A Case of Nasopharyngeal Posterior Wall Injury due to an Unusual Metallic Foreign Body
Received Date: April 25, 2024 Accepted Date: May 25, 2024 Published Date: May 28, 2024
doi: 10.17303/jspcr.2024.6.201
Citation: Navid Ahmady Roozbahany, Semiramis Nasri, Amin Hasheminia (2024) A Case of Nasopharyngeal Posterior Wall Injury due to an Unusual Metallic Foreign Body. J Surg Proce Case Rep 6: 1-8
Abstract
We present a case of unusual nasopharynx injury caused by a metallic shaving entering the oral cavity, perforating the soft palate, and injuring the nasopharynx mucosa. The imaging revealed that the foreign body is embedded very close to the clivus of the occipital bone. After ruling out major vascular and neurological injury, the foreign body was successfully retrieved, and the post-operative course was favorable. The significance of self-protection devices and familiarity with the region's anatomy is discussed.
Keywords: Nasopharyngeal Posterior Wall Injury; Nasopharynx Injury; Oral Cavity; Nasopharynx Mucosa; Occipital Bone
Case Report
Following an accident on a construction site, paramedics transported a 30-year-old male patient to the emergency room. The patient, a metal worker, was making hole in a piece of metal with a motorized tool, resulting in production of some metallic shavings including a long swarf. This stringy tendril emerged from the work surface and moved toward the patient. Because the patient's mouth was open at the time, the metal piece got into his mouth. It penetrated the soft palate and became lodged in the posterior wall of the lower nasopharynx. The piece was more than 50 cm long and was cut by paramedics at the scene just outside the patient's mouth to help him move. There was only minor self-limiting bleeding from the mouth and both nasal nostrils.
The patient was agitated and terrified while in the emergency room. He was reassured, and IV lines were put in place. The patient was unable to speak but was alert and cooperative. There had been no previous medical or surgical history. The vital signs remained stable, and the general examination was unremarkable. The function of the cranial nerves was normal, and there were no neurological signs or symptoms. There was no tenderness when the cervical spine was touched. The general examination, which included the heart, lung, abdomen, and extremities, was normal. There had been no other trauma to the body. The CBC, coagulation tests, and basic metabolic panels were all within normal limits.
In the head and neck examination, the patient's mouth was open, and a spiral piece of metal protruded from it (Figures 1 and 2). There was dried blood around the mouth and nose, but no active bleeding was present. Blood clots were found in both nasal cavities during an anterior rhinoscopy, but there was no active bleeding. The metallic piece was found to penetrate the soft palate just posterior to the posterior nasal spine. There was evidence of previous bleeding but no active hemorrhage. The other end of the metal piece was not visible.
Following local anesthesia, nasal and nasopharyngeal endoscopy revealed a foreign body penetrating the midline nasopharyngeal mucosa and lodging in the inferior border of the nasopharynx. Touching the piece gently revealed that it was firmly attached to the surrounding tissue.
An anterior-posterior and lateral X-rays of the skull were taken. The images revealed that the foreign body had penetrated deep into the mucosa and fascia before stopping just above the bone above C1, passing through the anterior atlantooccipital membrane part of the anterior longitudinal ligament and almost touching the clivus(Figures 3 and 4). Due to the patient's discomfort, no additional imaging was performed, and the patient was transferred to the operating room.
It was obvious that pulling the piece out directly would cause additional trauma and had the potential to cause catastrophic neural and/or vascular injury due to its proximity to the skull base, C1, and regional blood vessels. Due to the position of the foreign body, it was also impossible to secure any airways through the mouth or nose. While the tracheostomy and cricothyroidotomy set was being prepared, the team decided to begin with IV sedation and spontaneous respiration but to be prepared to secure a surgical airway if necessary. Following the induction of IV sedation using ketamine, sodium thiopental, and midazolam, oxygen administered via nasal cannula, the mouth was kept open by manual traction and repeated oropharyngeal suction was performed. The inner end of the foreign body was visualized using a laryngoscopy 75-degree rigid endoscope. Instead of pulling, the surgeon began rotating the piece counterclockwise, dislodging it from the bone, facia, and mucosa in the same way that a screw was removed. The piece was dislodged after one full turn, and it was out of the nasopharyngeal mucosa after two turns. It was then pulled through the soft palate laceration and delivered out of the mouth. There was minor bleeding at the entry point in the nasopharynx, which was controlled with gentle pressure for 2 minutes. Afterward, the patient underwent general anesthesia, and oral intubation was performed. The nasopharyngeal injury site was washed with normal saline and repaired with one layer of Vicryl sutures. The soft plate injury was repaired in three layers. The postoperative course was uneventful, and the patient was discharged the next day. The injuries were well healed at the two-week follow-up, and the patient had no symptoms.
Discussion
Metallic foreign bodies are common and usually secondary to embedded bullets or shrapnel from explosive weapons [1]. On the other hand, work-related foreign bodies are uncommon, and when they occur, they most commonly involve the eyes, facial skin, and subcutaneous tissues [2]. There have been reports of metallic foreign bodies involving arteries and veins, as well as structures as deep as the optic nerve; oropharyngeal and nasopharyngeal submucosal foreign bodies, on the other hand, are extremely rare [3]. After ingestion, sharp foreign bodies can become lodged in the mucosa and submucosa of the oropharynx, hypopharynx, or esophagus. There have been reports of needles or denture parts becoming lodged in these areas [4]; however, occupational injuries to the mucosa and submucosal structures of the nasopharynx are unique and have not been reported previously
A chain of events resulted in the unusual presentation of our case. He was working with high-speed and high- -power instruments without proper protection, which was most likely the most critical factor in his injury. The subsequent injury was also influenced by the head's position and the mouth's opening. If the mouth had been closed, the damage could have been limited to the lips and teeth. The angle at which the metallic piece traveled was also important, as it avoided the hard plate and instead injured the soft plate. Sharp object injury to the palate is not uncommon, and it usually occurs in children who fall while holding a pencil in their mouth [5]. By the way, perforating injury caused by a foreign object is extremely rare.
Nasopharynx is the pharynx's most superior portion. It is bounded superiorly by the skull base and inferiorly by the soft palate. The nasopharynx connects the nasal cavity to the oropharynx and houses the adenoids and Eustachian tube openings. Posterior pharyngeal wall bounds the posterior, and the medial pterygoid plates and superior pharyngeal constrictor muscles are lateral walls of nasopharynx. The nasopharynx has an anterior-posterior diameter of about 2 cm and a height of about 4 cm [6]. Nasopharynx contents include the opening of the eustachian tube, which is located on the posterolateral wall. The torus tubarius is located immediately posterior to the opening of the eustachian tube, the fossa of Rosenmuller is superior and posterior to the torus tubarius, and the adenoids (nasopharyngeal tonsils) are located in the nasopharynx's roof and posterior wall [6].
Branches of the internal carotid artery (mandibular artery), maxillary artery (pterygopalatine artery), facial artery (ascending palatine artery), and ascending pharyngeal artery (superior pharyngeal artery) supply the nasopharynx. The parapharyngeal venous plexus drains venous blood. It drains into the retropharyngeal and facial veins, connecting to the internal jugular vein [7]. The initial lymph-collecting system consists of a capillary network within the mucosal membrane linked to a similar network within the nasal atrium, turbinates, and posterior floor. The Rouvière nodes are the first encountered lymph nodes retropharyngeal lymph nodes. The internal jugular nodes are connected to the retropharyngeal nodes [8]. The maxillary division of the trigeminal nerve travels through the sphenopalatine ganglion and provides sensory innervation anterior to the eustachian tube opening. The glossopharyngeal nerve innervates the posterior sensory system. Except for the tensor veli palatini muscle, which is supplied by the mandibular division of the trigeminal nerve, muscles originating in the nasopharynx receive motor supply from the Vagus nerve [9].
The clivus is a bony structure at the base of the skull. It is a shallow depression behind the sphenoid bone's dorsum sellae. It gradually slopes to the anterior part of the basilar occipital bone, where it meets the sphenoid bone. The pons rests on the clivus' basilar surface. The abducens nerve follows the clivus during its track [10]. The ligaments that connect the occipital bone to the C1 and C2 vertebral bodies allow the craniovertebral junction to be extremely stable and flexible. The craniovertebral junction is made up of the occipital bone and condyles, as well as C1 and C2. The cruciate ligament, the paired alar ligaments, the tectorial membrane, the apical ligament, and the anterior and posterior atlanto-occipital membranes are all important ligaments that help hold these osseous structures together. The osseous elements' unique structure and horizontal orientation of their articulations allow for significant movement, with the majority of cervical spine flexion and extension occurring at occipital condyl-C1, and the majority of cervical spine axial rotation occurring at C1-C2. As a result, the craniovertebral junction ligaments are crucial to the stability of these unusually shaped joints [11]. The foreign body in our patient was precisely inside this junction.
Plain x-ray imaging of the craniovertebral junction is a quick and easy way to assess alignment. Because dynamic views are easily obtained, stability and ligamentous structure integrity can be determined. Plain radiographs, however, do not show the ligaments because of poor soft tissue contrast resolution and a lack of cross-sectional information [11].
The utilization of advanced imaging modalities, such as a CT scan, plays a crucial role in evaluating the intricate anatomy of the nasopharyngeal region when managing injuries involving metallic foreign bodies. CT scans can provide detailed images that are invaluable for understanding the relationship of the foreign body to critical bony structures, including the clivus, sphenoid, and vertebrae. These structures are significant not only due to their anatomical importance but also because of their proximity to the brain stem, spinal cord, and essential vascular anatomy, which necessitates a careful and thorough examination.
Specifically, the ability to visualize the precise location of the foreign body in relation to key arteries, such as the ascending pharyngeal artery, the ascending palatine branch of the facial artery, the ascending cervical artery, and the maxillary artery, although sometimes challenging to detect in CT scans, is particularly valuable. Accurate identification of these structures in various sections can greatly aid in the management and surgical planning for patients with similar injuries. Despite these advantages, the emergent situation and the patient's severe discomfort, compounded by the necessity to keep his mouth open continuously, along with the considerable emotional stress experienced by the patient and his family, influenced our decision to rely on plain X-rays rather than proceeding with a CT scan. This decision balanced the need for detailed anatomical information with the imperative to minimize further stress and discomfort for the patient [12].
MRI, while offering superior imaging for soft tissue evaluation, is contraindicated in the presence of metallic foreign bodies due to the risk of movement or heating of the metal, which could exacerbate the injury [13].
In this particular case, the plain X-rays provided adequate visualization to confirm that the bone had not been penetrated and to guide the subsequent surgical intervention. However, in less urgent situations or where additional anatomical detail is necessary to plan a more complex surgical approach, the use of CT scans should be strongly considered to ensure comprehensive assessment and optimal patient outcomes [14]. Future cases may benefit from a more flexible approach, where the use of advanced imaging can be tailored to the specific clinical scenario and the patient's overall condition.
Neurovascular injury in a complex anatomical site like the skull base is always a concern. In our case, the injury occurred in the midline, away from the internal carotids and vertebral arteries. We also believed that the injury was not caused by a high-velocity projectile, so trauma to distant anatomical elements was unlikely. Therefore, we decided not to perform an angiographical examination of the regional vessels before proceeding with surgery. The favorable post-operative course of our patient demonstrated that our approach was correct.
Similar cases in the literature highlight the rarity and complexity of such injuries. For instance, a case of a sewing needle lodged in the nasopharynx after accidental ingestion was reported, requiring careful endoscopic removal [15]. Another case involved a toothbrush penetrating the soft palate and extending into the nasopharynx, which was successfully removed surgically [16]. These cases, along with ours, underscore the need for meticulous planning and consideration of imaging to map the foreign body's trajectory and relations to critical anatomical structures.
This case underscores the critical importance of preventive measures and protective equipment in high-risk occupational settings. Personal protective equipment (PPE), such as face shields, safety goggles, and mouth guards, plays an essential role in preventing injuries caused by flying debris or accidental ingestion of foreign objects. Face shields, in particular, provide comprehensive protection by covering the entire face, including the eyes, nose, and mouth, thereby significantly reducing the risk of similar injuries. Additionally, adherence to safety protocols, such as keeping the mouth closed when working with high-speed tools, can further minimize the risk of injury. Proper training on the use of PPE and regular safety drills can enhance workers' awareness and adherence to safety measures. The efficacy of these protective measures is well-documented, as they have been shown to reduce the incidence of work-related injuries across various industries. Implementing stringent safety standards and ensuring the availability and use of appropriate protective equipment are vital steps in safeguarding workers, particularly in environments involving high-speed machinery and hazardous materials [17].
Conclusion
This case highlights the critical importance of meticulous evaluation for patients with penetrating foreign bodies, utilizing appropriate imaging modalities, and timely surgical management. Effective collaboration between surgeons and anesthesiologists is essential in managing aerodigestive tract injuries. Additionally, the article emphasizes the necessity of personal protective equipment and strict adherence to safety guidelines, especially when operating high- -speed and powerful tools.
- Negoduyko V, Mikhaylusov R, Velikodnyi A, Kovtun K (2019) Research of Foreign Bodies Soft Tissue Gunshot Origin. Georgian Medical News, 297: 13-7.
- Zhao Y, Li Y, Li Z, Deng Y (2020) Removal of Orbital Metallic Foreign Bodies With Image-Guided Surgical Navigation. Ophthalmic Plastic and Reconstructive Surgery, 36: 305-10.
- Zhang C, Wu J, Zhang W, Yuan H, Yang C, et al. (2022) Preliminary Study of the Treatment Strategy for Retaining Traumatic Foreign Bodies Involving the Carotid Artery. The Journal of Craniofacial Surgery.
- Bendiouri R, Chennoufi I, Lachkar A, Benfadil D, Abdenbi A, et al. (2021). Internal Jugular Vein Thrombosis by Sewing Needle Ingestion. International Journal of Surgery Case Reports, 83: 105988.
- Qing-Bin Z, Zhao-Qiang Z, Dan C, Yan Z (2013) Epidemiology of Maxillofacial Injury in Children Under 15 Years of Age in Southern China. Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology, 115: 436-41.
- Mukherji SK, Castillo M (1998) Normal Cross-sectional Anatomy of the Nasopharynx, Oropharynx, and Oral Cavity. Neuroimaging Clinics of North America, 8: 211-8.
- Tobias PV (1981) The Nasopharynx: Review of Structure and Development, with Notes on Speech, Pharyngeal Hypophysis, Chordoma and the Dens. The Journal of the Dental Association of South Africa, 36: 765-78.
- Davis KR (1987) Embolization of Epistaxis and Juvenile Nasopharyngeal Angiofibromas. AJR. American Journal of Roentgenology, 148: 209-18.
- Chong VF, Ong CK (2008) Nasopharyngeal Carcinoma. European Journal of Radiology, 66: 437-47.
- Rai R, Iwanaga J, Shokouhi G, Loukas M, Mortazavi MM, et al. (2018) A Comprehensive Review of the Clivus: Anatomy, Embryology, Variants, Pathology, and Surgical Approaches. Child's Nervous System, 34: 1451-8.
- Nidecker AE, Shen PY (2016) Magnetic Resonance Imaging of the Craniovertebral Junction Ligaments: Normal Anatomy and Traumatic Injury. Journal of Neurological Surgery. Part B, Skull Base, 77: 388-95.
- Towbin AJ, D'Souza BM (2013) Patient Comfort During Imaging Procedures. Radiology Clinics of North America, 51: 681-93.
- Kanal E, Shellock FG (2014) Magnetic Resonance Imaging of Patients with Implants and Devices: An Update. Journal of Magnetic Resonance Imaging, 40: 557-75.
- Koivikko MP, Salminen JT (2007) The Role of Computed Tomography in the Evaluation of Penetrating Injuries. European Journal of Radiology, 61: 59-66.
- Lohn JW, Penn-Barwell JG (2011) Management of Penetrating Foreign Bodies in Head and Neck Trauma. Clinical Otolaryngology, 36: 214-22.
- Rothrock SG, Green SM (2006) Foreign Bodies in the Upper Airway and Gastrointestinal Tract. Pediatric Emergency Care, 22: 527-34.
- Weisenbach CA, McGhee JS (2021) Aviation Maxillofacial Shields and Blunt Impact Protection in U.S. Army Helicopter Mishaps. Aerospace Medicine and Human Performance, 92: 50-3.
FIGURE 1

Figure 1: The lateral view of the patient
FIGURE 2
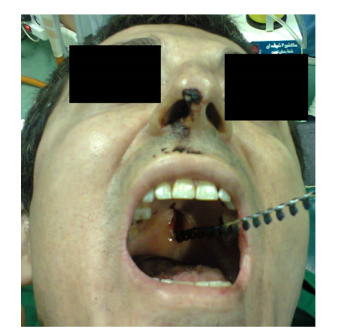
Figure 2: Intraoral view
FIGURE 3
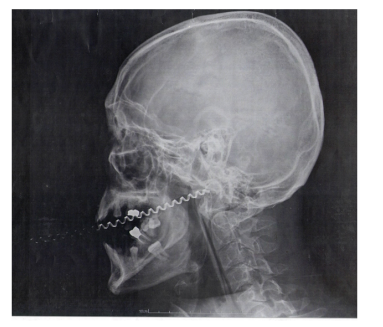
Figure 3: Lateral Skull X-ray
FIGURE 4
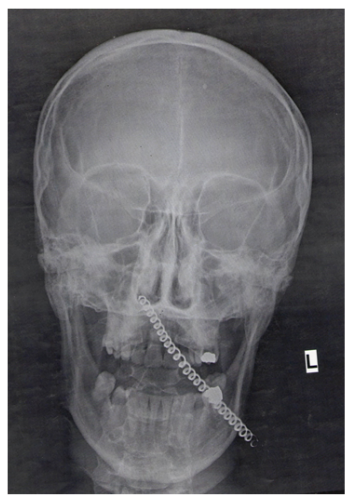
Figure 4: AP Skull X-ray
Figures at a glance