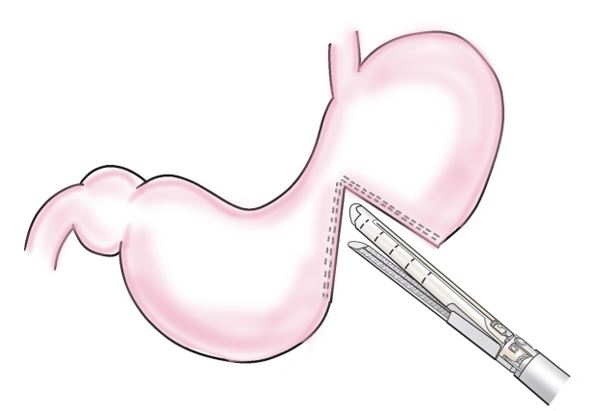
Figure 1: Step 1: Incomplete dissection of the stomach
The stomach was then incompletely dissected with a stapling device (3.5 mm/80 mm), leaving a 2–3 cm gastric angle on the lesser fold side.
Figure 1: Step 1: Incomplete dissection of the stomach
The stomach was then incompletely dissected with a stapling device (3.5 mm/80 mm), leaving a 2–3 cm gastric angle on the lesser fold side.
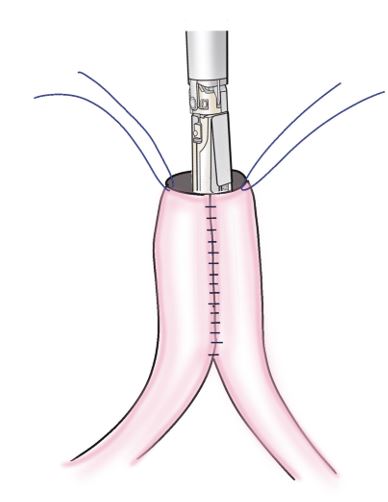
Figure 2: Step 2: Creation of jejunal pouch
The jejunal wall 30–40 cm from the ligament of Treitz bent and suture-separated with a stapler device, such that the suture line was on the contralateral side of the mesentery, to create a jejunal pouch.
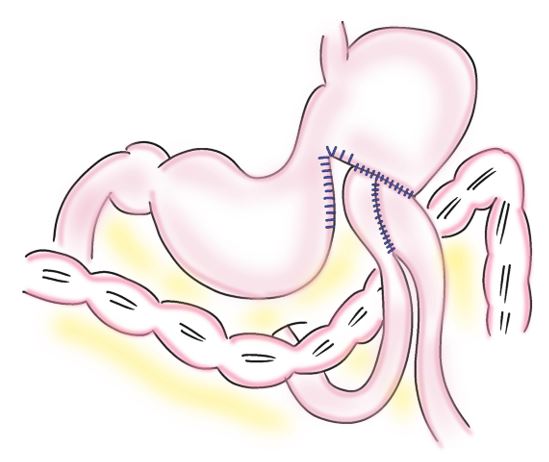
Figure 3: Step 3: Anastomosis of the jejunal pouch and stomach
An Albert-Lembert anastomosis was performed between an incompletely dissected oral segment of the stomach and the jejunal pouch using a 4-0 absorbable suture. The diameter of the anastomosis should match that of the jejunal pouch.
Tables at a glance
Figures at a glance