential diagnosis. The mass was completely excised. The diagnosis of breast schwannoma was confirmed by histopathological examination.
Discussion: The clinical and pathological features of a schwannoma are similar to those of other benign tumors. Schwannoma was suspected based on the result of the second core biopsy
Conclusion: Although breast schwannomas are rare, they can be confused with cystic lesions in the breast.
Keywords: Schwannoma; Breast lesion; Cystic; Breast Pain
Introduction
A schwannoma, also known as neurilemmoma, neuroma, or neurinoma, is a benign neoplasm of Schwann cells in the peripheral nerve sheath [1,2]. It is a slow-growing tumor that generally affects young people and usually appears in the third decade of life [3]. Intramammary schwannomas constitute only 2.6% of all schwannomas [4]. Mammographically, they are identified as non-specific, well-defined, round or oval densities [5]. On ultrasound, they are reported as hypoechoic, well-defined masses [6]. Breast schwannomas do not have specific features on mammography or ultrasound. An excisional biopsy is required to differentiate a schwannoma from other lesions, including metaplastic carcinomas, fibroepithelial lesions, fibromatosis, and myofibroblastomas [7]. We aimed to conduct a literature review along with a rare case presentation of schwannoma, which can be mistaken for cystic lesions in the breast.
Case Report
A 39-year-old female patient who did not have any medical history or von Recklinghausen’s disease presented to our center with complaints of pain and palpable hardness in the left breast for the past six months. On physical examination, there was a palpable mass in the upper outer quadrant of the left breast. Ultrasound revealed a well-circumscribed, oval lesion containing cystic areas, measuring 15x22x26 mm in the upper inner quadrant of the left breast. Vascular structures were observed within the slightly cellular fibrolipomatous stroma in serial sections of the core biopsy. According to the mammography performed one year later, there was a 13x28-mm, well-circumscribed, oval opacity on left mediolateral radiography (Breast Imaging-Reporting and Data System [BI-RADS] category 4a findings) (Figure 1).
On magnetic resonance imaging, an 18x23-mm lesion was detected in the left breast, which was hypointense in the T1-weighted series (Figure 2) and hyperintense in the T2-weighted series (Figure 3). In the dynamic examination, there was a round lesion with smooth borders and intense heterogeneous contrast enhancement from the early period onwards (BI-RADS category 4a findings). In the second core biopsy, upon reviewing the histopathological findings and immunohistochemical and histochemical staining pattern together, it was considered that there might be a neoplasia of neural origin, but the total excision of the described lesion was recommended for a definitive/differential diagnosis. The mass was completely excised. In the detailed pathological examination, a nodular, smooth-surfaced, homogeneous mass lesion with a widest diameter of 2 cm was observed macroscopically in the sections of the sample. The microscopic examination of the lesion revealed a mesenchymal tumor consisting of spindle-ovoid cells containing mixed hypocellular and hypercellular areas, without apparent atypia or mitotic activity. Ancient changes, including myxoid change, hyalinization, old hemorrhage, and enlargement of the nuclei, were noted in the tumor. Immunohistochemically, S100 was diffusely strong, and CD34 was focally weakly positive in the cells. Desmin and actin were negative. The Ki-67 proliferation index was around 1-2%. The diagnosis of breast schwannoma was confirmed by histopathological examination (Figure 4).
Discussion
The clinical and radiological appearances of schwannomas are similar to those of benign tumors [8]. On ultrasonography, schwannomas are defined as solid and hypoechoic masses with variable degrees of posterior acoustic shadowing [9]. However, our patient’s ultrasound revealed a well-circumscribed, oval lesion containing cystic areas. The patient was followed up with a diagnosis of cystic disease in the breast. The mammographic findings of these tumors are usually defined as non-specific, appearing as round or oval densities, although some normal mammographic findings have also been described [8]. In our patient’s mammography, a well-circumscribed, oval opacity was observed.
BI-RADS evaluates breast schwannomas as category 4a lesions with a low risk of malignancy [10]. Therefore, schwannoma should also be considered in the presence of a palpable and painful breast mass with BI-RADS 4a lesions.
Uchida et al. described a well-circumscribed, hypoechoic mass with a large cystic area in the ultrasonography performed on a patient with breast schwannoma [11]. Ogose et al. reported that only 5/99 (5%) of patients with benign schwannomas experienced pain at rest, whereas 94/992 (95%) of patients with breast schwannomas had pressure-related pain [12]. Our patient’s primary complaint was pain in the breast. In young women who present with cystic lesions in the breast on ultrasound accompanied by pain, mammography or magnetic resonance imaging should be performed, considering the possibility of breast schwannoma.
In conclusion, although breast schwannomas are rare, they can be confused with cystic lesions in the breast.
Declarations of Interest
None
- TDN Ravelomihary, NNM Razafimanjato, L Nomenjanahary, AF Rakototiana, HJL Rakotovao, HN Rakoto-Ratsimba (2019) “Schwannoma of the breast: a report of rare location and a brief literature review,” Annals of Breast Surgery, 3: 17.
- QT Tan, EWL Chuwa, SH Chew, GS Hong (2014) “Schwannoma: an unexpected diagnosis from a breast lump,” J Surg Case Rep, 9: 085.
- Y Parikh, KJ Sharma, SJ Parikh, D Hall, (2016) “Intramammary schwannoma: a palpable breast mass,” Radiol Case Rep, 11: 129-33.
- TK Das Gupta, RD Brasfield, EW Strong, SI Hajdu (1969) “Benign solitary Schwannomas (neurilemomas).,” Cancer, 24: 355-66.
- KS Cho, HY Choi, SW Lee, SH Sung (2001) “Sonographic findings in solitary schwannoma of the breast,” J Clin Ultrasound, 29: 99-101.
- V Dialani, N Hines, Y Wang, P Slanetz (2011) “Breast schwannoma.,” Case Rep Med, 2011: 930841.
- Christopher DM Fletcher (2021) Tumors of the Peripheral Nervous System.
- T Fujii, R Yajima, H Morita, S Tsutsumi, T Asao, H Kuwano (2014) “A rare case of anterior chest wall schwannoma masquerading as a breast tumor.,” Int Surg, 99: 196-9.
- KK Yadav, N Poudel, K Acharya, RK Yadav, P Pathak, S Hirachan (2022) “Right breast schwannoma in a male: A rare case report,” Int J Surg Case Rep, 99: 107667.
- M Niknejad, Y Weerakkody (2010) “Breast imaging-reporting and data system (BI-RADS),” in Radiopaedia.org
- N Uchida, H Yokoo, H Kuwano (2005) “Schwannoma of the Breast: Report of a Case,” Surg Today, 35: 238-42.
- A Ogose et al. (1999) “Tumors of peripheral nerves: correlation of symptoms, clinical signs, imaging features, and histologic diagnosis,” Skeletal Radiol, 28: 183-8.
FIGURE 1
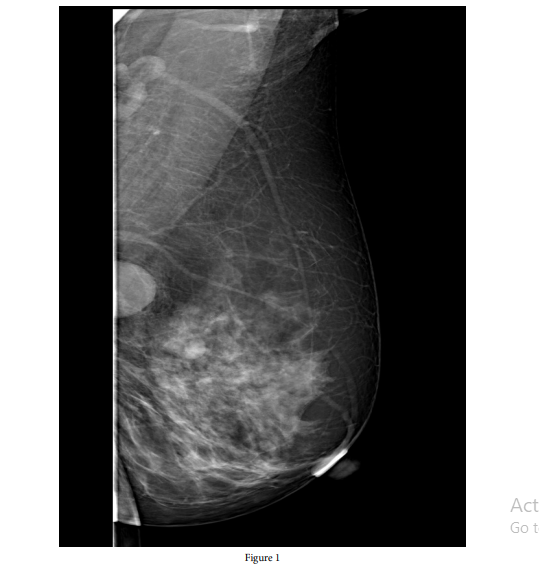
Figure 1:
FIGURE 2
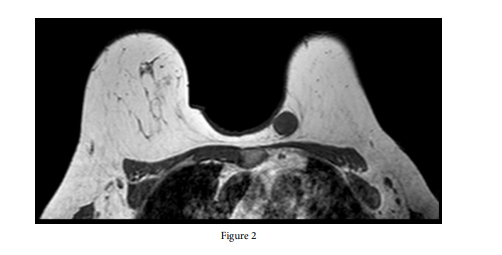
Figure 2:
FIGURE 3
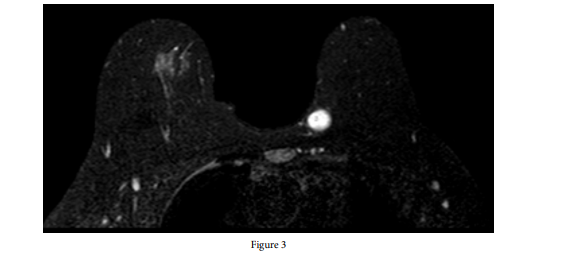
Figure 3:
FIGURE 4
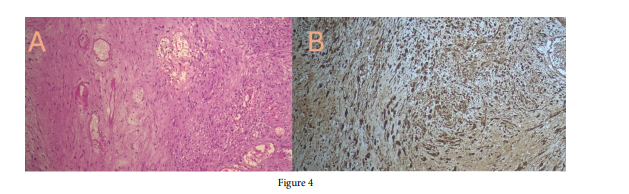
Figure 4:
Figures at a glance