Extra-Levator Abdomino-Perineal Resection, 10 years Tertiary Care Cener Experience: A Retrospective Cohort Study
Received Date: March 16, 2024 Accepted Date: April 16, 2024 Published Date: April 19, 2024
doi: 10.17303/jspcr.2024.6.103
Citation: Anwar Tawfik Amin, Ahmed Refaat Abd Elzaher, Ayatallah Ali Youssief Mohammed, Nayer NH Rizkallah, Abdallah M Taha et al. (2024) Extra-Levator Abdomino- Perineal Resection, 10 years Tertiary Care Cener Experience: A Retrospective Cohort Study. J Surg Proce Case Rep 6: 1-11
Abstract
Background: Total mesolectal excision (TME) is a standard component of oncological rectal cancer surgery. TME ensures adequate radial margin and reduces local recurrence rates. Abdominoperineal resection, low anterior resection and coloanal anastomosis using total mesorectal excision (TME) are the surgical options for treating rectal cancer. Abdominoperineal resection (APR) remains one of the gold standard surgical option for resection of low rectal cancers with curative intent; however, local recurrence rate remains high. Our oncological APR has included a tumor-specific, total meso-rectal (TME) with extra-levator excision EL-APR, including adequate perineal margins. We are auditing our standard tumor- specific, APR with TME extra-levator approach in term of oncological outcomes including local recurrence rates.
Methods: We did a retrospective review of all patients who underwent abdominoperineal resection from 2011 to 2021 at a single tertiary university oncology center, South Egypt cancer Institute. Our primary endpoint was local recurrence. Secondary endpoints included disease-free survival, overall survival and perioperative complications.
Results: There were 162 patients undergoing APR for rectal cancer identified with a mean follow-up of 33.8 months (range, 0 – 127), with 82% having undergone neoadjuvant therapy.
A laparoscopic approach was attempted in 35 (21%) cases with an overall conversion rate of 20% (7 cases).
Postoperative complications occurred in 25% (n=41) patients, with perineal wound complications most common (9%). Circumferential margins were positive in 9% of patients (14 cases). There were 28 deaths (17%) during follow-up and Kaplan-Meier analysis showed five-year overall survival of 72%. An R0 resection was completed in 136 patients (83%). Overall local recurrence rate was 4%. Of the R0 patients, two (1.5%) R0 patients had local recurrences and 8 (6.0%) R0 resection patients had distant recurrences. Kaplan-Meier analysis showed five-year disease-free survival of 84%.
Conclusions: EL-APR when performed as our standard method, excellent oncological outcomes with low local recurrence rates can be achieved.
Keywords: Rectal Cancer; Apdominoperineal Resection; Total Mesorectal Excision
Introduction
Colorectal cancer (CRC) does pose a significant threat to the health of global populations. Its incidence and mortality rates vary markedly around the world. Globally, CRC is the third most common cause of cancer worldwide, with almost 1.65 million new cases per year. It is the second most common cause of cancer deaths worldwide, with almost 835,000 deaths per year [1,39].
Colorectal cancer (CRC) is the fourth most frequently diagnosed cancer in the United States [1]. Management of rectal cancer has made significant oncologic advancements with the development of the total mesorectal excision (TME) and chemoradiation regimens, as well as reduced postoperative morbidity with the advent of minimally invasive approaches [2-7]. Additionally, improved imaging modalities such as MRI and PET-CT have improved pre-operative planning [8,9]. With these advancements have come a growing trend for sphincter-preserving procedures when possible. However, for certain patients, abdominoperineal resection (APR), a major operation that completely excises the distal colon, rectum and anal sphincter complex utilizing both an anterior abdominal and perineal approach, may be the best option [10].
Total mesorectal excision (TME) is a standard component of radical rectal cancer surgery. TME reduces the positive radial margin and local recurrence rates. Abdominoperineal resection, low anterior resection and coloanal anastomosis using total mesorectal excision (TME) are the surgical options for treating rectal cancer [1,38].
APR remains an important procedure in treating locally advanced and recurrent rectal cancers, especially for those with low-lying lesions or sphincter involvement [11]. In various registries, APR was the treatment of choice 25-50% of the time for patients diagnosed with rectal cancer [12,13]. Though the procedure was developed nearly a century ago and remains a therapeutic option today in the armament of colorectal surgeons, the APR has a significant risk of morbidity and mortality [11,14]. Furthermore, in spite of the radical resection of the tumor and surrounding tissue, risk for local recurrence following APR is reported to be approximately 10% and higher, with rates of 20-40% described as recently as the 1990’s [15-18]. The technical, surgeon-specific nature of APR makes it an operation that is ideally performed in high-volume centers [19].
Although the “cylindrical” or extra-levator APR (EL-APR) has been discussed recently, surgeons have been doing this for many years, and have considered this to be the conventional APR [20]. Thus, studies comparing conventional and cylindrical APR may send a conflicting message to some surgeons [21]. At our institution, as with many others, rather than the traditional approach of a formal “cylindrical APR,” a tumor-specific, extra-levator TME is performed, with particular focus on the appropriate perineal margins [22,23].
The aim of this work is to assess our standard tumor-specific, TME extra-levator APR (EL-AAR) in term of oncological outcomes including local recurrence rates.
Materials and Methods
After obtaining ethical Board approval, patients who underwent APR for rectal cancer from 2011-2021 at South Egypt cancer Institute have retrospectively been evaluated including tumors within 5 cm from the anal verge, tumors associated with lymphoid tissue, tumors with involved structures from within the deep pelvis, involvement of the external sphincter or invasion of the levator ani complex as well as those patients with poor baseline sphincter function with rectal cancer. Patients with no clear consent or no adequate follow up data have been excluded. The information retrieved included patients’ demographics, co-morbidities, and preoperative imaging. Perioperative parameters collected included surgical approach, intra-operative characteristics, operative time, and wound classification. Post-operative parameters collected included length of hospital stay, surgical complications and hospital death. Oncologic parameters collected included pathological grade and staging, histology, tumor size, pathologic margins and recurrence, adjuvant and neoadjuvant therapies.
The primary endpoint for this study was incidence of local recurrence. Secondary endpoints included pathological margins, disease-free survival (DFS), overall survival (OS), and incidence of recurrence as well as postoperative complications.
Operative Technique
The lithotomy is the standards position during our EL-APR surgery, a tumor-specific, extra-levator approach had been used for all cases and the inter-sphincteric approach had not been used for any cases. We specifically did use the extra-levator APR approach for low and ultra-low rectal tumors requiring APR, or when there was a concern for positive circumferential resection margin (CRM), involvement of the sphincters or involvement of the levators. A wider, tumor-specific perineal excision was even performed for tumors with extensive perineal involvement, fistulous disease or other concerns for a more extensive perineal tumor with higher risk of positive margins. In no cases were the levators closed, as the levators were always resected widely and did not permit closure.
Statistical Analysis
All statistical analyses were performed using STATA v.12 (STATA Corp., Texas, and USA). A p-value < 0.05 was considered significant. Categorical variables were presented as frequencies and percentages. Continuous variables are reported as means with ranges. Kaplan-Meier analysis was used to assess the local recurrence-free survival, DFS and OS.
Results
A total of 161 patients underwent APR for rectal cancer from 2011 to 2021. Patient demographics are reported in Table 1. Mean age was 43 years (range, 34 – 74) and 60% of the patients were male. Mean body mass index (BMI) was 29 kg/m2 (range, 19– 46 kg/m2). Of the co-morbidities, 51% had a history of smoking, 22% had diabetes and 6% had chronic obstructive pulmonary disease (COPD). CT was performed for local staging in 63% of patients. Neoadjuvant radiation was given to 83% of the patients and neoadjuvant chemotherapy was given to 82% of the patients. Postoperative adjuvant radiation was given to 10% of the patients and adjuvant chemotherapy was given to 44% of the patients.
Operative details are described in Table 2. Overall, an open surgical approach was utilized in 79% (n=127) of the cases and laparoscopic converted to open approach in 7 cases who were reported as open cases. 17.4% (n=28) of cases were completed laparoscopically. Mean operative time was 280 minutes (range, 145 – 347) and 60 minutes shorter in the laparoscopic group. Mean estimated blood loss was 300 mL (range, 100 – 2100). Multi-visceral resections were performed in 20% (n=32) of patients.
Post-operative parameters and complications are reported in Table 3. Mean LOS overall was 9 days (range, 3– 38). Overall complications included perineal wound infection or dehiscence (9%), thromboembolic events in 3% of patients and urinary tract infection (UTI) in 5%.
Oncologic details and follow-up data are shown in Table 4. Mean follow-up was 33.8 months (range, 3 – 117. Mean tumor size was 3.2 cm (range, 0.3 – 10). Tumors were a mean of 4.8 cm (range, 0.9 – 24) from the anal verge. The post-resection CRM was positive in 14 (8.6%) patients, with 3 10.7%) CRM-positive patients in the laparoscopic group and 11 (8.2%) in the open group with no significant difference (P = 0.42). Negative margins had a mean CRM distance of 7.0 mm (range, 3.0 – 25.0 mm).
An R0 resection was completed in 136 (84%) patients, 14 (8.5%) patients underwent an R1 resection and 12 (7.5%) underwent an R2 resection. Of patients undergoing curative R0 resection, two patients (1.5%) had local recurrences (Figure 1), 8 patients had distant recurrences (6.0 %) and Kaplan-Meier analysis showed five-year DFS of 73%. There were 28 deaths (17.2%) during follow-up with a fiveyear OS of 84% on Kaplan-Meier analysis (Figure 2). In terms of surgical approach, OS was significantly decreased for patients who underwent an open approach than a laparoscopic approach (P = 0.01). However, there was no significant difference in DFS and local recurrence between an open approach and laparoscopic approach (P > 0.05).
Discussion
In this study, our aim was to assess the oncologic outcomes after a conventional, but tumor-specific, extra-levator excision (EL-APR) that includes appropriate perineal margins. Over the course of a decade, we have demonstrated excellent outcomes after APR in a large single-center study. The results show an overall local recurrence rate of 2.5% which decreases to 1.5% in patients who underwent an R0 resection. Five-year DFS was 73% for patients who underwent an R0 resection and five-year OS was 84%. The focus of this paper was not to directly compare laparoscopic and open approaches, as they were complimentary in this population of patients of whom not all were appropriate for a laparoscopic approach given the need for multi-visceral resection. However, we did find that the laparoscopic approach was associated with higher OS without affecting DFS or local recurrence rates for those who underwent an R0 resection.
APR remains a necessary approach in low rectal cancer when anterior resection does not offer a safe oncologic outcome. The development of the TME has played an important role in the surgical management of rectal cancer, decreasing the rate of local recurrence and increasing overall survival [26,27]. Nevertheless, APR inferiority in comparison to anterior resection with regard to CRM involvement, local recurrence and poor prognosis has motivated surgeons to improve upon the APR technique [17,28].
Although the concept of an extra-levator APR or abdominoperineal excision (EL-APE) has been described by Holm et al. as a technique to reduce CRM involvement by tumor and bowel perforation, this operation has been performed by many surgeons for generations and simply called an APR.[29] Indeed, excitement for EL-APE has been tempered by multiple meta-analyses with different conclusions. In agreement with Holm et al., Stelzner et al. and Yu et al. reported superior local recurrence rates and lower positive CRMs following ELAPE compared to standard APR [29-31]. However, Zhou et al. and Krishna et al. concluded there was no significant difference in negative CRM and Prytz et al. even found increased risk of local recurrence in ELAPE [32-34].
We believe the discrepancy in these reports is that some surgeons perform a technically adequate APR which they call “conventional”, and some surgeons do not. Thus, as with any operation, one must do it properly. The tailored approach utilized by the authors in this report resulted in 9% of patients with a positive CRM which is comparable to reported rates of 4 – 21% seen in recent literature [33]. Our 4% overall local recurrence rate, and 1.5% local recurrence rate for patients who underwent R0 resection is significantly lower than the 7-10% reported by the meta-analyses in the literature [30,35]. We believe this to be the result of careful focus on doing a tumor-specific extra-levator APR, with wide perineal excision when required, and always avoiding an inter-sphinteric approach for cancer cases. Our low rate of CRM positivity, local recurrence and DFS regardless of surgical approach confirms that laparoscopy should have a role in APR given proper patient selection and adequate laparoscopic experience.
Conventional APR can achieve excellent oncological outcomes based on pathological parameters, low local recurrence rates, and overall survival. Great care needs to be paid to performing a tumor-specific, extra-levator operation, and paying attention to circumferential margins during pre-operative planning and surgery. Laparoscopy with the appropriate patient in the hands of the experienced laparoscopic surgeon is not a contraindication oncologically and should reduce morbidity and mortality. Continued follow-up of these patients will provide an even more robust understanding for the results of APR with a selective perineal approach.
- American Cancer Society (2011) Colorectal Cancer Facts and Figure 2017-2019. Color Cancer.
- Marco Milone, Michele Manigrasso, Morena (2015) Rectal cancer—state of art of laparoscopic versus open surgery Ann Laparosc Endosc Surg, 2:147.
- Joep Knol, Deborah S. Keller (2020) Total Mesorectal Excision Technique—Past, Present, and Future Clin Colon Rectal Surg, 33: 134-43.
- Shahab Hajibandeh, Shahin Hajibandeh, Joseph Matthews, Lucy Palmer, Andrew Maw (2020) Meta-analysis of survival and functional outcomes after total mesorectal excision with or without lateral pelvic lymph node dissection in rectal cancer surgery Surgery, 168: 486-96.
- Hong KD, Kang S, Urn JW, Lee S Il (2015) Transanal Minimally Invasive Surgery (TAMIS) for Rectal Lesions: A Systematic Review. Hepatogastroenterology, 62: 863-7.
- Xiaoqiang Xue, Guole Lin (2022) Transanal endoscopic microsurgery: exploring its indications and novel applications. A narrative review Wideochir Inne Tech Maloinwazyjne, 17: 95-103
- Sauer R, Becker H, Hohenberger W, Rödel C, Wittekind C, et al. (2004) Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med, 351:1731-40.
- Kim NK, Kim MJ, Yun SH, Sohn SK, Min JS (1999) Comparative study of transrectal ultrasonography, pelvic computerized tomography, and magnetic resonance imaging in preoperative staging of rectal cancer. Dis Colon Rectum, 42: 770-5.
- Drew PJ, Farouk R, Turnbull LW, Ward SC, Hartley JE, Monson JRT (1999) Preoperative magnetic resonance staging of rectal cancer with an endorectal coil and dynamic gadolinium enhancement. Br J Surg, 86: 250-4.
- Alteri R, Bandi P, Brooks D, Cokkinides V, Doroshenk M, Gansler T, Graves K, Jacobs E, Kirkland D, Kramer J, Levin B, Magro A, McCullough M, Na D, Wagner D (2011) Colorectal Cancer Facts & Figures 2011-2013. Am Cancer Soc 2011. doi: 10.1038/nrgastro.2011.208
- Perry WB, Connaughton JC (2007) Abdominoperineal resection: How is it done and what are the results? Clin Colon Rectal Surg, 20: 213-20.
- Nilsson PJ (2006) Omentoplasty in abdominoperineal resection: A review of the literature using a systematic approach. Dis Colon Rectum, 49:1354-61.
- Schoetz DJ (2006) Evolving Practice Patterns in Colon and Rectal Surgery. J Am Coll Surg 203: 322-7.
- Marcel den Dulk, Corrie A. M. Marijnen, Hein Putter, Harm J. T. Rutten ,§ Geerard L. Beets,Theo Wiggers, Iris D. Nagtegaal, Cornelis J. H. van de Velde. Risk Factors for Adverse Outcome in Patients With RectalCancer Treated With an Abdominoperineal Resection in the Total Mesorectal Excision Trial, Ann Surg, 246: 83-90.
- McCall JL, Cox MR, Wattchow DA (1995) Analysis of local recurrence rates after surgery alone for rectal cancer. Int J Colorectal Dis, 10: 126-32.
- den Dulk M, Putter H, Collette L, Marijnen CM, Folkesson J, et al. (2009) The abdominoperineal resection itself is associated with an adverse outcome: The European experience based on a pooled analysis of five European randomised clinical trials on rectal cancer. Eur J Cancer, 45: 1175-83.
- Marr R, Birbeck K, Garvican J, Macklin CP, Tiffin NJ, et al. (2005) The modern abdominoperineal excision: the next challenge after total mesorectal excision. Ann Surg, 242: 74-82.
- Heald RJ, Smedh RK, Kald A, Sexton R, Moran BJ (1997) Abdominoperineal excision of the rectum--an endangered operation. Norman Nigro Lectureship. Dis Colon Rectum, 40: 747-51.
- Holm T, Johansson H, Cedermark B, Ekelund G, Rutqvist LE (1997) Influence of hospital- and surgeon-related factors on outcome after treatment of rectal cancer with or without preoperative radiotherapy. Br J Surg, 84: 657-63.
- Holm T (2014) Controversies in abdominoperineal excision. Surg Oncol Clin N Am, 23: 93-111
- Han JG, Wang ZJ, Wei GH, Gao ZG, Yang Y, Zhao BC (2012) Randomized clinical trial of conventional versus cylindrical abdominoperineal resection for locally advanced lower rectal cancer. Am J Surg, 204: 274-82.
- Keller DS, Lawrence JK, Delaney CP (2014) Prone jackknife position is not necessary to achieve a cylindrical abdominoperineal resection: demonstration of the lithotomy position. Dis Colon Rectum, 57: 251.
- DLH Baird, C Simillis, C Kontovounisios, Q Sheng, S Nikolaou, WL Law, et al. (2017) A systematic review of transabdominal levator division during abdominoperineal excision of the rectum (APER. Tech Coloproctol, 21: 701-7.)
- Williams CP, Reynolds HL, Delaney CP, Champagne B, Obias V, Joh YG, Merlino J, Kinsella TJ (2008) Clinical results of intraoperative radiation therapy for patients with locally recurrent and advanced tumors having colorectal involvement. Am J Surg, 195: 405-9.
- Brady JT, Crawshaw BP, Murrell B, Dosokey EMG, Jabir MA, Steele SR, et al. (2017) Influence of intraoperative radiation therapy on locally advanced and recurrent colorectal tumors: A 16-year experience. Am J Surg.
- Heald RJ, Husband EM, Ryall RD (1982) The mesorectum in rectal cancer surgery--the clue to pelvic recurrence? Br J Surg, 69: 61-6.
- Martling A, Holm T, Rutqvist LE, Johansson H, Moran BJ, et al. (2005) Impact of a surgical training programme on rectal cancer outcomes in Stockholm. Br J Surg, 92: 225-9.
- Nagtegaal ID, van de Velde CJH, Marijnen CM, van Krieken JHJM, Quirke P (2005) Low rectal cancer: a call for a change of approach in abdominoperineal resection. J Clin Oncol, 23: 9257-64.
- Holm T, Ljung A, Häggmark T, Jurell G, Lagergren J (2007) Extended abdominoperineal resection with gluteus maximus flap reconstruction of the pelvic floor for rectal cancer. Br J Surg, 94: 232-8.
- Stelzner S, Koehler C, Stelzer J, Sims A, Witzigmann H (2011) Extended abdominoperineal excision vs. standard abdominoperineal excision in rectal cancer-a systematic overview. Int J Colorectal Dis, 26:1227-40.
- Yu H-C, Peng H, He X-S, Zhao R-S (2014) Comparison of short- and long-term outcomes after extralevator abdominoperineal excision and standard abdominoperineal excision for rectal cancer: a systematic review and meta-analysis. Int J Colorectal Dis, 29: 183-91.
- Krishna A, Rickard MJFX, Keshava A, Dent OF, Chapuis PH (2013) A comparison of published rates of resection margin involvement and intra-operative perforation between standard and “cylindrical” abdominoperineal excision for low rectal cancer. Color Dis, 15: 57-65.
- Zhou X, Sun T, Xie H, Zhang Y, Zeng H, Fu W (2015) Extralevator abdominoperineal excision for low rectal cancer: A systematic review and meta-analysis of the short- -term outcome. Color Dis, 17:474-81.
- Prytz M, Angenete E, Bock D, Haglind E (2015) Extralevator Abdominoperineal Excision for Low Rectal Cancer—Extensive Surgery to be Used With Discretion Based on 3-Year Local Recurrence Results. Ann Surg 0: 1.
- Chen B, Yu PDZ, Ph D (2012) Enhanced Recovery After Surgery Programs Versus Traditional Care for Colorectal Surgery: A Meta- analysis of Randomized Controlled Trials, 667-78.
- Chuwa EWL, Seow-Choen F (2006) Outcomes for abdominoperineal resections are not worse than those of anterior resections. Dis Colon Rectum, 49: 41-9.
- Messenger DE, Cohen Z, Kirsch R, O’Connor BI, Victor JC, Huang H, McLeod RS (2011) Favorable pathologic and long-term outcomes from the conventional approach to abdominoperineal resection. Dis Colon Rectum, 54: 793-802.
- Beyond TME Collaborative (2013) Consensus statement on the multidisciplinary management of patients with recurrent and primary rectal cancer beyond total mesorectal excision planes. Br J Surg, 100: 1009-14.
- Fitzmaurice C, Allen C, Barber RM, Barregard L, Bhutta ZA, et al. (2017) Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups,1990 to 2015: a systematic analysis for the global burden of disease study. JAMA oncology, 3: 524-48.
FIGURE 1
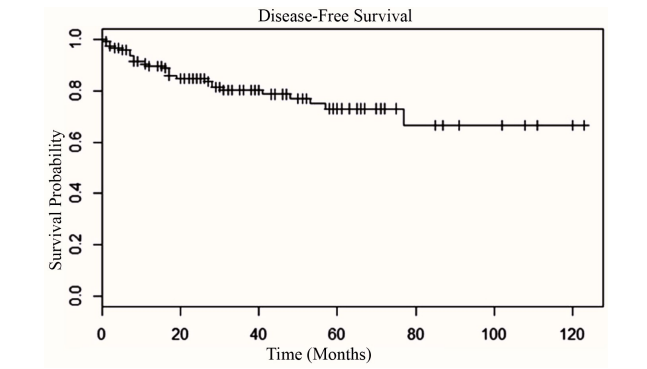
Figure 1: Kaplan-Meier curve and disease-free survival (5-year disease-free survival rate for patients with R0 resection=73%).
FIGURE 2
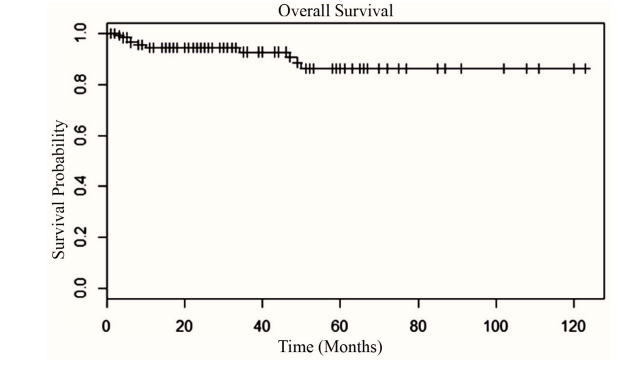
Figure 2: Kaplan-Meier Curve, Overall survival (5-year -Overall-Survival rate 84%). The 5-year -Overall-Survival rate 73%.
Tables at a glance
Figures at a glance