Severe Contraction and Almost Complete Obliteration of the Urinary Bladder – Lessons Learnt in Management of Lower Urinary Tract Symptoms
Received Date: April 20, 2024 Accepted Date: May 20, 2024 Published Date: May 23, 2024
doi: 10.17303/jspcr.2024.6.105
Citation: Vivien Hsu, Katherine Ong, Stephen McCombie (2024) Severe Contraction and Almost Complete Obliteration of the Urinary Bladder – Lessons Learnt in Management of Lower Urinary Tract Symptoms. J Surg Proce Case Rep 6: 1-5
Abstract
Lower urinary tract symptoms (LUTS) can be debilitating and a life-long struggle for patients. Many conditions can cause LUTS and identifying the cause early can prevent irreversible changes to bladder capacity, compliance, and overall function. If a bladder becomes permanently damaged, treatment options are limited but the clinician must consider the patient’s quality of life. We present a case of a patient with a severely contracted and almost obliterated bladder, his management, and lessons we learnt along the way.
Keywords: Obliterated Bladder; Small Capacity Bladder; Contracted Bladder
Introduction
Lower urinary tract symptoms (LUTS) can be caused by many different conditions and depending on the pathophysiology, the structural composition of the bladder can vary [1]. These changes can sometimes be reversible but may become permanent over time with severe impacts on the patient’s quality of life [1]. In patients with bladder outflow obstruction, fibrosis can cause decreased bladder compliance and increase their risk of obstructive uropathy [2]. If patients then require long-term catheterisation, the bladder can then lose further compliance, contract, and lose a significant amount of bladder capacity [3]. These patients may then suffer from symptoms associated with small capacity bladders such as bladder spasm, pain, and bypassing of the catheter [3]. Once patients reach this point, it can be difficult to find a solution that improves their quality of life. Ideally, patients with LUTS should be recognized as early as possible to try to identify the underlying cause, treat the condition early and prevent irreversible changes to the bladder.
We present the case of a patient who developed a severely contracted and almost completely obliterated bladder, his management, and the lessons we learnt along the way.
Case Presentation
The patient is an 80-year-old male, with his medical history including type two diabetes mellitus, bronchiectasis, atrial fibrillation, ischaemic heart disease, chronic renal failure, and obstructive sleep apnoea.
He was referred into hospital by his General Practitioner (GP) with predominantly voiding LUTS such as slow flow and straining to void, as well as an ultrasound showing bilateral hydroureteronephrosis. He had no history of urinary tract infections or visible haematuria and was a nonsmoker. A bedside bladder scan revealed a post-void residual volume of 380mL, and he had an acute on chronic renal injury on blood tests. A urethral indwelling catheter (IDC) was placed and after being monitored for post-obstructive diuresis, he was discharged home.
He returned to hospital four weeks later for an elective transurethral resection of prostate (TURP). He had an uncomplicated procedure, but initially failed his trial of void and was discharged home with an IDC in situ. He later passed his trial of void and the histopathology from his TURP returned with benign prostatic hyperplasia (BPH).
He was admitted again several months later with worsening LUTS, particularly severe urinary incontinence affecting his quality of life, as well as declining renal function with bilateral hydroureteronephrosis again demonstrated on repeat imaging. His post-void residual varied between 100-150mLs. He had a urethral IDC inserted again but his kidney function did not improve as expected. A MAG3 (mercaptoacetyltriglycine) renogram was performed which showed possible upper tract obstruction, and he underwent cystoscopy and bilateral ureteric stent insertion. He was discharged home without a urethral IDC. His kidney function still did not improve and a repeat MAG3 scan showed no improvement in renal excretion despite the stents being in the appropriate position. The stents were therefore removed.
Over the next six months, the patient had several admissions into hospital where a urethral IDC was inserted and would then subsequently be removed. Interestingly, his kidney function appeared to improve with IDC placement. Therefore, he had a urethral IDC placed with a view to this remaining permanent until definitive treatment was decided on. In his work-up, he had a cystoscopy and computed tomography (CT) scan for an episode of visible haematuria that showed no evidence of malignancy. He then went on to have video urodynamics which demonstrated bilateral vesicoureteric reflux with a small capacity bladder of 20mL and was booked for intravesical botulinum toxin to try to improve his bladder capacity
He was admitted for his elective cystoscopy and intravesical botox injection about three years after his first presentation. On cystoscopy, he had a large prostate cavity from his previous TURP, a stenosed bladder neck and an extremely contracted bladder with only a tiny vertical column of bladder urothelium visible between two grossly dilated ureteric orifices. Fluoroscopy was used to outline his anatomy (see Image 1) with his ureters appearing to enter almost directly into his prostate cavity. The planned injection of intravesical botulinum toxin was abandoned and a urethral IDC was replaced.
The patient had a very poor quality of life with an IDC as it sat within the prostate cavity causing severe discomfort and bypassing often. Given the patient’s extremely contracted bladder and poor quality of life with the IDC, he was offered and underwent a sub-total cystectomy and formation of ileal conduit. The histopathology from his operation revealed an almost entirely denuded urothelium with prominent fibrosis and acute with chronic inflammation within the bladder wall.
He recovered well and is much happier with his quality of life with an ileal conduit.
Discussion
When our patient first presented to our service, he clearly had been suffering from LUTS for many years resulting in chronic urinary retention and reflux nephropathy. It is likely that at this point, he already had a degree of irreversible bladder fibrosis and decreased bladder compliance. The catheterisation over the following years, as well as chronic inflammation, likely resulted in his bladder contracting down and becoming almost obliterated [3,4].
There are several key learning points in this case. Ideally video urodynamics should have been performed earlier and before his bladder capacity was so small. This could potentially have allowed his poorly compliant bladder to be treated earlier, with treatments such as intravesical botulinum toxin or even an ileocystoplasty. Secondly, the bladder capacity for this patient could have been preserved. Several strategies have been recommended to maintain bladder capacity, including intermittent catheterisation, or using a catheter valve to allow the bladder to fill [3]. These alternative bladder management methods were certainly considered and the patient was referred to Continence for bladder training and education on self-intermittent catheterisation (SIMC), however, renal function continued to decline without permanent catheterisation as well as ongoing urinary incontinence. Placement of permanent IDC was complicated by haematuria due to lifelong anticoagulation for atrial fibrillation in this patient. Bilateral nephrostomy for urinary diversion posed a similar dilemma with issues surrounding anticoagulation, as well as being unacceptable to the patient from a quality-of-life perspective. In managing complex cases of severe LUTS such as this, collaboration with other specialists and multidisciplinary care may be of value and the patient was also referred to Nephrology for ongoing input regarding his renal function. Lastly, whilst cystectomy is a morbid operation with many risks, it should be considered in patients with severe symptoms and a poor quality of life secondary to their LUTS.
Conclusion
Patients suffering from LUTS need to be identified and appropriately managed early to prevent irreversible changes to bladder composition, compliance, and capacity. Once permanent changes have occurred, steps should be taken to preserve the remaining bladder function and maintain quality of life. Urinary diversion should be considered if a patient is suffering from severe symptoms, is medically fit, and has exhausted other management options.
Declarations of Interest
None
Funding
This research did not receive any specific grant from funding agencies in the public, commercial or not-- for-profit sectors.
- Panwar V, Tosh J, Mittal A, Narain T, Mandal A, Talwar H (2022) Small contracted bladders posing bigger problems: Etiology, presentation and management and a short review of the literature. J Family Med Prim Care; 11: 2246-51
- Fry C, Kitney D, Paniker J, Drake M, Kanai A, Andersson K (2018) Fibrosis and the bladder, implications for function ICS-RS 2017. Neurourol Urodynam; 37: S7-12
- Reid S, Brocksom J, Hamid R, Ali A, Thiruchelvam N, Sahai A, et al. (2021) British Association of Urological Surgeons (BAUS) and Nurses (BAUN) consensus document: management of the complications or long-term indwelling catheters. BJU Int. 128: 667-77.
- Cantu H, Maarof S, Hashim H (2019) The Inflammatory Contracted Bladder. Curr Bladder Dysfunt Rep. 14:67-74
FIGURE 1
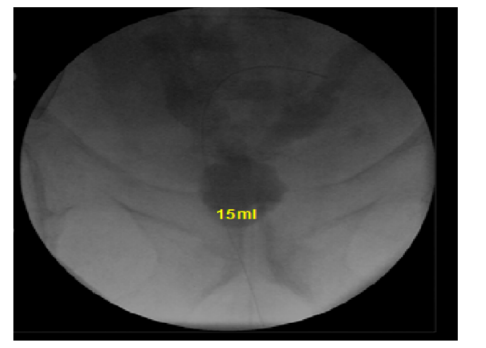
Figure 1: Video urodynamics showing small bladder capacity of 15-20mL and bilateral vesicoureteric reflux.
FIGURE 2
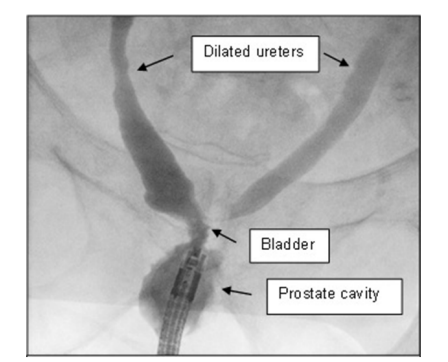
Figure 2: Fluoroscopy performed during cystoscopy highlighting patient's bladder anatomy
Figures at a glance