Gallbladder Volvulus: A Rare Presentation
Received Date: August 07, 2024 Accepted Date: September 07, 2024 Published Date: September 10, 2024
doi: 10.17303/jspcr.2024.6.204
Citation: Greg W Zhang, Jack A Will, Sarah A Person, W Gregory Reese, Mark O Tucker, et al. (2024) Gallbladder Volvulus: A Rare Presentation. J Surg Proce Case Rep 6: 1-9
Abstract
Gallbladder volvulus is an exceedingly rare presentation that tends to resemble acute cholecystitis, presenting in about 1 in 365,000 cases of gallstone disease. In this article, we report a case of an 89-year-old female who presented to our emergency department with three days of progressive nausea, vomiting, poor oral tolerance, and abdominal pain. Initial imaging revealed diffuse gallbladder wall thickening and edema characteristic of acalculous cholecystitis. The patient was admitted to the surgery service, but due to her age and other medical comorbidities, the patient was referred to interventional radiology for placement of a cholecystostomy tube. It was determined by the radiologist that the patient had a gallbladder volvulus for which a cholecystostomy tube would be contraindicated. As a result, after undergoing preoperative risk stratification and initiation of IV antibiotics, the patient underwent a successful laparoscopic cholecystectomy and did well postoperatively. Intraoperative findings included a necrotic appearing gallbladder that was twisted on the cystic artery. This represents a rare, challenging condition for which the mainstay is urgent same-day admission and cholecystectomy.
Keywords: Gallbladder Volvulus; Cystic Duct; Artery; Biliary Drainage; Acute Cholecystitis
Introduction
The first case of gallbladder volvulus was documented by Wendel in 1898, describing a “floating” gallbladder with a long mesentery and cystic duct [1]. Since then, there have been over 500 cases published in the literature [2]. Gallbladder volvulus occurs more frequently in elderly females and is characterized by a gallbladder with abnormal torsion along its long axis (the axis of the cystic duct and artery). This results in ischemia due to interruption of blood flow from the cystic artery, and distension due to interruption of biliary drainage through the cystic duct [1,3]. It represents a difficult diagnosis due to its rarity, subtle and easily missed radiological features, and overlap of symptoms with other more common pathological conditions affecting the biliary tract such as acute cholecystitis. Often, nonspecific symptoms and equivocal findings on imaging lead towards more common diagnoses, and gallbladder volvulus is not identified until the intraoperative setting. A high degree of suspicion should warrant surgical exploration and should not be treated with nonoperative measures such as antibiotics, percutaneous drainage, or observation due to the high risk of gallbladder ischemia and subsequent perforation [4]. In this paper, we discuss a case of early identification of gallbladder volvulus, resulting in a successful, uncomplicated laparoscopic cholecystectomy with an excellent postoperative outcome.
Case
An 89-year-old female with a past medical history of hypertension, hyperlipidemia, coronary artery disease, myocardial infarction, congestive heart failure with reduced ejection fraction (30-35%), osteoarthritis, colon cancer, and chronic back pain secondary to scoliosis presented to the emergency department at our urban, tertiary care hospital after three days of worsening nausea, vomiting, right upper quadrant abdominal pain radiating to the back, and inability to tolerate both solids and liquids. She had no prior history of biliary colic symptoms. She had an extensive surgical history with multiple open abdominal surgeries including a hysterectomy for unknown indications; a sigmoid colectomy for early-stage colon cancer complicated by an incisional hernia requiring two subsequent open ventral hernia repairs; and an additional celiotomy with extensive lysis of adhesions and small bowel resection for a bowel obstruction. Her home medications included aspirin, atorvastatin, carvedilol, lisinopril, nitroglycerin, and polyethylene glycol (stool softener). She denied the use of alcohol, tobacco, or illicit drugs. Family history included heart disease in her father.
Clinical evaluation showed an afebrile, and well-appearing elderly female with moderate abdominal tenderness upon palpation of the right upper quadrant and epigastrium with no rebound or guarding. She had a BMI of 19 and denied any recent weight loss or gain. All vital signs were within normal limits. Laboratory investigations were remarkable for a glucose of 136 and albumin of 3.1, with all other lab values within normal limits including her transaminases and total bilirubin. Both sonographic and physical Murphy’s signs were absent. She underwent workup for biliary pathology given her classical presentation for suspected symptomatic cholelithiasis or acute cholecystitis. However, a right upper quadrant US identified diffuse gallbladder wall thickening and edema with no calculi. Because the quality of the US was limited by bowel gas and the patient’s complicated medical and surgical history, a computed tomography (CT) scan was obtained in the ED in addition. Furthermore, her extensive past surgical history allowed for a broad list of differential diagnoses which CT imaging could help narrow. The CT showed severe, diffuse gallbladder wall thickening, edema, and pericholecystic fluid highly suggestive of acute cholecystitis.
Due to the combination of the patient’s age, medical comorbidities, most notably the significant cardiac history, and a high level of suspicion for a hostile abdomen, our acute care surgical service evaluated the patient and subsequently recommended that the patient’s presumed diagnosis of acute acalculous cholecystitis be managed with the placement of a cystostomy tube by interventional radiology. Considering the hostile abdomen expected and that this patient was ostensibly suffering an acalculous cholecystitis, we planned for the cholecystostomy tube to potentially be definitive treatment with the goal of outpatient removal without cholecystectomy if appropriate. However, upon further review of the imaging by the radiologist, it was determined that there was a 360-degree volvulus of the gallbladder resulting in the obstructed gallbladder fundus being separated from the gallbladder fossa and a “swirl sign” characterized by a rapid tapering of the gallbladder neck.
After discussion with the patient, we recommended an urgent cholecystectomy after undergoing medical optimization and risk stratification. The surgical risk was deemed elevated but acceptable, so the patient was scheduled for a robot-assisted laparoscopic cholecystectomy the same day.
The procedure began by attempting Hasson entry at Palmer’s point. The dissection proceeded past the fascia and muscle, but a layer of subfascial mesh from her previous incisional hernia repair precluded the peritoneal entry. The same technique was employed in the right lower quadrant of the abdomen which was successful. Extensive laparoscopic adhesiolysis took an estimated one hour of operative time with a combination of blunt dissection, electrocautery with the harmonic scalpel, and sharp dissection with endoshears. Additional trocars were placed in the right upper quadrant, mid-epigastric region, and just lateral to the midclavicular line in the typical laparoscopic cholecystectomy approach. Upon visualization of the gallbladder, it appeared to be torsed by 180-degrees. Through retraction of the volvulized segment upward and the infundibulum laterally, we were able to successfully devolvulize the gallbladder. The hepatocystic triangle was easily dissected as there was minimal inflammation and healthy appearing tissue just inferior to the volvulus. The peritoneum was then mobilized, and the cystic duct and artery were identified using Firefly Fluorescence Imaging. The gallbladder was dissected in a "bottom-up" approach ensuring excellent hemostasis to the gallbladder fossa. The critical view of safety was established, and the cystic artery and duct individually clipped and divided. Once the gallbladder was mobilized from the liver, it removed from the abdomen using an Endo-Catch bag. The skin was closed, and the patient was extubated and returned to the surgical unit in stable condition.
The patient’s diet was advanced, and she was discharged on postoperative day two with two additional days of amoxicillin-clavulanate for intraabdominal infection prophylaxis as well as tramadol and acetaminophen on an as-needed basis for pain control. Three weeks later she was seen in clinic for postoperative follow-up where she endorsed minimal post-cholecystectomy symptoms as well as continued resolution of her pain. She presented to the emergency department and was admitted briefly for a small bowel obstruction 6 months after the procedure which resolved nonoperatively with bowel rest and a successful gastrografin challenge.
Discussion
Gallbladder volvulus is associated with an anatomical abnormality of the vascular pedicle to the gallbladder or the presence of an abnormally long mesentery from the gallbladder to liver bed [6]. This ultimately results in a “floating” gallbladder with abnormal mobility that can twist around the axis of the cystic duct and artery [7]. The majority of patients, approximately 84%, are over the age of 70 [1,8]. Contributing factors to this condition include loss of visceral fat, peristaltic activity of the surrounding bowel, spinal deformities, and having a tortuous, atherosclerotic cystic artery [3,9]. Scoliosis may allow for an aberrant vertical positioning of the gallbladder [9]. The two anatomic variants described in the literature are type A, with an elongated mesentery that supports both the gallbladder and cystic duct, and type B, with a defective mesentery that only connects cystic duct with liver [10]. Our patient, not surprisingly, had all of these contributing factors including having a minimal visceral fat and a thin atrophic cystic artery, with a known history of scoliosis.
Gallbladder volvulus is associated with the typical presentation of acute cholecystitis including nausea, vomiting, and decreased oral tolerance [1,7]. Many patients present with a palpable gallbladder on physical examination due to longstanding gallbladder distension [1,11]. The disease likely presents in the elderly due to a lack of visceral fat, ultimately resulting in a thin, skeletonized gallbladder pedicle [12,13]. Jaundice is an uncommon finding due to over >70% of gallbladder volvulus being acalculous and not associated with biliary obstruction in the common bile duct [14].
On ultrasound, criteria for the diagnosis of a gallbladder volvulus include a thickened and hypoechoic gallbladder wall that displays gangrene and inflammation, a “floating” gallbladder in which the majority of the organ does not adhere to the liver bed, and a conical structure at the gallbladder neck consisting of multiple linear echoes converging toward the tip [3,15]. Hepatobiliary iminodiacetic acid (HIDA) scan may reveal a bullseye image due to the subsequent accumulation of the radio isotope in the gallbladder [1]. CT imaging may demonstrate a gallbladder abnormally positioned outside its anatomical fossa, a vertical to horizontal rotation of the gallbladder's axis, or a twisting along the gallbladder's vascular pedicle [1,16]. In high-risk patients, magnetic resonance cholangiopancreatography (MCRP) may be useful in identifying characteristic features of gallbladder volvulus. These include a V-shaped distortion of the extrahepatic bile ducts caused by cystic duct traction, tapering, and twisting interruption of the cystic duct, an enlarged gallbladder deviated toward the midline, or a gallbladder, extrahepatic bile ducts, and cystic duct showing variable intensities [1].
Nonoperative measures, such as conservative management with antibiotics or percutaneous drainage, should ultimately be ruled out once gallbladder volvulus has been confirmed due to the high risk of associated gallbladder necrosis and perforation [17]. Current literature suggests that while these approaches may be appropriate for acute cholecystitis, the mechanical obstruction and vascular compromise inherent to gallbladder volvulus necessitates surgical management [3]. Delayed treatment with these nonoperative measures has been associated with significantly increased morbidity and mortality as the sequelae of this disease process is ultimately perforation of the gallbladder resulting in intra-abdominal infection.
This case particularly highlights the importance of diagnostic vigilance, particularly in the case of elderly patients with a low BMI and atypical presentations of acute cholecystitis. While rare, gallbladder volvulus should be considered in the differential diagnosis for elderly patients presenting with symptoms of acute cholecystitis in the absence of jaundice or biliary obstruction [17]. Early recognition is critical, as delayed diagnosis can lead to severe complications and poor patient outcomes. This case reinforces the importance of maintaining a high index of suspicion for this condition, particularly when imaging suggests abnormal positioning outside of the gallbladder’s anatomical fossa.
Conclusions
Gallbladder volvulus is an extremely rare diagnosis. The general or acute care surgeon needs to differentiate this challenging case from typical acute cholecystitis. The diagnosis relies on accurate history, physical examination,and attention to detail on imaging studies. Ultimately, this condition requires urgent surgical intervention. Delays in surgery or attempts to manage nonoperatively may result in poor outcomes.
Acknowledgements
The authors declare that they have no conflict of interests. This iteration of the manuscript was reviewed and agreed upon by all authors.
Informed consent for publication of their details was obtained from the patient prior to compilation of this manuscript.
- Keeratibharat N, Chansangrat J (2022) Gallbladder Volvulus: A Review. Cureus. 14: e23362.
- Beatty AS, Kulendran K,Iswariah H, Chandrasegaram MD (2023) Gallbladder volvulus with preoperative and intraoperative imaging. J Surg Case Rep. 2023: rjad048.
- Kashyap S, Mathew G, Abdul W, Ahmad H (2023) Gallbladder Volvulus. StatPearls.
- Pisano M, Allievi N, Gurusamy K. et al. (2020) World Society of Emergency Surgery updated guidelines for the diagnosis and treatment of acute calculus cholecystitis. World J Emerg Surg. 15: 61.
- Krishnamurthy G, Ganesan S, Ramas J, Damodaran K, Khanna A, Patta R (2021) Early laparoscopic cholecystectomy in acute gallbladder perforation: Single-centre experience. J Minim Access Surg. 17: 153-8.
- Lim LX, Mahin HH, Burnett D (2022) Gallbladder volvulus: An unexpected "twist". Radiol Case Rep. 17: 1755-9.
- Matías-García B, Sainz-Azara C, Mendoza-Moreno F, Díez-Alonso M, Gutiérrez-Calvo A (2023) Gallbladder Volvulus in an Elderly Patient: A Case Report and Review of Literature. Cureus. 15: e45167.
- Reilly DJ, Kalogeropoulos G, Thiruchelvam D (2012) Torsion of the gallbladder: a systematic review. HPB (Oxford). 14: 669-72.
- Chai JS, Wang X, Li XZ, Yao P, Yan ZZ, Zhang HJ, Ning JY, Cao YB (2020) Presentation of gallbladder torsion at an abnormal position: A case report. World J Clin Cases. 8: 2667-73.
- Abou Sleiman C, Terro JJ, Semaan DB, Nicolas G, El Shami J, et al. (2019) Gallbladder Volvulus: An Unusual Presentation. Am J Case Rep. 20:1879-82.
- Chin X, Ng JY (2021) Gallbladder Volvulus: An Uncommon Twist in Biliary Pathology. Cureus. 13: e20469.
- Sidhu K, Seyfi D, Crawford M, Watson G (2023) Gallbladder Volvulus in an Elderly Female With Severe Kyphoscoliosis. Cureus. 15: e36256.
- Kachi A, Nicolas G, Nasser J, Hashem M, Abou Sleiman C (2019) A Rare Presentation of Gall Bladder Volvulus: A Case Report. Am J Case Rep. 20: 1466-70.
- Chugh J, Davis B, Sandoval J, Soliman B (2023) Gallbladder Volvulus Masquerading as Acute Cholecystitis: A Case Report. Cureus. 15: e48529.
- Alkhalili E, Bencsath K (2014) Gallbladder torsion with acute cholecystitis and gross necrosis. BMJ Case Rep. 2016: bcr2014204917.
- Younan G, Schumm M, Ali F, Christians KK (2016) Gallbladder Volvulus in a Patient with Type I Choledochal Cyst: A Case Report and Review of the Literature. Case Rep Surg. 2016: 5626531.
- Chugh J, Davis B, Sandoval J, Soliman B (2023) Gallbladder Volvulus Masquerading as Acute Cholecystitis: A Case Report. Cureus. 15: e48529
FIGURE 1

Figure 1: Intraoperative image of necrotic, dilated gallbladder
FIGURE 2

Figure 2: Right upper quadrant ultrasound demonstrates a distended gallbladder with wall thickening, sludge, and pericholecystic fluid but without calculi
FIGURE 3
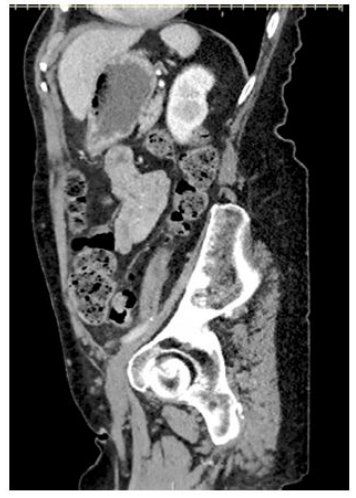
Figure 3: Sagittal CT slice demonstrates the presence of intramural air within the dilated gallbladder
FIGURE 4

Figure 4: The presence of a "beak" and "swirl" sign at the location of the gallbladder neck
FIGURE 5
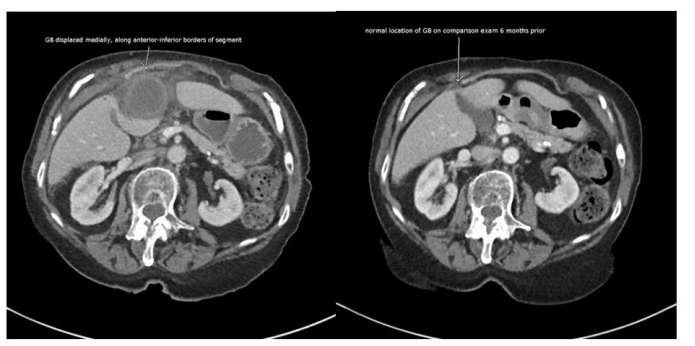
Figure 5: Axial CT slice demonstrates the relative displacement of the gallbladder compared to its location six months prior
FIGURE 6
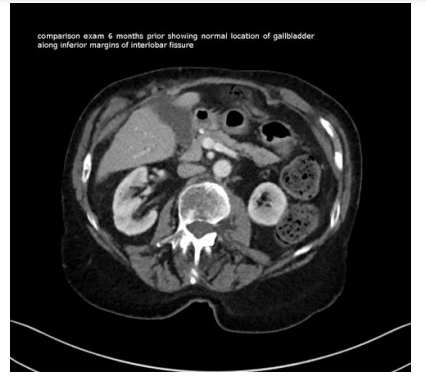
Figure 6: Axial CT scan slice that demonstrates previous normal anatomical location of gallbladder
FIGURE 7

Figure 7: Axial CT slice revealing the distance of separation of inflamed gallbladder from the interlobar fissure, displacement anteriorly and medially to its normal attachment
Figures at a glance