The "System-Reset" Framework for Unstable Peritrochanteric Fractures in the Ultra-Elderly: Decoupling Mechanical Stability from Biological Latency via Primary Arthroplasty
Received Date: January 14, 2026 Accepted Date: January 31, 2026 Published Date: February 03, 2026
doi:10.17303/jspcr.2026.8.101
Citation: Chi-Ming Chiang (2026) The ‘’System-Reset’’ Framework for Unstable Peritrochanteric Fractures in the Ultra-Elderly: Decoupling Mechanical Stability from Biological Latency via Primary Arthroplasty. J Surg Proce Case Rep 8: 1-11
Abstract
Background: Unstable peritrochanteric fractures (AO/OTA 31-A2/A3) in ultra-elderly patients challenge internal fixation because both sliding hip screws and cephalomedullary nails remain substrate-limited by osteoporotic cancellous purchase. We propose that treating hip fractures in the super-elderly is not merely a biological reconstruction but a systems-stability problem (i.e., ensuring reliable early load acceptance). Unlike internal fixation, which relies on stochastic biological healing, the 'System-Reset' via arthroplasty provides an immediate, deterministic restoration of mechanical stability (a step-change in load acceptance)."
Objective: To formalize a “System-Reset” framework that treats primary arthroplasty as a deterministic strategy for immediate load acceptance in biologically latency-limited hosts, and to describe an “In-Situ Reconstruction Algorithm” that reduces technical complexity in comminuted extracapsular patterns.
Methods: Stability is modeled as purchase potential × device mechanism. Arthroplasty is modeled as a variable substitution that replaces cancellous purchase with a more deterministic stem–canal (often cement-augmented) interface. Five radiographic figures and two conceptual phase diagrams illustrate the framework.
Illustrative applications: A four-step protocol—envelope preservation, non-dislocation strategy, in-situ neck resection, and centripetal reduction via cement–stem “hydrostatic splinting”—achieved immediate construct stability in illustrative examples, enabling full weight-bearing mobilization within 48 hours.
Conclusion: For ultra-elderly patients with unstable peritrochanteric fractures and limited biological reserve, primary arthroplasty can function as a mechanical override that decouples postoperative mobility from fracture-healing latency.
Transparency statement: This manuscript is a concept-and-technique article using illustrative, de-identified radiographs to demonstrate decision logic and operative mechanics; it is not intended as outcome-based clinical research.
Keywords: Ultra-Elderly; Unstable Intertrochanteric Fracture; Peritrochanteric Fracture; Primary Arthroplasty; Hemiarthroplasty; Cemented Stem; Early Mobilization; Mechanical Stability
1. Introduction
Hip fracture is a rapidly expanding global burden as population’s age, and unstable extracapsular patterns increasingly concentrate in the highest-risk segment of the age distribution. Epidemiologic syntheses forecast a steep rise in worldwide hip fracture incidence over coming decades, with a growing contribution from Asia [1].
We define the 'biologically latency-limited' host operationally as patients aged ≥80 years (or ≥75 with ASA score ≥3) who exhibit severe osteoporosis (cortical thickness index <0.4) and limited physiological reserve, for whom the 3–4-month biological healing latency of internal fixation poses an unacceptable mortality risk." Contemporary hip fracture pathways therefore prioritize early operative management and accelerated mobilization as core determinants of survival and functional recovery, because immobility itself is a medically destabilizing exposure in frail hosts [2,3].
Operational definitions (for clinical applicability): In this article, “ultra-elderly” refers to patients aged ≥85 years (or ≥80 years with marked frailty), and “biologically latency-limited” refers to hosts in whom the expected fracture-healing reserve is clinically constrained by a high frailty burden (e.g., dependence in basic activities of daily living or a high clinical frailty score), severe osteoporosis/poor cancellous purchase (radiographic osteopenia, opportunistic CT/HU surrogates when available), and limited physiologic reserve such that prolonged protected weight-bearing is not realistic. These criteria are intended as pragmatic triggers for considering a deterministic stability strategy rather than as strict eligibility rules.
Within this landscape, unstable peritrochanteric fractures (AO/OTA 31-A2/A3) represent a specific mechanical dilemma: comminution compromises the medial buttress, shifts loading toward shear, and converts small errors in implant–bone interface behavior into catastrophic collapse. The classic tip-apex distance paradigm made explicit that fixation failure often localizes at the screw–bone interface, even when reduction and implant placement appear technically acceptable [4,5].
Device-selection debates frequently focus on “sliding hip screw versus intramedullary nail.” However, high-quality randomized evidence suggests that, across broad trochanteric fracture populations, many one-year outcomes are similar, implying that the dominant driver of failure in a subset of ultra-elderly patients is not the device class but the substrate: severely osteoporotic purchase [6,7].
This manuscript proposes that in the boundary condition where cancellous purchase becomes a stochastic and unreliable variable, the correct question is not which fixation construct is optimal, but whether fixation remains a rational system choice at all. Systematic reviews comparing primary arthroplasty with proximal femoral nailing in unstable intertrochanteric fractures consistently emphasize earlier weight-bearing and shorter hospitalization after arthroplasty, albeit with trade-offs in operative time and blood loss [8].
Older comparative work already framed arthroplasty not merely as salvage but as a strategy to minimize mechanical failure and to enable rapid functional recovery in unstable intertrochanteric and subtrochanteric fracture patterns. A guideline-synthesis perspective similarly reinforces that the ultimate objective is reliable early mobilization when biological reserve is limited [9,10].
2. Conceptual Framework: Stability Transformation and “System Reset”
We define the operative problem as a systems-stability problem rather than a purely anatomical one. Internal fixation aims to maintain alignment while biological consolidation progresses; by design, functional stability is time-dependent and rises only as the fracture heals. In the ultra-elderly with severe osteoporosis, the dominant failure mode becomes substrate-limited: the implant can only be as reliable as the cancellous bone that must purchase it.
In a simplified model, the effective stability of fixation (S_fixation) can be expressed as the product of (i) purchase potential (P_bone), a function of bone density and microarchitecture (ρ), and (ii) mechanism factor (M_device), representing the mechanical philosophy of the implant:
S_fixation(t) = P_bone(ρ) × M_device
As age approaches the tenth decade in frail patients, ρ may approach a functional lower bound, such that P_bone(ρ) → ε. In this boundary condition, S_fixation collapses regardless of M_device, and the risk of cut-out, toggle, and varus collapse becomes dominated by the screw–bone interface [4,5].
Primary arthroplasty is modeled as a variable substitution: the stochastic purchase term is replaced by a more deterministic stem–canal interface (often cement-augmented in osteoporotic hosts), and immediate load acceptance becomes feasible. Conceptually, arthroplasty functions as a hybrid construct: the stem provides intramedullary load transfer (analogous to a cephalomedullary device’s lever-arm reduction), while the prosthetic articulation provides rotational dissipation and immediate functional motion.
S_arthroplasty ≈ C_implant × (M_stem + M_articulation)
This framing does not assert that arthroplasty is universally superior. Rather, it proposes a decision boundary: when the cumulative probability of fixation failure during the biological latency interval dominates the one-time procedural complexity cost of arthroplasty, a “system reset” becomes rational.
This decision boundary and the resulting decoupling of immediate mechanical stability from biological latency are schematized as a phase portrait.
3. Methods and Operative Strategy: The In-Situ Reconstruction Algorithm
Scope note: The following content presents an operative algorithm and illustrative radiographic material to communicate conceptual and mechanical logic; it does not report comparative clinical outcomes or effect sizes.
This manuscript presents a conceptual framework coupled with a reproducible operative algorithm and illustrative radiographic material selected to demonstrate the operative logic and mechanical implications of the proposed system-reset strategy, rather than as a case series or outcome-based clinical study. The clinical endpoint is immediate construct reliability sufficient to permit full weight-bearing mobilization within 48 hours—an endpoint aligned with modern hip-fracture care pathways emphasizing early surgery and early mobilization in frail patients.2,3
A four-step “In-Situ Reconstruction Algorithm” was developed to reduce the technical complexity cost of arthroplasty in comminuted extracapsular fractures by minimizing energy input into an unstable fracture field. The technique treats the prosthesis and cement mantle not solely as a replacement, but as an intramedullary reduction and stabilization device operating within a preserved soft-tissue envelope.
The operative logic can be further conceptualized as navigating a procedural complexity landscape, in which high-torque dislocation and forceful impaction represent a higher-complexity trajectory (“high-perturbation path”), whereas the in-situ strategy aims to follow a lower-entropy trajectory (“low-perturbation path”) with reduced surgical perturbation.
3.1 Step 1: Envelope preservation (biological tension-band containment)
A modified lateral approach is used with muscle splitting rather than extensive detachment. The comminuted intertrochanteric zone is not widely exposed. By preserving the peri-fracture soft-tissue sleeve, fragment divergence is mechanically constrained, analogous to maintaining a closed-system boundary condition.
3.2 Step 2: Non-dislocation strategy (boundary-condition conservation)
Hip dislocation is intentionally avoided. The limb is maintained in controlled rotation and length. In unstable A2/A3 morphologies, high-torque maneuvers associated with dislocation can disrupt comminuted fragments and transform a contained comminution into gross displacement. Working in situ aims to preserve the minimum-energy configuration already enforced by capsular and soft-tissue tension.
3.3 Step 3: In-situ neck resection (strategic decoupling)
Through an anterior capsulotomy, the femoral neck is resected in situ while preserving the intertrochanteric ring. This step decouples the compromised head–neck unit from the load pathway while maintaining containment of the trochanteric fragments.
3.4 Step 4: Centripetal reduction via cement–stem hydrostatic splinting
A cemented stem is inserted with deliberate avoidance of aggressive impaction. The stem functions as a mandrel within the canal, promoting centripetal re-expansion of collapsed proximal fragments against the preserved envelope. The cement mantle behaves as a “hydrostatic splint,” integrating stem, shaft, and contained fragments into a composite construct while minimizing impact-induced crack propagation.
4. Illustrative Applications (Representative Radiographic Examples)
Representative radiographs (Figures 1–5) are presented to illustrate how primary arthroplasty transforms an unstable peritrochanteric fracture from a time-dependent fixation problem into an immediately load-accepting system. Figure 1 demonstrates a preoperative unstable peritrochanteric morphology with proximal comminution and the immediate postoperative restoration of a functional hip center after primary cemented hemiarthroplasty. Lateral views further demonstrate establishment of a stable intramedullary load pathway (Figure 2, right). Serial follow-up imaging shows maintained implant position with progressive peri-trochanteric osseous response without early mechanical failure (Figure 3). A separate representative example demonstrates an unstable extracapsular fracture managed with primary total hip arthroplasty using a long-stem construct spanning the comminuted proximal segment (Figure 4), with composite imaging highlighting alignment and load-transfer continuity across pre-existing lower-extremity arthroplasty implants (Figure 5).
The images were selected from four elderly women aged 78–96 years who sustained unstable peritrochanteric or extracapsular hip fractures following low-energy falls. Although comorbidities varied—including prior cerebrovascular accident with residual hemiplegia, advanced frailty with severe osteoporosis, and pre-existing lower-extremity arthroplasty—each patient shared a common boundary condition of limited biological reserve and unreliable cancellous bone purchase. In this setting, primary arthroplasty was selected to prioritize deterministic early load acceptance, enabling full weight-bearing mobilization within 48 hours. These radiographic examples are intended to demonstrate operative and system-level logic rather than to report comparative clinical outcomes.
Consistent with this framing, prior studies have reported earlier weight-bearing and shorter hospitalization with primary arthroplasty in unstable intertrochanteric fractures, while acknowledging trade-offs related to operative invasiveness.8,9 The corresponding conceptual schematics are provided in Figures 6 and 7.
5. Discussion
The central claim of the “System-Reset” framework is that, in a subset of ultra-elderly patients, the dominant determinant of construct reliability is not implant sophistication but cancellous bone purchase. When purchase potential collapses toward a functional minimum, fixation becomes probabilistic regardless of whether a sliding hip screw or a cephalomedullary nail is selected [4,5].
Randomized trials comparing intramedullary nails with sliding hip screws in trochanteric fractures have often shown modest or no clinically meaningful differences in many one-year outcomes. This observation supports a substrate-dominant interpretation: when bone quality is sufficiently compromised, the screw–bone interface becomes the common bottleneck across device classes [6,7].
Primary arthroplasty addresses this bottleneck by substituting a stem–canal interface for cancellous purchase and by permitting immediate functional loading. Systematic reviews suggest that arthroplasty can provide earlier weight-bearing and shorter hospital stay in unstable patterns, although it may increase operative time and blood loss and does not uniformly improve long-term functional scores [8].
Historically, the principal critique of arthroplasty-first strategies in extracapsular comminution has been technical: exposure, dislocation, and aggressive manipulation can destabilize trochanteric fragments, increase bleeding, and raise the risk of complications. The in-situ reconstruction algorithm is designed specifically to reduce this complexity cost by preserving the soft-tissue envelope, avoiding dislocation-related torque, and using the cement–stem complex as an internal reduction device rather than as a passive replacement.
From a geriatric-medicine perspective, the value of deterministic early stability is that it directly supports care pathways prioritizing rapid mobilization and reduction of immobilization-related morbidity. Guidelines and guideline summaries repeatedly emphasize these pathway objectives, reinforcing why “immediate system reliability” may be a rational endpoint in biologically latency-limited hosts [2,3,10].
This manuscript has limitations. The cases are illustrative and do not provide comparative outcome estimates. The mathematical formalism is intentionally simplified to clarify decision logic rather than to generate quantitative predictions. Future work should prospectively operationalize the boundary condition of “biological latency limitation” using reproducible metrics (eg, frailty indices and opportunistic bone-quality measures) and should compare early mobility, complications, and health-economic outcomes against best-practice internal fixation in unstable A2/A3 patterns.
Ultimately, the System-Reset strategy exemplifies a 'Physics-Informed Orthopedics' approach. By prioritizing mechanical determinism over biological uncertainty, we can effectively reduce instability and immobility-related risk of the aging skeletal system. This concept aligns with broader principles of load-transfer continuity and early stability control, suggesting a unified framework for managing geriatric fragility."
6. Conclusion
In ultra-elderly patients with unstable peritrochanteric fractures and limited biological reserve, the operative objective may shift from anatomical restoration to system reliability. The proposed “System-Reset” framework conceptualizes primary arthroplasty as a mechanical override that decouples postoperative mobility from fracture-healing latency by substituting a more deterministic implant interface for osteoporotic cancellous purchase. The accompanying in-situ reconstruction algorithm aims to reduce the technical complexity cost of arthroplasty in comminuted extracapsular fractures and to operationalize immediate load acceptance as a clinically meaningful endpoint.
Declarations
Ethics approval and consent to participate
Not applicable (conceptual framework with illustrative de-identified radiographs).
Consent for publication
Radiographs are anonymized. Publication consent should be obtained according to institutional policy and local regulations.
Availability of data and materials
Not applicable.
Competing interests
The author declares no competing interests.
Funding
None.
Authors’ contributions
CMC conceived the framework, developed the operative algorithm, and drafted the manuscript.
Acknowledgements
None.
- Dhanwal DK, Dennison EM, Harvey NC, Cooper C (2011) Epidemiology of hip fracture: Worldwide geographic variation. Indian J Orthop. 45: 15-22.
- National Institute for Health and Care Excellence. Hip fracture: management (NICE guideline CG124). Updated 2023 Jan 6. London: NICE; 2023.
- American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: Evidence-based clinical practice guideline. Rosemont (IL): AAOS; 2021 Dec 3.
- Baumgaertner MR, Curtin SL, Lindskog DM, Keggi JM (1995) The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J Bone Joint Surg Am. 77: 1058-64.
- Baumgaertner MR, Solberg BD (1997) Awareness of tip-apex distance reduces failure of fixation of trochanteric fractures of the hip. J Bone Joint Surg Br. 79: 969-71.
- Parker MJ (2017) Sliding hip screw versus intramedullary nail for trochanteric hip fractures; a randomised trial of 1000 patients with presentation of results related to fracture stability. Injury. 48: 2762-7.
- Schemitsch EH, Nowak LL, Schulz AP, Brink O, Poolman RW, Mehta S, et al. (2023) Intramedullary nailing vs sliding hip screw in trochanteric fracture management: The INSITE randomized clinical trial. JAMA Netw Open. 6: e2317164.
- Chen WH, Guo WX, Gao SH, Wei QS, Li ZQ, He W (2021) Arthroplasty vs proximal femoral nails for unstable intertrochanteric femoral fractures in elderly patients: A systematic review and meta-analysis. World J Clin Cases. 9: 9878-88.
- Haentjens P, Casteleyn PP, De Boeck H, Handelberg F, Opdecam P (1989) Treatment of unstable intertrochanteric and subtrochanteric fractures in elderly patients: Primary bipolar arthroplasty compared with internal fixation. J Bone Joint Surg Am. 71: 1214-25.
- O'Connor MI, Switzer JA (2022) AAOS clinical practice guideline summary: Management of hip fractures in older adults. J Am Acad Orthop Surg. 30: e1291-6.
FIGURE 1
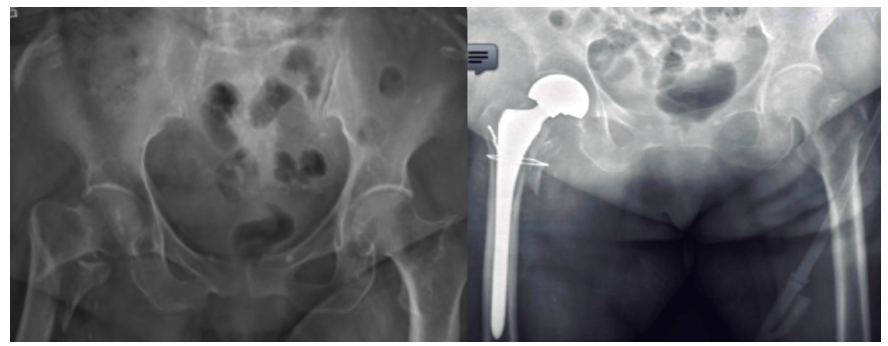
Figure 1: Preoperative anteroposterior (AP) pelvis radiograph demonstrating an unstable peritrochanteric fracture with proximal comminution (left). Immediate postoperative AP pelvis radiograph after primary cemented hemiarthroplasty with adjunctive trochanteric stabilization (right).
FIGURE 2
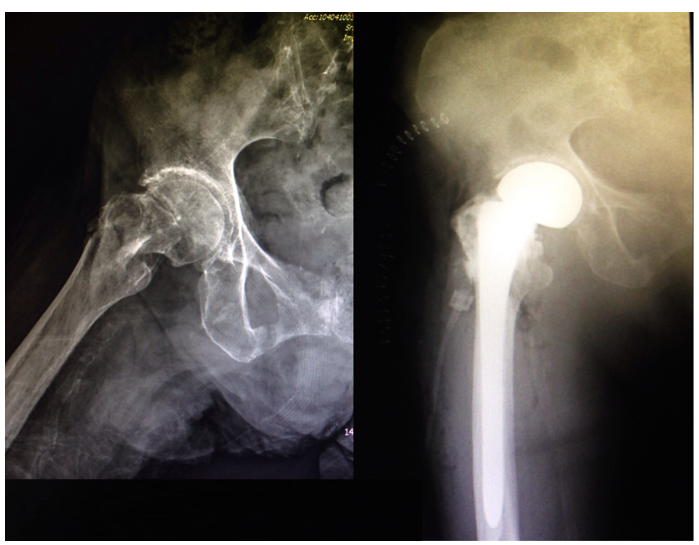
Figure 2: Lateral radiographs of the affected hip showing preoperative unstable extracapsular fracture morphology (left) and postoperative lateral radiograph demonstrating stem position and restoration of the proximal load pathway after primary arthroplasty (right).
FIGURE 3

Figure 3: Serial radiographs demonstrating (from left to right) preoperative AP pelvis, immediate postoperative AP pelvis, later follow-up AP pelvis, and follow-up lateral view. The construct maintains position while peritrochanteric osseous response/consolidation develops around the proximal femur.
FIGURE 4

Figure 4: Preoperative AP radiograph demonstrating an unstable intertrochanteric/peritrochanteric fracture morphology (left). Postoperative AP radiograph after primary total hip arthroplasty, illustrating acetabular component fixation and a long-stem construct spanning the comminuted proximal segment (right).
FIGURE 5
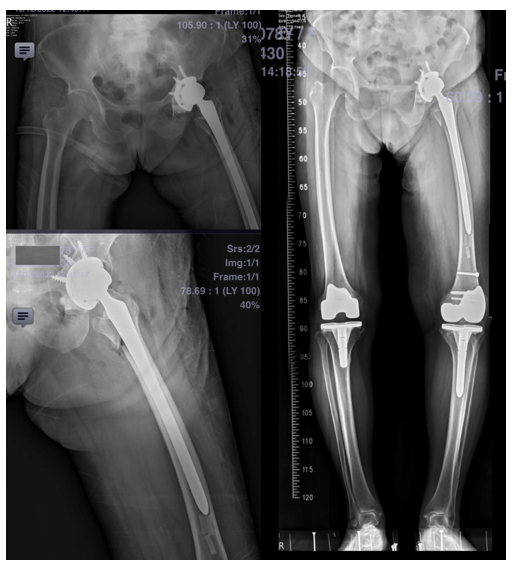
Figure 5: Composite postoperative imaging including AP pelvis (upper left), lateral hip/femur view (lower left), and standing full-length lower-extremity alignment view (right). The long-stem hip construct coexists with bilateral total knee arthroplasties, highlighting alignment and load-transfer considerations in geriatric patients with multiple arthroplasty implants.
FIGURE 6
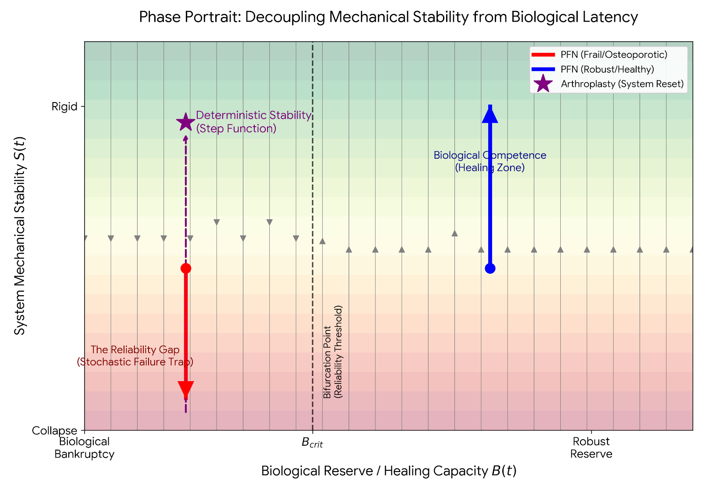
Figure 6: Conceptual phase portrait illustrating the “System-Reset” decision boundary that decouples immediate mechanical stability S(t) from biological reserve/healing capacity B(t). The diagram contrasts probabilistic fixation trajectories in frail/osteoporotic hosts (reliability gap) with competent healing trajectories in robust hosts, and models primary arthroplasty as a deterministic stability step (“system reset”) across the reliability threshold (B_crit).
FIGURE 7
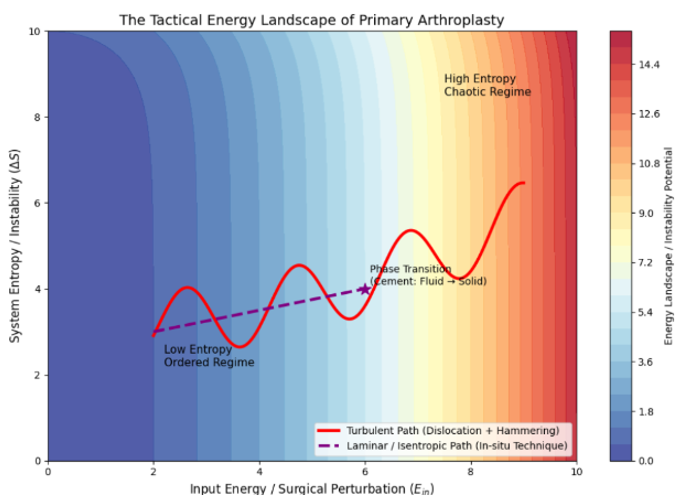
Figure 7: Conceptual “tactical energy landscape” of primary arthroplasty. The schematic contrasts a higher-entropy operative trajectory (“high-perturbation path,” eg, dislocation plus forceful impaction) with a lower-entropy in-situ/isentropic trajectory that minimizes surgical perturbation while achieving the phase transition to a stable load-accepting construct.
In clinical terms, this trajectory represents the transition from a reliance on callus formation (slow, uncertain) to immediate implant stability (fast, deterministic).
Figures at a glance