Performing a Transduodenal Ampullectomy in an Annular Pancreas Patient:Case Report
Received Date: March 24, 2024 Accepted Date: April 24, 2024 Published Date: April 27, 2024
doi: 10.17303/jspcr.2024.6.104
Citation: Daniel Eckhardt, Felix Huettner, Wolfram Schief, Markus Diener (2024) Performing a Transduodenal Ampullectomy in an Annular Pancreas Patient: Case Report. J Surg Proce Case Rep 6: 1-8
Abstract
Annular pancreas is a rare anomalia. It can be diagnosed via endoscopy, CT scan or MRI. Yet, there is no guideline offering strategies for treatment of symptomatic annuli or as complicative issue in biliopancreatic surgery. Reporting a case of a transduodenal ampullectomy of a low grade adenoma in the ampulla of Vater region, we try to figure out the treatment options of patients suffering that anomalia and giving advice on the surgical approach.
Keywords: Annular Pancreas; Anomalia; Endoscopy, CT Scan or MRI; Transduodenal Ampullectomy
Introduction
Symptoms of duodenal obstruction like abdominal pain, jaundice, vomiting of bileor ingested food and pancreatitis are the most common indications for surgery [1,2]. Noteworthy, most patients remain asymptomatic [3].
The ring is often located oral to the papilla of vater [4,5]. Annular pancreas can be classified in two subtypes: An intramural type draining directly into the duodenum and an extramural type draining via a ventral duct into a second duct [4,6,7]. The “annular duct” opens into the pancreatic duct (type I), to the common bile duct, fusioning with the wirsung`s duct (type II) or the wirsung`s duct being missed, to the Santorini`s duct [4,6,7].
Diagnosis, especially in symptomatic patients, can be made via endosonography, CT scan (so called “crocodile jaw” sign) or MRI [1,6]. These diagnostics are not only necessary to confirm expected diagnosis but also to exclude a pancreas divisum or the location of a minor papilla 5,8. Even endoscopic retrograde cholangiopancreaticscopy (ERCP) may be helpfull to distinguish the types of drainage [1,5]. Biopsies are not done routinely, but are performed if there is suspicion of malignancy [1,2]. Preoperative diagnosis is difficult, so exploration remains necessary in many cases to confirm annular pancreas – and to initiate treatment [4,5]. Larger samples of patients show higher incidences for pancreatobiliary malignancies [5].
However, to our knowledge there is no explicit recommendation on the exact location of the duodenotomy (oral, through or aboral to the annular pancreas) as different locations of papilla of vater in relation to the annular pancreas have been described [4-6]. Making the wrong decision on where to duodenotomize may complicate the ampullectomy.
Methods
We reviewed the literature using pubmed (https://pubmed.ncbi.nlm.nih.gov/) entering “annular pancreas”, “annular pancreas resection”, “annular pancreas types” as keywords. Approval from the patient was obtained after informed consent on surgery. Personal data were removed from all pictures.
Case Report
Reporting the case of an 84 years old male patient, called G. G., who was institutionalised to our hospital initially with symptomatic pancreatitis in November 2020. Evaluating Cholestasis via sonography our collegues performed endoscopic retrograde cholangioscopy trying to remove concrements from the hepatocholedochal duct (Figure 1). Surprisingly, they found an adenoma at the papilla of vater, being histopathologically staged as “low grade dysplasia”. The adenoma couldn´t be fully resected due to its localization up to 5mm into the bilde duct. Our collegues implanted a stent into the common bile duct.
Symptoms and cholestasis declined afterwards. We initiated a CT-scan to exclude metastasis or any further pathologies. As can be seen on the CT scan (Figure 2), there is a thin tissue surrounding the pars decendens duodeni oral to the papilla of vater. As we found no note of cancer, we decided to resect the ampulla transduodenally instead of a pylorus- preserving pancreatics head resection. The stent had been changed once prior to the resection.
In February 2021 the patient was planned for the transduodenal ampullectomy with simultaneously performed cholecystectomy. After laparotomy and mobilization of the right hemicolon the duodenum had been exposed. At that stage we could confirm the suspicious tissue within the CT-slices (pic. 2) to be part of an annular pancreas (Figure 3). Regarding the CT-scan the ampulla of vater is distal to the ring, but we couldn`t be sure about an additional duct or porus within the annular pancreas.
As mentioned in the literature review above, there is no prior description of an ampullectomy on an annular pancreas patient. Discussing the treatment options, we refused to perform pylorus-preserving pancreas head resection and staid with the decision to perform a transduodenal ampullectomy: After performing a duondenotomy distal to the annular pancreas, we uncovered the ampulla but were unable to identify the stent. We resected the distal duct due to the size of the adenoma. Rapid section examination found no incidence for malignoma or high-grade dysplasia. To be sure about stent dislocation and persisting concrements in the hepatocholedochal duct, cholangioscopy was performed. Some further concrements were removed without note for a foreign body. The oral duodenum had been explored as well to rule out a second duct draining the annular pancreas [4]. After reinsertion of the bile duct into the duodenum (Figure 4) surgery was completed. Documenting citrobacter and E. coli from ductal microbiological examination, antibiotics were infused in order to treat chronic cholangitis properly. 14 days after surgery G. G. was discharged from the hospital without complications during the postoperative course.
Relieving an abscess in the drainage channel two weeks afterwards by reopening the wound in the emergency ambulance, a minor complication could be treated without second operation.
On a telephone call three months after discharge the patient described himself in good condition, the reopened wound be almost entirely closed without an persisting secretion.
Discussion
Asymptomatic annular pancreas patients without suspion of malignancy need no treatment [1]. The same authors prefer laparoscopic duodenojejunostomy or gastrojejunostomy in symptomatic patients without indication for resection [1,9]. Even a duodenoduodenostomy is feasable [1,6]. Kobayashi et al. reported a case of a Japanese patient with an intraductal papillary mucinous neoplasm within the annulus and chose limited resection of the annular part of the pancreas [10].
Benassai et al. performed subtotal gastrectomy including the duodenal bulb and reconstruction by a Roux-Y procedure in a case where the annular pancreas encircled the duodenal bulb and the tissue had been suspicious of pancreatic cancer (UICC stage I; [4]). Foo et al. reported of several case series indicating pancreaticoduodenectomy, if biopsies revealed high- grade dysplasia [2].
Reviewing the available literature, we were unable to identify a single publication describing an appropriate surgical strategy for ampullary neoplasms in patients with annular pancreas. We demonstrated feasability of transduodenal ampullectomy in those patients.
In conclusion, we managed to make a proposal for treatment of annular pancreas and illness additional to that malformation, respectively: Asymptomatic patients shoud not be treated anyway [1], patients solely symptomatic from the annular pancreas without hints for malignancy could be treated via laparoscopic duodenoduodenotomy, duodenojejunostomy or gastrojejunostomy [4]. Transduodenal ampullectomy in patients with low grade dysplasia of the papilla of Vater and annular pancreas is feasable, yet 45-58% of cases after ampullectomy revealed to be invasive adenocarcinoma (false-negative preoperative staging [11,12]). Patients with suspicion of dysplasia or malignancy should undergo pancreaticoduodenectomy [2,12]: Patient with annular pancreas
Suspicious of Malignancy?
Patients with annular pancreas, whether known prior to surgery or not, should be diagnosed for malignancy. Patients with cancer or dysplasia should be resected according to pancreas cancer in the head [4,11,12]. Patients without cancer-like lesions, who expose no symptoms need no treatments while those suffering from duodenal obstruction or other diseases need specific treatment [6]: Duodenoduodenostomy, duodenojejunostomy or gastrojejunostomy for those with duodenal obstruction and transduodenal ampullectomy for those with obstruction of the ampulla of Vater.
This case report is limited by several aspects: First, this report describes just a single case in a retrospective mannor. Second, we didn`t establish a systematic follow-up as we called the patient three months after discharge to ask for his general health and possible additional complications after the ampullectomy. Further clinical data is necessary to strengthen the evidence of recommendations on the surgical approach of transduodenal ampullectomy in annular pancreas patients.
Acknowledgement
None
- Chittawadagi B et al. (2020) Laparoscopic Roux-en Y duodenojejunostomy: A safe and physiological treatment for symptomatic annular pancreas in adults. J Minim Access Surg, 16: 121-5.
- Foo FJ, Gill U, Verbeke CS, Guthrie JA, Menon KV (2007) Ampullary carcinoma associated with an annular pancreas. JOP, 8: 50-4.
- Jiménez-Romero C, Manrique A, Justo I (2017) Annular pancreas as graft for pancreas transplantation. Technical considerations and long-term follow-up of two successful cases. Transplant International, 30: 841-3.
- Benassai G et al. (2015) Ductal adenocarcinoma in anular pancreas. Int J Surg, 21: S95-97.
- Gromski MA et al. (2019) Annular pancreas: endoscopic and pancreatographic findings from a tertiary referral ERCP center. Gastrointestinal Endoscopy, 89: 322-8.
- Zheng HM, Cai XJ, Shen LG, Finley R (2007) Surgical treatment of annular pancreas in adults: a report. Chin Med J (Engl), 120: 724-5.
- De Rai P et al. (2010) Surgical management of acute pancreatitis in Italy: lessons from a prospective multicentre study. HPB, 12: 597-604.
- Sandrasegaran K, Patel A, Fogel EL, Zyromski NJ, Pitt HA (2009) Annular pancreas in adults. AJR Am J Roentgenol, 193: 455-60.
- Noh TH, Lee SE, Park JM (2012) Laparoscopic treatment of annular pancreas in adults: report of a case. Korean J Hepatobiliary Pancreat Surg, 16: 43.
- Kobayashi S, Kamohara Y, Nagata Y, Ito M, Fujioka H (2015) Intraductal papillary mucinous neoplasm in an annular pancreas: a case report. surg case rep, 1: 68.
- de Castro SMM et al. (2004) Surgical management of neoplasms of the ampulla of Vater: local resection or pancreatoduodenectomy and prognostic factors for survival. Surgery, 136: 994-1002.
- Bucher P, Chassot G, Durmishi Y, Ris F, Morel P (2007) Long-term results of surgical treatment of Vater’s ampulla neoplasms. Hepato gastroenterology, 54: 1239-42.
FIGURE 1
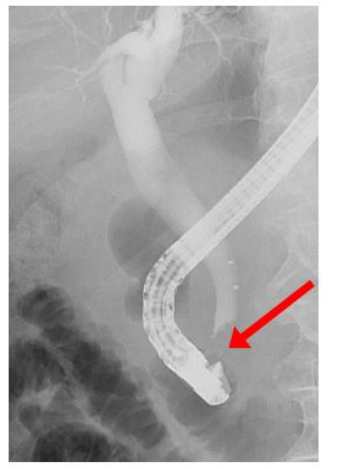
Figure 1: Endoscopic retrograde cholangioscopy
In the distal hepatocholedochal duct there seems to be a contrast media sparing concrement or adenoma (red arrow).
FIGURE 2
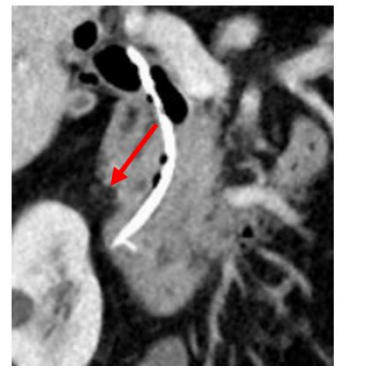
Figure 2: CT-Scan of the duodenal region
FIGURE 3
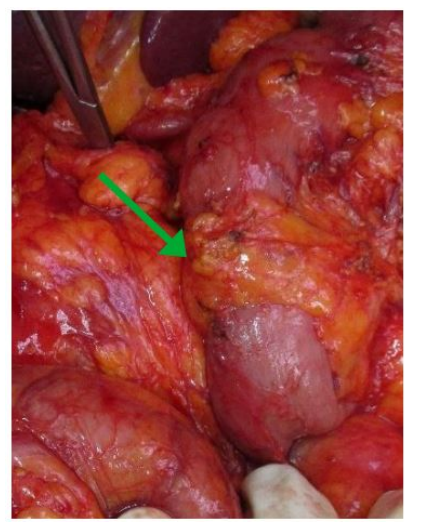
Figure 3: Intraoperative Picture of annular pancreas The descendent part of duodenum is totally encircled with pancreatic tissue (green arrow). Ampulla of vater has not been detectable.
FIGURE 4
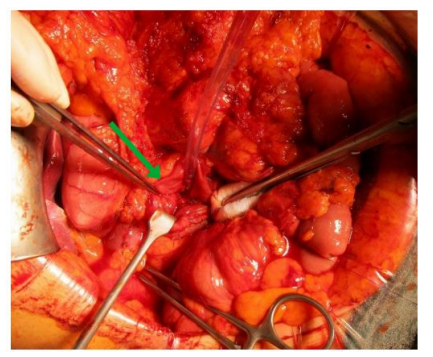
Figure 4: Photography of the ampulla of vater
In the center of the duodenotomy the ampulla has been exposed (green arrow). The adenoma is not shown.
FIGURE 5
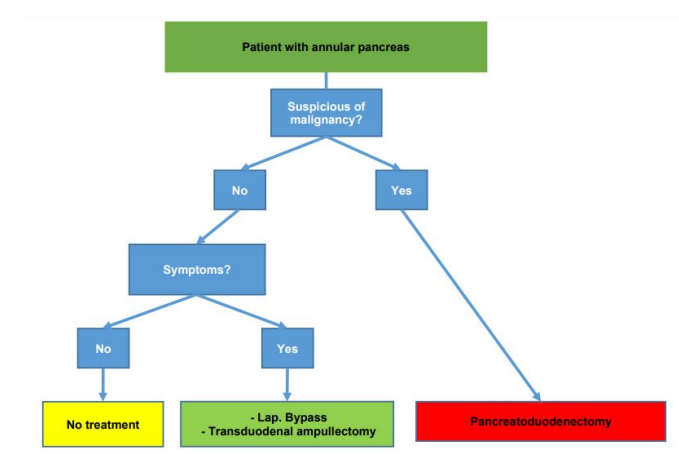
Figure 5: Treatment scheme for annular pancreas patients
Figures at a glance