Urethral Stricture Combined with Urethral Scrotal Fistula Following Transurethral Resection of the Prostate: A Case Report and Literature Review
Received Date: September 04, 2024 Accepted Date: October 04, 2024 Published Date: October 07, 2024
doi: 10.17303/jspcr.2024.6.301
Citation: Mingkuan Zhou, Xiaoyuan Guo, Juan Lin, Jin-huan Wei, Hong-wei Zhao, et al. (2024) Urethral Stricture Combined with Urethral Scrotal Fistula Following Transurethral Resection of the Prostate: A Case Report and Literature Review. J Surg Proce Case Rep 6: 1-5
Abstract
Urethral scrotal fistula (USF) is a rare abnormal communication between the urethra and scrotum, often resulting from iatrogenic causes or secondary to stone perforation. This condition leads to painful scrotal swelling due to urine entering the scrotum through the fistula. We present a case of a 63-year-old male who developed urethral stricture complications following transurethral resection of the prostate (TURP). Postsurgery, the patient underwent blind catheterization with a urethral dilator multiple times, resulting in swelling and tenderness of the left scrotum. Bladder imaging revealed contrast agent from the urethra and prostate entering the scrotum through the fistula opening. The patient was successfully treated with urethral dilation, indwelling catheterization, and cystostomy. Urethral stricture is a common complication of prostatectomy. However, blind catheterization following stricture can lead to the formation of a false passage and USF. Clinicians should consider USF in cases of postoperative scrotal swelling and pain, alongside other differential diagnoses such as epididymitis.
Keywords: Urethral Scrotal Fistula; Urethral Stenosis; TURP
Case Report
A 63-year-old male patient was admitted to our hospital with scrotal swelling and pain persisting for over 20 days following a prostatectomy three months prior. His medical history includes presenting to a local hospital three months ago with recurrent urinary difficulty. At that time, he was diagnosed with benign prostatic hyperplasia (BPH) and underwent a transurethral resection of the prostate (TURP). The patient denied any history of diabetes, hypertension, or other relevant medical conditions. One year ago, the patient underwent surgical treatment for pneumothorax. Approximately one month ago, the patient experienced a diminished urine stream and sought medical attention for a suspected urethral stricture. Multiple catheterizations were performed, and urethral dilation was attempted. However, following the removal of the indwelling catheter, he experienced difficulty urinating and severe pain in the left scrotum. The local hospital's color Doppler ultrasound examination revealed a hydrocele or pyocele in the left testicular sheath and diffuse lesions in the scrotal soft tissue, suggesting infection. Consequently, the patient was diagnosed with epididymitis and treated with levofloxacin for anti-infective therapy for one week. Additionally, an ultrasound-guided aspiration of the fluid in the scrotum was performed, but there was no significant improvement in symptoms. Subsequently, a catheter was reinserted, and scrotal puncture with fluid extraction was performed under ultrasound guidance, revealing no bacterial growth upon culture and sensitivity testing. Due to persistent symptoms, the patient was referred to our hospital for further evaluation and management.
Upon admission, physical examination revealed an enlarged, tender, and tense left scrotum without palpable nodules or abnormalities of the testicles or penis. The pelvic CT scan and 3D reconstruction revealed fluid or pus accumulation between the corpus spongiosum of the penis and the scrotum (figure 1). Subsequently, a surgical incision and drainage were performed under local anesthesia (figure 2). Upon incision and drainage, the fluid was found to be pale yellow, raising the suspicion of urine leakage. Further evaluation through cystourethrography confirmed the presence of a urethral spongiosum-scrotal fistula, along with a urethral stricture at the prostatic segment. A diagnosis of urethral stricture with a urethral scrotal fistula (left) was confirmed (Figure 3).
On the tenth day following admission, the patient underwent urethral stricture dilation surgery and cold knife incision. Intraoperatively, an aberrant urethral passage was discovered, situated superior to the normal urethra and connecting to the penile base. Injection of water into this false passage resulted in its drainage through the left scrotum (Video1), further confirmed by methylene blue injection, which showed overflow from the false passage (Video2). Additionally, prostatic urethral stricture was visualized during urethroscopy. Cold knife incisions were performed at the 2 o'clock, 12 o'clock, and 10 o'clock positions, followed by dilation using a dilator. The procedure was uneventful, and a urethral balloon catheter was placed for continuous catheterization. Levofloxacin was administered for infection prophylaxis. On the third postoperative day, urinary flow persisted through the scrotum, indicating continued urine drainage alongside the catheter, necessitating redirection of the urinary stream. Consequently, a bladder fistula surgery was performed. The scrotal drainage strip was removed one week post-surgery, and the urinary catheter and cystostomy tube were replaced at one month. Both the urinary catheter and cystostomy tube were removed at two months postoperatively. Subsequent follow-up demonstrated unimpeded urination, absence of urine leakage from the scrotum, and no scrotal swelling.
Discussion
Urethral scrotal fistula is a rare abnormal passage often caused by stones or iatrogenic procedures. Previous literature has linked penile prosthesis implantation [1], ketamine abuse [2], and residual urinary tract in the urethra [3] to this condition. However, there are no reports of urethral scrotal fistula formation due to multiple catheterizations after prostatectomy. In this case, the patient experienced difficulty urinating post-electrocautery for benign prostatic hyperplasia. The use of an iron urethral dilator multiple times under blind vision led to excessive force, causing the probe to create a false passage outside the urethral lumen, connecting to the scrotum through the base of the penis. This resulted in painful inflammation and ultimately a penile scrotal fistula.
Studies have suggested that the occurrence of urethral strictures following benign prostatic hyperplasia surgery may be associated with iatrogenic injuries, prolonged preoperative indwelling urethral catheterization, preoperative infections, and prolonged postoperative indwelling catheterization. Therefore, it is crucial to assess and manage the patient's infection status prior to surgery, avoid excessive manipulation during surgical procedures, and minimize the duration of postoperative indwelling catheterization in order to reduce the incidence of postoperative urethral strictures.
Epididymitis is a common complication after prostatectomy [4], presenting with scrotal swelling and pain, which can mimic penile and scrotal fistula symptoms. Misdiagnosis as epididymitis occurred in this case, leading to a week of incorrect treatment. Ultrasound is crucial for diagnosing testicular swelling and pain post-prostatectomy. Retrograde urethrography (RU) and urinary bladder urethrography (VCU) are traditional diagnostic methods for penile and scrotal fistula but have limitations in evaluating surrounding tissues. Multidetector CT (MDCT) with reformatted images can provide more comprehensive information [5].
The mainstay of penile and scrotal fistula treatment is managing the urethral false passage. While the theoretical approach is resecting the false passage, clinical practice faces challenges due to the varying length and depth of the false passage, sometimes located behind the prostate urethra or in front of the rectum. Resection can lead to significant damage, excessive bleeding, and potential rectal injury. Resection may also involve damaging the internal and external sphincters, affecting sphincter function and causing urinary incontinence if the false passage is long and connected to the bladder neck. Treatment often focuses on diverting urine flow and widening the false passage. In this case, the urethral false passage healed fully two months post-surgery, likely due to its short formation time and non-epithelialized inner wall. Further cases are needed to determine the optimal surgical approach for partially epithelialized false passages that have not healed over time.
Conclusion
Urethral stricture combined with urethral scrotal fistula post-prostatectomy is a rare condition that can be mistaken for epididymitis. Clarification of the diagnosis typically requires ultrasound and CT imaging. Treatment options include urethral dilation, diverting urine flow, and addressing any urethral false passages.
- Parlak S, Okay AE (2016) Urethroscrotal Fistula: A Rare Cause of Scrotal Swelling. Pol J Radiol. 81: 438-40.
- Pavlica P, Barozzi L, Menchi I (2003) Imaging of male urethra.Eur Radiol. 13: 1583-96.
- Zhang XM, Hu WL, He HX, Lv J, Nie HB, et al. (2011) Diagnosis of male posterior urethral stricture: comparison of 64-MDCT urethrography vs. Standard urethrography.Abdom Imaging, 36: 771-5.
- Kuzaka B, Borkowsk T, Kuzaka P, Czaplicki M (2007) Epididymitis after prostatic adenomectomy--24-years observations. Przegl Lek. 64: 1018-21.
- Caoili EM, Cohan RH, Korobkin M, Platt JF, Francis IR, et al. (2002) Urinary tract abnormalities: initial experience with multi-detector row CT urography. Radiology. 222: 353-60.
FIGURE 1

Figure 1: CT scan shows left scrotal fluid accumulation and local
FIGURE 2

Figure 2: Left scrotum incision drainage, a large amount of urine is drawn out from the drainage port during urination
FIGURE 3
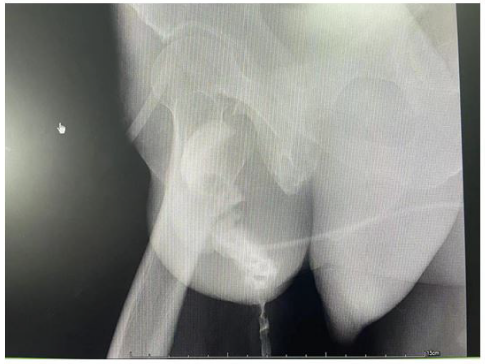
Figure 3: Cystourethrography shows that urine flows out of the left scrotum during urination
Figures at a glance