Hydrocele of the Canal of Nuck: A Forgotten Pathology
Received Date: October 05, 2025 Accepted Date: October 17, 2025 Published Date: October 21, 2025
doi:10.17303/jspcr.2025.7.104
Citation: Nuha Alsaleh, M.D (2025) Hydrocele of the Canal of Nuck: A Forgotten Pathology. J Surg Proce Case Rep 6: 1-8
Abstract
Background: A hydrocele of the canal of Nuck is an extremely rare anatomical abnormality observed in children. The disease results from the partial obliteration of the canal of Nuck, an anomalous peritoneal pouch that extends into the labia majora before the uterine round ligament. Inadequate obliteration of this canal, called patent processus vaginalis, can lead to a hydrocele or an inguinal hernia.
Aim: This review summarizes the disease pathology, clinical presentation, diagnosis, and management of hydrocele of the canal of Nuck.
Conclusion: The diagnosis of this rare disorder is primarily imaging-based, with ultrasonography being the most convenient method. The treatment is based on clinical presentation. The rarity of this disorder and the overlapping groin disorders complicate the diagnosis of this anatomical disease of early life.
Keywords: Canal of Nuck; Hydrocele; Imaging; Embryology
Introduction
Among females, the hydrocele of the canal of Nuck is a condition equivalent to a hydrocele of the spermatic cord among males. This condition is also known as "female hydrocele" (encysted hydrocele). During embryogenesis, processus vaginalis passes through the inguinal canal simultaneously as the round ligament or testis, which are on their way, respectively, into the labium majora or the scrotum. This takes place in the presence of both structures. The canal of Nuck closes for good in most humans at some point during the first year of their life. If a thorough obliteration is not accomplished, the patient risks developing a hydrocele or an indirect inguinal hernia. Both of these conditions can be quite painful. The anomaly has been named in honor of anatomist Anton Nuck of the 17th century [1].
The disorder has rarely been reported in detail in gynecological or surgical textbooks, and the case studies published to date are also scarce. The findings of the separate case studies have been summarized in Table 1. The disorder remains relatively unfamiliar to clinicians, frequently misdiagnosed as an abscess or inguinal hernia [2]. This study reviews the current literature to assist with the cause(s), diagnosis, and treatment of this detailed debilitating anatomical disorder.
Embryology and Anatomy
The canal of Nuck hydrocele is a disease of embryological origin involving both the processus vaginalis and the gubernaculum [10]. During the eighth to twelfth week of fetal development, a fibromuscular structure known as the gubernaculum emerges in the fetus. This structure continues down to the groin area of the fetus. In males, the distal part of the gubernaculum continues to expand to provide room for testicles to descend into the scrotum [1]. However, the absence of androgen prevents the expansion of the gubernaculum in females, which enables the gonadal tissue typically found in the pelvis to remain there [11].
The processus vaginalis is a parietal peritoneal invagination that enters the deep inguinal ring anteriorly to the gubernaculum. During the first trimester of pregnancy, the processus vaginalis develops. In males, it makes it easier for the gubernaculum to create a dilated pathway to descend testicles into the scrotum. The portion of processus vaginalis known as the canal of Nuck can be found in females' inguinal canals [11,12].
Disease Pathogenesis
At some point between the eighth month of pregnancy and the first year after birth, the canal of Nuck typically closes off completely in humans along the craniocaudal axis. This phenomenon occurs along the craniocaudal axis. Following the failure to complete closure can lead to communicative hydrocele and hernia. The fluid build-up originates from the fluid secretion from the processus vaginalis lined with mesothelial cells. This takes place when the proximal part of processus vaginalis shuts, but the distal portion of the vaginal opening stays open. The hydrocele will continue to become more rounded if there is a disparity between the fluid produced and the amount absorbed [1].
Classification
The hydrocele of the canal of Nuck can be classified into three main types:
Type 1: Encysted hydrocele is the most prevalent type of hydrocele. It forms the same way male encysted hydroceles do, when the proximal section of the canal closes, limiting contact between the peritoneal cavity and the rest of the body. It is usually unilocular and takes the shape of a comma or a mushroom [12].
Type 2: The hydrocele of type 2 develops when the peritoneal cavity is not closed off, and fluid can move freely between the abdominal cavity and the labia. Fluid will move into the labia when the patient stands erect because gravity will force it there. This explains the patients' descriptions of the lump as it appeared and then disappeared. Gradual compression can force fluid back into the abdomen and cause the palpable canal of the Nuck mass to collapse, resulting in patency maintained over time [13].
Type 3: Type 3 hydroceles, also known as hourglass hydroceles, are the rarest of the three and develop when a deep inguinal ring compresses a big hydrocele. A deep inguinal ring around the waist can appear like an hourglass or bilobar [2].
Clinical Presentation
Clinically, a canal of Nuck hydrocele may manifest as an achy or uncomfortable fluctuating inguinal mass; however, it is usually not accompanied by nausea or vomiting. Transillumination may occur if the mass is not reducible and large enough. There is a possibility of an indirect inguinal hernia developing as long as peritoneal evagination is patent [14].
Among females, inguinal swelling should be separated from abscesses, cysts, inguinal hernias, tumors (sarcoma, lipoma, and leiomyoma), and lymphadenitis. It is important to distinguish an inguinal hernia from the canal of Nuck in most instances; Hernias are frequently diagnosed in cases whereby the patency is sufficiently large to allow the omentum or bowel to protrude into the canal. This is a common cause of hernias. This is a typical timeframe for the diagnosis of hernias [1,15].
Radiological Diagnosis
The hydrocele diagnosis of Nuck's canal is based on Imaging analysis performed by expert radiologists [16,17]. Three prime imaging modalities can be used to diagnose this anatomical disorder in female children.
Ultrasound
Numerous medical specialists regard ultrasonography as the most effective modality for the initial imaging of canal of Nuck anomalies. This condition typically presents on ultrasound as a well-defined anechoic lesion exhibiting posterior acoustic amplification, which is characteristic of a hydrocele [3,16]. Figure 2 illustrates the ultrasonographic findings associated with all three types of anomalies. During an ultrasound examination, a lesion may appear hypoechoic or generate low-level echoes due to an elevated protein concentration. In instances where complications arise from a hydrocele, such as infection or hemorrhage, the lesion is likely to exhibit a complicated appearance, characterized by echogenic content, a thickened wall, or internal septations. This is indicative of an increased likelihood of such complications. The presence of a giant cyst may be connected to a smaller cyst with thin walls; both cysts may respond to the pressure applied by the transducer, potentially resulting in a "cyst-in-cyst" appearance, which could lead to misdiagnosis. To differentiate these findings from those of an imprisoned bowel loop, it is essential to utilize Doppler ultrasonography, which can provide clarity regarding the absence of visible color flow within the lesion [16,17].
Magnetic Resonance Imaging (MRI)
When the ultrasonography results are unclear, a magnetic resonance imaging (MRI) scan is performed to learn more about the herniated structures. In these patients, T1-weighted imaging typically reveals both a hypointense and a hyperintense canal of Nuck hydrocele. MRI can also assist in distinguishing the canal of Nuck from soft-tissue tumors that might manifest as a palpable lump in the inguinal region [10].
Computed Tomography (CT)
Owing to the radiation emitted by a CT scan, it is not a primary imaging tool used to assess a mass in the groin. CT imaging may show a well-defined low-density collection in cases where the inguinal canal is relatively uncomplicated. Regardless of how basic or complicated they are, do not exhibit any sign of contrast enhancement [10-17].
Management
The canal of Nuck can present as acute or persistent discomfort, in addition to infections of the hydrocele. Even though there are a significant number of reported cases of hydroceles, the vast majority do not require emergency surgical intervention. However, surgical intervention may be required for a small fraction of patients presenting with infections, tumors, or herniations [16].
Surgical treatment for a cyst in the Canal of Nuck consists of two components: the excision of the cystic structure and the simultaneous closure of the inguinal defect, which can be done with or without mesh. The cyst can be removed surgically, and the prosessus vaginalis can be closed, which may make it feasible to reduce the frequency with which the condition returns. The choice of the most effective surgical procedure is based on various factors, including the seriousness of the underlying disorder, the presence of an inguinal hernia, the accuracy of the preoperative diagnosis, and a few other considerations [1].
Depending on the circumstances, if an inguinal hernia is discovered simultaneously, a hernia repair may be performed concurrently, with or without mesh insertion. When the mass extends to the labia majora, an extra vulva repair could be recommended as a treatment option. An intraoperative photograph of a hydrocele of the canal of Nuck is shown in Figure 3.
Although laparoscopic excision has become more common in recent years, people with a Nuck cyst canal and an indirect inguinal hernia may consider having laparoscopic surgery. This is due to “laparoscopic surgery can remove both the canal of the Nuck cyst and the indirect inguinal hernia [17,18]. Even if there is only a tiny cyst, laparoscopic excision can likely cause the inner ring to grow, necessitating the implantation of a patch [19].
As a consequence of this, surgeons have to select the most appropriate method for diagnosing and treating a canal of Nuck cyst based on several factors, such as the woman's age, the presence of an inguinal hernia at the same time, and the patient's intention to become pregnant shortly. In addition, cyst aspiration may assist in alleviating symptoms, even though it is not recommended as a treatment in and of itself [1].
Conclusion
Canal of Nuck is the male analog of female processus vaginalis; nevertheless, it is significantly less well-known than processus vaginalis. Radiologists rarely encounter this rare condition, especially in adults, because it is unusual. In addition, the canal of Nuck disease might be more common than was previously believed, and it ought to be considered a potential cause of groin discomfort in the differential diagnosis. It is essential to have a solid grasp of the embryology and anatomy of the canal of Nuck to correctly diagnose the myriad of pathological conditions that might develop in this region. In addition, physicians need to be familiar with this entity to create an accurate and comprehensive differential diagnosis for a labial mass or swelling.
- Keeratibharat N, Chansangrat J (2022) Hydrocele of the Canal of Nuck: A Review. Cureus. 14.
- Holley A (2018) Pathologies of the canal of Nuck. Sonography. 5: 29-35.
- Wang L, Maejima T, Fukahori S, Shun K, Yoshikawa D, Kono T (2021) Laparoscopic assisted hydrocelectomy of the canal of Nuck: a case report. Surg Case Rep. 7: 52.
- Wang L, Maejima T, Fukahori S, Shun K, Yoshikawa D, Kono T (2021) Laparoscopic surgical treatment for hydrocele of canal of Nuck: A case report and literature review. Surg Case Rep. 7: 121.
- Zvizdic Z, Milisic E, Chikha A, Sefic I, Dzananovic A, Vranic S (2019) Encysted hydrocele of the canal of Nuck in an 11-month-old child with a past history of duodenal atresia and Arnold-Chiari malformation: A case report. Medicine (Baltimore). 98: e14232.
- Janssen K, Klinkner D, Kumar T (2011) Encysted hydrocele of canal of nuck: a case report with review of literature. J Surg Tech Case Rep. 3: 97-8.
- Sarkar S, Panja S, Kumar S (2016) Hydrocele of the Canal of Nuck (Female Hydrocele): A Rare Differential for Inguino-Labial Swelling. J Clin Diagn Res. 10: Pd21-2.
- Vinoth T, Lalchandani A, Bharadwaj S, Pandya B (2022) Revisiting the clinico-radiological features of an unusual inguino-labial swelling in an adult female. Int J Surg Case Rep. 98: 107515.
- Khanna PC, Ponsky T, Zagol B, Lukish JR, Markle BM (2007) Sonographic appearance of canal of Nuck hydrocele. Pediatr Radiol. 37: 603-6.
- Nasser H, King M, Rosenberg HK, Rosen A, Wilck E, Simpson WL (2018) Anatomy and pathology of the canal of Nuck. Clinical Imaging. 51: 83-92.
- Rosa F, Martinetti C, Veirana MA, Attieh A, Trisoglio A, Sabattini R, et al. (2021) How embryology knowledge can help radiologists in the differential diagnosis of canal of Nuck pathologies. La radiologia medica. 126: 910-24.
- Brainwood M, Beirne G, Fenech M (2020) Persistence of the processus vaginalis and its related disorders. Australasian Journal of Ultrasound in Medicine. 23: 22-9.
- Sarkar S, Panja S, Kumar S (2016) Hydrocele of the canal of Nuck (female hydrocele): a rare differential for inguino-labial swelling. Journal of clinical and diagnostic research: JCDR. 10: PD21.
- Sethi V, Patel H (2016) Hydrocele in the Canal of Nuck-CT appearance of a developmental groin anomaly. Journal of radiology case reports. 10: 29.
- Kono R, Terasaki H, Murakami N, Tanaka M, Takeda J, Abe T (2015) Hydrocele of the canal of Nuck: a case report with magnetic resonance hydrography findings. Surgical Case Reports. 1: 1-5.
- Fikatas P, Megas I-F, Mantouvalou K, Alkatout I, Chopra SS, Biebl M, et al. (2020) Hydroceles of the canal of Nuck in Adults—Diagnostic, treatment and results of a rare condition in females. Journal of clinical medicine. 9: 4026.
- Wang L, Maejima T, Fukahori S, Shun K, Yoshikawa D, Kono T (2021) Laparoscopic surgical treatment for hydrocele of canal of Nuck: a case report and literature review. Surgical Case Reports. 7: 1-6.
- Lee SR (2022) Laparoscopic Hydrocelectomy of Encysted Hydrocele of the Canal of Nuck with High Ligation in Children or Iliopubic Tract Repair in Adults. J Laparoendosc Adv Surg Tech A. 32: 684-9.
- Kohata A, Hirata Y, Ishikawa S, Kai A, Namba Y, Okimoto S, et al. Large hydrocele of the canal of Nuck diagnosed and treated using conventional and laparoscopic methods. Journal of Surgical Case Reports. 2020: rjaa222.
FIGURE 1
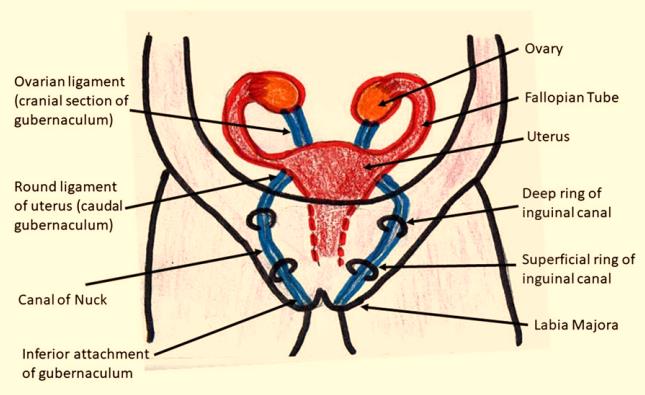
Figure 1: Diagrammatic depiction of embryological attachment of gubernaculum that occurs from female gynecological organs to labia majora.
FIGURE 2

Figure 2: The ultrasound shows the hydrocele of Nuck's canal. The arrow illustrates a comma-shaped hydrocele attenuated by the fluid.
FIGURE 3
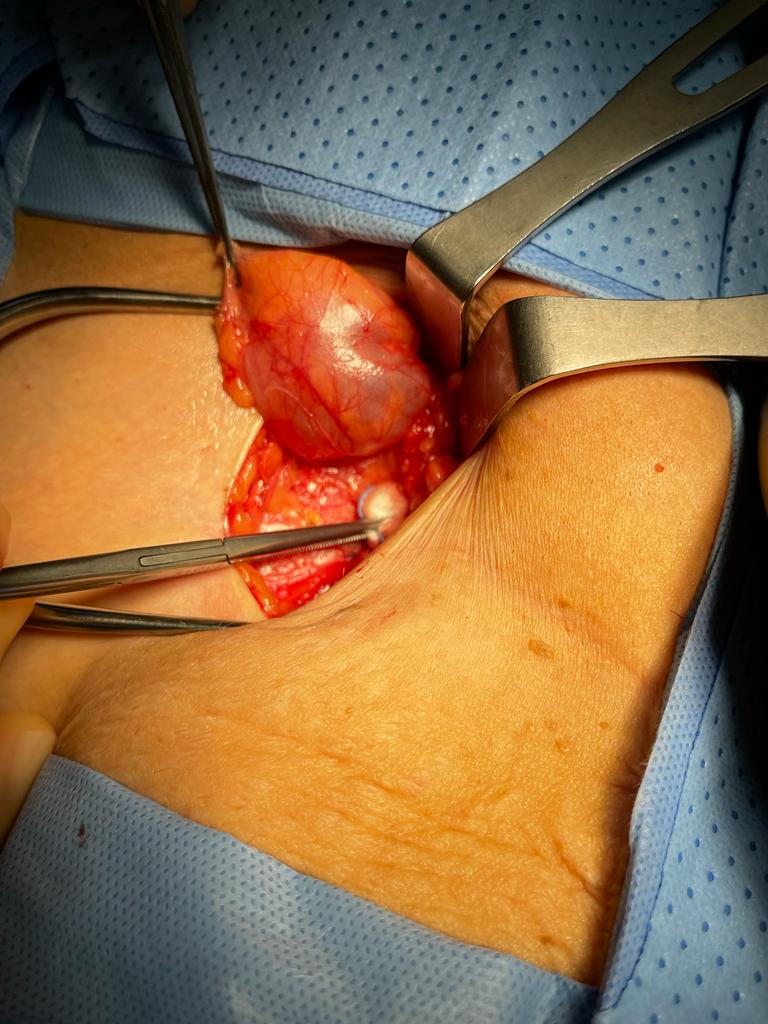
Figure 3: Intraoperative picture of a hydrocele of the canal of Nuck
Tables at a glance
Figures at a glance