Correction of Anatomical Aberration: Posterior Repositioning of Right Hepatic Artery in Choledochal Cyst Excision and Hepaticojejunostomy - Case Report
Received Date: May 24, 2024 Accepted Date: June 24, 2024 Published Date: June 27, 2024
doi: 10.17303/jspcr.2024.6.203
Citation: Ravindra Budhwani M.Ch, Arun ManoharanM.S, Vijay Kumar Sharma M.Ch, Abhijit Chandra M.Ch (2024) Correction of Anatomical Aberration: Posterior Repositioning of Right Hepatic Artery in Choledochal Cyst Excision and Hepaticojejunostomy- Case Report. J Surg Proce Case Rep 6: 1-9
Abstract
The right hepatic artery crossing the common hepatic duct anteriorly is one of the frequent abnormalities. This aberrant right hepatic artery interferes with the dissection of the common bile duct and can cause postoperative hepaticojejunostomy stenosis. So repositioning of the right hepatic artery posterior to hepaticojejunostomy should be done. We had a 28-year-old female who presented with upper abdominal pain and on evaluation was diagnosed with a choledochal cyst and pancreaticobiliary maljunction. Abdominal MRI showed an aberrant right hepatic artery running anteriorly to the common hepatic duct. Open choledochal cyst resection and hepaticojejunostomy were planned. Intraoperative findings showed the aberrant right hepatic artery crossing the choledochal cyst anteriorly. We performed open hepaticojejunostomy by replacing the aberrant right hepatic artery posteriorly to facilitate suturing and prevent postoperative anastomotic stenosis. The postoperative course was uneventful, with no findings suggestive of anastomotic leak, stenosis, strictures, bleed, liver dysfunction, or abscess. The abnormality of the right hepatic artery is reported to be one of the primary causes of anastomotic stenosis after hepaticojejunostomy. Once anastomotic stenosis or stricture develops, it is often difficult to treat. In a choledochal cyst with an aberrant right hepatic artery, posterior repositioning is effective for preventing postoperative anastomotic stenosis and cholestasis.
Keywords: Anomalous Right Hepatic Artery; Choledochal Cyst; Posterior Repositioning
Introduction
High incidence of vascular anomalies in HPB surgery should be viewed as the norm rather than an anomaly as they can alter the surgical strategies. 31% of the population from the southern part of India had variant arterial anatomy [1].
The right hepatic artery running on the anterior side of the common hepatic duct (CHD) is one of the prevalent abnormalities [2]. In the situation of the choledochal cyst (CDC), anomalous right hepatic artery (ARHA) interferes with the CDC circumferential dissection, proximal transection of CDC, hepaticojejunostomy (HJ) suturing and can cause postoperative anastomotic stenosis [3]. Furthermore, ARHA obstructs CDC dissection; additionally, can go into spasm and it can come into bites during hepaticojejunostomy (HJ) suturing, causing bleeding or a potential pseudoaneurysm. To avoid stenosis of HJ, we outline our surgical strategy for replacing the ARHA posteriorly in hepaticojejunostomy. Also when undergoing surgery for HJ stricture, there is a significant risk of ARHA injury if it is not positioned posteriorly, which can also lead to a higher risk of re-stricture and HJ leaks.
Case Presentation
A 28-year-old female patient presented with continuous, dull, non-radiating abdominal pain in the right upper quadrant for two months. There was no additional noteworthy medical or surgical background. On physical examination, she showed no signs of jaundice and was in fair overall general condition. Abdominal examination were normal. There were no palpable lymph nodes, inguinal masses, or visible collaterals. Liver function tests, serum electrolytes, renal function tests, and complete blood counts were normal, and HIV testing and hepatitis viral markers were negative. A type I C choledochal cyst with an abnormal right hepatic artery coursing anteriorly to CDC was seen on MRI (Figure1,2,3) and was scheduled an open choledochal cyst excision and Roux en-Y hepaticojejunostomy after a diagnosis of choledochal cyst type IC in the Todani classification [4].
Under general anaesthesia, supine position, the abdomen is entered through a Kocher incision. The intraoperative findings showed that ARHA crossed anteriorly of CDC (Figure 4) just below the confluence. After the dissection of the CDC using an energy device instrument and looping the CDC, distal transection was done just above the joining of the CC and pancreatic duct (Figure 5). After dissecting ARHA from CDC, looping of ARHA was done. CDC was taken anteriorly to RHA and posterior repositioning of the ARHA was performed (Figure 6) because it seemed to compress the CHD and risked postoperative HJ stenosis. Proximal transection was done just below the confluence and intraoperative choledochoscopy was done to rule out web, membrane, stenosis, stones, and sludge (Figure 7). While performing HJ repositioning the ARHA posteriorly helped in suturing and bites were taken cautiously avoiding RHA which if taken may cause haemorrhage and pseudoaneurysm (Figure 8). After finishing the HJ, the pulsation of the ARHA was felt, confirming the blood flow. We placed a drain posteriorly to the HJ, later jejunojejunostomy was done. In the postoperative period patient tolerated orally on postoperative day (POD) 2, and on POD 5, the drain was removed as it had a serous nature, negative amylase, and declining volume. The LFT on POD 3 and POD 5 was within the normal range. For five days, we gave antibiotics intravenously. After the wound sutures were removed on POD 7, the patient was discharged. During our follow-up of 3 months, there were no clinical symptoms, no derangement in LFT and intrahepatic bile ducts were normal in diameter on abdominal ultrasonography.
Discussion
Surgeon and interventional radiologists should be aware of anatomical variations of the hepatic artery throughout its course as it is of utmost importance in surgery including liver transplantation, pancreatoduodenectomy, biliary reconstruction or planning for percutaneous interventional angioplasty. Few available strategies for managing aberrant arteries include sacrifice, embolization, dissection and preservation, or transaction and reconstruction. If small artery, sacrifice can be done but a large caliber artery preservation is necessary for adequate surgical outcome. Preoperative embolization are also performed for the maintenance of collateral circulations. Resection and reconstruction or reimplantation can be done in pancreatic tumor involvement of ARHA. Ultimately Dissection and preservation is most optimal approach for aberrant arterial variation. But if gets sacrificed, extrahepatic circulation of the liver acts as collateral circulation which comes from epigastric arteries, inferior phrenic arteries and small gastric arteries.
The right hepatic artery running anteriorly to the choledochal cyst is one of the numerous anomalies of the HPB region [1]. Todani reported on the method of restoring normal anatomy by positioning the ARHA posterior to CHD [4]. Lal et al. stated that the ARHA courses the anterior wall of the CDC in 12.8% of children [5]. A typical anatomical anastomosis was restored by posteriorly realigning these arteries.
Cases of dorsal ARHA replacement during laparoscopic redo-HJ were documented by Diao et al. [2]. Additionally, they noted that in 23.3% of patients with surgical recurrent biliary obstruction, the ARHA ran anteriorly to the CHD. After HJ, one of the main causes of anastomotic stenosis was the anomalous RHA [6].
HJ stenosis might result in stricture, cholangitis, or intrahepatic stones. Liver fibrosis and cirrhosis would eventually result from these problems' long-term repercussions. Managing a hepaticojejunostomy stricture can be a challenging task. Anastomotic stricture can be managed with additional techniques like balloon dilatation of the anastomosis, and percutaneous transhepatic biliary drainage [7]. However, these techniques can result in tube placement for a longer time, which can cause cholangitis, cholestasis, and stenosis of the bile duct at the drain placement site. Double-balloon enterotomy (DBE), a less invasive method used for anastomotic stenosis, was described by Ono et al. [8] as a means of managing postoperative intrahepatic stones. However, these modalities of treatment have only shown to be palliative in nature when treating anastomotic stenosis brought on by extrinsic causes, such as ARHA. Making an early determination on whether the ARHA needs to be repositioned is crucial for hepaticojejunostomy and open choledochal cyst resection. Based on intraoperative results, such as the presence of ARHA, the decision should be made.
Conclusion
We encountered a case of a choledochal cyst with ARHA in which the artery was replaced posteriorly at the anastomosis after open choledochal cyst excision and hepaticojejunostomy. In surgery for a choledochal cyst with ARHA, replacing the artery to the posterior side of the anastomosis is essential for preventing postoperative extrinsic anastomotic stenosis.
Conflict of Interest
The authors declare that they had no conflict of interest. There was no source of funding for this study.
Acknowledgement
None
- Rajapriyan P, Dutta S, Nagarajan K, Ariharan K, Ramakrishnaiah VP (2022) Prevalence of hepatic vascular anomalies in consecutive contrast-enhanced computed tomography images — A retrospective observational study. Egyptian Liver Journal, 12: 1-11.
- Tsuchiya R, Eto T, Harada N, Yamamoto K, Matsumoto T, Tsunoda T et al. (1984) Compression of the common hepatic duct by the right hepatic artery in intrahepatic gallstones. World J Surg. 8: 321-6.
- Diao M, Li L, Cheng W (2015) Recurrence of biliary tract obstructions after primary laparoscopic hepaticojejunostomy in children with choledochal cysts. Surg Endosc. 30: 3910-5.
- Todani T, Watanabe Y, Toki A, Ogura K, Wang ZQ (1998) Co-existing biliary anomalies and anatomical variants in the choledochal cyst. Br J Surg. 85: 760-3.
- Lal R, Behari A, Hari RH, Sikora SS, Yachha SK, Kapoor VK (2013) Variations in biliary ductal and hepatic vascular anatomy and their relevance to the surgical management of choledochal cysts. Pediatr Surg Int. 29: 777-86.
- Urushihara N, Fukumoto K, Fukuzawa H, Mitsunaga M, Watanabe K, Aoba T et al. (2012) Long-term outcomes after excision of choledochal cysts in a single institution: operative procedures and late complications. J Pediatr Surg. 47: 2169-74.
- Urushihara N, Fukumoto K, Fukuzawa H, Mitsunaga M, Watanabe K, Aoba T et al. (2012) Long-term outcomes after excision of choledochal cysts in a single institution: operative procedures and late complications. J Pediatr Surg. 47: 2169-74.
- Ono S, Maeda K, Baba K, Usui Y, Tsuji Y, Yano T et al. (2013) The efficacy of double-balloon enteroscopy for intrahepatic bile duct stones after Roux-en-Y hepaticojejunostomy for choledochal cysts. Pediatr Surg Int. 29: 1103-7.
FIGURE 1

Figure 1: MRCP Showing Type 1 Choledochal Cyst
FIGURE 2
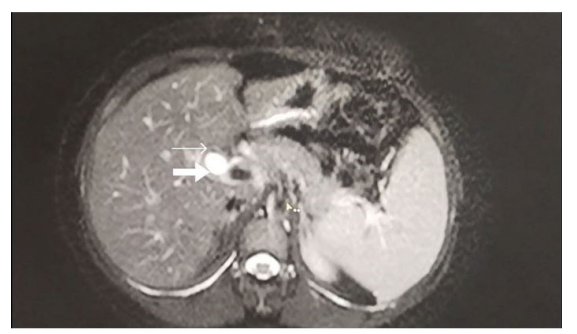
Figure 2: Axial Section of Contrast Enhanced MRI Showing Choledochal Cyst (Thick Arrow) And Right Hepatic Artery Traversing Anteriorly (Thin Arrow) To Choledochal Cyst
FIGURE 3
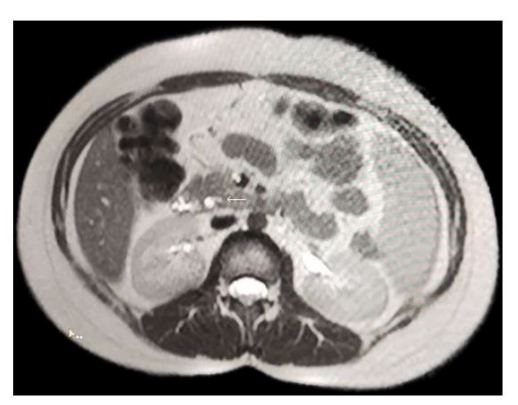
Figure 3: Axial Section Of MRCP Showing Joining Of Pancreatic Duct With Choledochal Cyst
FIGURE 4
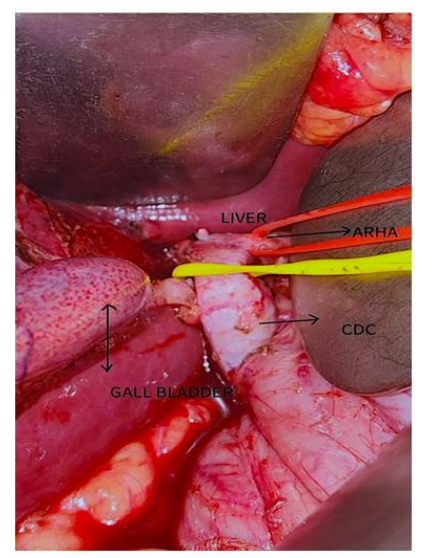
Figure 4: Anomalous Right Hepatic Artery Crossing Anterior To Choledochal Cyst
FIGURE 5
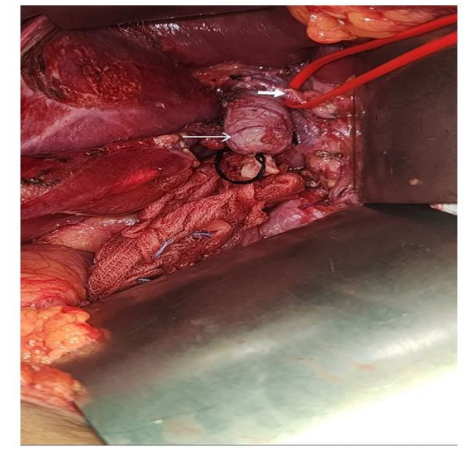
Figure 5: Distal Transection Of Choledochal Cyst
FIGURE 6
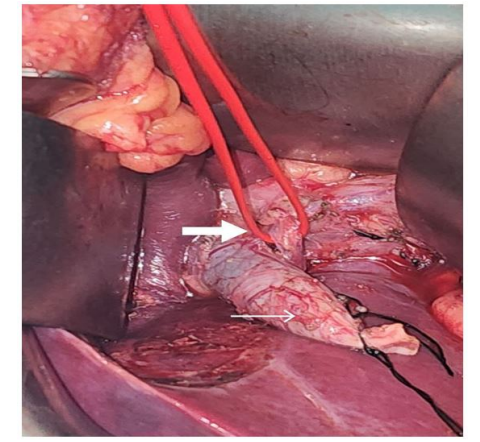
Figure 6: Repositioning Of Anomalous Right Hepatic Artery Posterior to Choledochal Cyst
FIGURE 7
Figure 7: Intraoperative Choledochoscopy
FIGURE 8
Figure 8: Hepaticojejunostomy Lying Anterior To Right Hepatic Artery
Figures at a glance