The Impact of Dienogest (2mg) on the Quality of Life of Women with Endometriosis
Received Date: February 07, 2023 Accepted Date: March 07, 2023 Published Date: March 10, 2023
doi: 10.17303/jwhg.2023.10.101
Citation: DFátima Faustino, José Lourenço Reis, Filipa Osório, Rui Viana, et al. (2023) The Impact of Dienogest (2mg) on the Quality of Life of Women with Endometriosis. J Womens Health Gyn 10: 1-12
Abstract
Background: Endometriosis is a chronic, often progressive and relapsing disease, characterized by the presence of endometrial glands and stroma outside the uterine cavity. Endometriosis affects woman's life globally, therefore the subjective assessment of the patient’s quality of life is central to the management of endometriosis. Currently, there is a lack of medical options as well as real word data regarding dienogest treatment.
Objective: To evaluate the impact of dienogest in health-related quality of life in patients with endometriosis.
Study design: Non-interventional, prospective and multicenter study. Women with endometriosis were eligible to enroll,regardless of previous treatment. Women received dienogest 2 mg once daily as part of their routine clinical practice. Quality of life was assessed through the Portuguese validated endometriosis health profile-30 (EHP-30) questionnaire at the baseline (beginning of the treatment) and at 3- and 6-months following treatment.
Results: A total of 88 women were screened for eligibility of which 86 (97.7%) were enrolled. From those, only 47 participants (54.7%) completed the study. EHP-30 scores improved at 3- and 6-months in all the five studied domains.Treatment with dienogest for 6 months elicited a mean change of -25.0 ± 25.0 (mean ± SD) in control and powerlessness domain (95% CI: -33.2; -18.9), followed by pain (–22.6 ± 23.4 ;95% CI: -30.4;-17.0), emotional wellbeing (–18.0 ± 22.7 ;95% CI: -25.5;-12.2), social support (–15.9 ± 26.0 ;95% CI: -20.6;-4.7), and self- image (–11.1 ± 28.5 ;95% CI: -24.3;-9.0), The percentage of patients with improvement in EHP-30 scores was the highest for control and powerlessness scale at both timepoints evaluated.
Conclusion: Treatment with dienogest 2 mg once-daily in women with endometriosis effectively reduced EHP-30 score,improving quality of life in a short-period as 3 months, with continued progress at 6 months.
Keywords: Dienogest; Endometriosis; EHP-30; Pain; Quality of Life
Introduction
Endometriosis is a chronic, often progressive and relapsing disease, characterized by the presence of endometrial glands and stroma outside the uterine cavity [1]. Globally, it is estimated that endometriosis affects approximately 10% of women of reproductive age [2]. The multifactorial nature of this disease hinders the diagnosis and often delays early intervention, demanding the collaboration of a multidisciplinary team.
Clinically, endometriosis is manifested by dysmenorrhea,chronic pelvic pain, dyspareunia, dysuria,dyschezia, infertility and abnormal uterine bleeding, among others. However, as the symptomatology is very heterogeneous among patients, it can take 6–10 years to diagnose endometriosis [3]. The symptomatologic pattern often affects physical, emotional and social morbidity which, by consequence, decrease quality of life [4,5]. Health-related quality of life is a multidimensional and dynamic concept that encompasses physical, psychologicaland social aspects related to a disease or its treatment. Given that endometriosis affects woman's life globally, the subjective assessment of the patient’s quality of life is central to the management of endometriosis [6].
The Endometriosis Health Profile Questionnaire-30 (EHP-30) is currently the most widely used and validated questionnaire to assess quality of life in women with endometriosis [4,7]. The EHP-30 contains 30 questions divided into five subcategories, addressing pain,control and powerlessness, emotional wellbeing, social support and self-image domains. It is recommended by the American Society for Reproductive Medicine (ASMR) and the European Society for Human Reproduction and Embryology for research on health-related quality of life in endometriosis [8,9]. Distinct studies have shown that EHP-30 is sensitive to changes in health status in patients with endometriosis over time [10-12]. This questionnaire has already been validated in several languages, such as Spanish [13], Swedish [14], Brazilian [15], Chinese [16] and also in Portuguese [8].
Currently, the medical management of endo- metriosis aims to improve symptoms and the related pain or to prevent the recurrence of postsurgical disease[6]. Hormonal treatments such as combined oral contraceptives and progestins are the first therapeutic choice in order to mimetize a hyperprogestogenic environment. By doing that, these medicines inhibit ovulation, decidualization, and result in a decrease in the size of the lesions [1]. Dienogest is an oral progestin with a strong progestogenic effect, resulting in pronounced endometrial lesion reduction [17]. This drug lacks significant androgenic, mineralocorticoid, or glucocorticoid activity and presents good tolerability, potentiating its long-term use. Of note, multiple evidence showed that the prolonged dienogest treatment sub- stantially improves endometriosis-related pain symptoms [18,19]. Thus, dienogest might present a promising first-line treatment option for the long-term management of debilitating endometriosis-associated symptoms, and consequently, quality of life [12,20]. In comparison with gonadotropin-releasing hormone (GnRH) agonists, dienogest demonstrated comparable efficacy in reducing endometriosis pain-associated symptoms with less adverse events [21]. Importantly, identical results are achieved with combined oral contraceptives (COCs) for the relief of endometriosis-associated pelvic pain and improvement in health-realted quality of life [22].
To date, real word data of the impact of dienogest treatment on quality of life are lacking. Thus, the present study aimed to evaluate the effect that endometriosis has on women's quality of life, using the EHP-30 questionnaire, before starting treatment with dienogest (2 mg/daily) and 3 and 6 months after starting the treatment. Understanding this information can help to improve counseling for women. Furthermore, this study will allow us to deepen our knowledge of the Portuguese reality about the quality of life of women with endometriosis, to evaluate the effect that endometriosis has on women's lives, as well as to identify factors that influence their quality of life, taking into account consideration of several dimensions (pain, sense of control and powerlessness, emotional well-being, social support and self-image).
Methods
Study Design
This study was a non-interventional, prospective and multicentric study conducted in routine clinical practice settings. The study recruited 88 women with endometriosis for whom a decision of being treated with dienogest 2 mg/daily (Zafril®, Gedeon Richter Plt., Hungary) was made by the physician according to the local health authority approved label. No additional diagnostic proce¬dure was applied. Patients who fulfilled all the eligibility criteria were invited by their gynecologist to participate in the study and all patients signed a written informed consent form prior to their admission. The study was approved by the competent Ethics Committee and conducted in accordance with the Declaration of Helsinki.
Study Population
Women with at least 18 years of age, with clinical or surgical diagnosis of endometriosis, with endometriosis associated pelvic pain and/or dysmenorrhea and women that were physically and psycho¬logically able to participate in the study were eligible. Women were excluded if they had any known adverse reactions to the active substance or to any of the excipients, if they were participating in an investigational program with interventions outside of routine clinical practice and if women were exposed to other medicine or medical device in investigation in the 6 months prior to recruiting. The study also excluded patients with a current or recent history of drug or alcohol abuse, and participants with a serious illness, mental disorder or any other cause that could impact their participation.
Data Collection
Following the initial explanation of the study and the signature of the informed consent form by the women, the physician filled a clinical questionnaire where clinical information about the woman was collected (time of diagnosis, method of diagnosis, classification of endo- metriosis, symptoms presented and previous treatment of endometriosis). Women were asked to respond to the Endometriosis Health Profile Questionnaire-30 (EHP-30) validated Portuguese version. The information collected comprised sociodemographic characteristics (age, educ- ation, occupation and marital status) and questions to measure the effect that endometriosis has on women's quality of life. Women answered the questionnaire in person at day 0 (before the start of treatment) and by telephone at day 90 (approximately 3 months) and at day 180 (approximately 6 months) after the treatment started. The questionnaires were performed between January 2021 and June 2022.
The Endometriosis Health Profile-30 (EHP-30)
The EHP-30 contains 30 questions divided into five subcategories. These categories address key problem-areas which are transversally reported by women with endometriosis: pain (questions 1 to 11), control and powerlessness (questions 12 to 17), emotional wellbeing (questions 18 to 23), social support (questions 24 to 27) and self-image (questions 28 to 30). When women were answering EHP-30, they were asked to recall their experience in the last 4 weeks using never, rarely, sometimes, often or always (five-point Likert scale (0–4)). Each scale was translated into a score ranging from 0 (best possible health status) to 100 (worst possible health status) by dividing the subscale scores by the maximum possible raw score within the subscale and multiplying it by 100. Changes in EHP-30 domains scores were categorized in deterioration, no change and improvement. These cat- egories were defined as >0, 0 and < 0 difference in EHP-30 scores, respectively.
Statistical Analysis
SData collected using the questionnaires were cleaned and coded. Data were entered and analyzed using SPSS Statistics for Windows, Version 21.0 (Armonk, NY: IBM Corporation). Proportions, arithmetic means, medians, minimum, maximum and standard deviations (SD) were used as summary statistics. In addition, skewness of score distribution and kurtosis were used to describe the distribution of item responses as well as 95% confidence intervals (CI).
Wilcoxon signed rank test was used to test for statistically significant differences between baseline and follow-up timepoints. P-value < 0.05 indicated a statistically significant change.
Results
Participants
A total of 88 women were screened for eligibility of which 86 (97.7%) were enrolled. From those, only 47 participants (54.7%) completed the study (Figure 1). Among the 39 women who did not complete the study, 21 were drop-out at 3 months’ follow-up and the remaining 18 at 6 months’ follow-up questionnaire. Voluntary with- drawal and loss to follow-up were the main reasons identified.
A summary of the characteristics of the patients is presented in Table 1. The average age of the sample was 35 ± 8 years old, ranging from 18 to 49 years old. In their majority, women had a university degree (bachelor’s degree or higher, 60.5%), were married or living in common-law marriage (57.0%) and were working (79.1%).
In regard to clinical endometriosis characteristics, 73.3% of the women only had a confirmatory diagnosis based on the clinical framework and 33.7% (n=29) had stage IV endometriosis, according to the ASMR clas- sification. Considering the symptoms experienced in the past four weeks (in relation to the time when baseline questionnaire was completed), most women reported dysmenorrhea (72.1%), chronic pelvic pain (66.3%) and dyspareunia (57.0%) (Table 1). Also, at baseline, most of the recruited women (66.3%) had been subject to a prior treatment. Hormonal therapy (41.9%, n=36) was the most used followed by surgery (26.7%, n=23).
The Effectiveness of Dienogest to Change Health Related Quality of Life
Scores for all EHP-30 core scales improved during the first 3 months of dienogest therapy and continued to improve until month 6 (Table 2). At baseline, the control and powerlessness dimension had the highest average score (64.0) and therefore was the one with the main negative impact on health-related quality of life. In turn, the self-image dimension had the lowest average score (54.6). At 6 months’ follow-up, all the five dimensions seemed to weigh the same in the overall health related quality of life (Table 2).
Treatment with dienogest for 6 months elicited a mean change of -25.0 ± 25.0 (mean ± SD) in control and powerlessness domain (95% CI: -33.2; -18.9), followed by pain (–22.6 ± 23.4 ;95% CI: -30.4;-17.0), emotional wellbeing (–18.0 ± 22.7 ;95% CI: -25.5;-12.2), social support (–15.9 ± 26.0 ;95% CI: -20.6;-4.7), and self- image (–11.1 ± 28.5 ;95% CI: -24.3;-9.0), (Table 2).
At 3- and 6-months follow-up, dienogest treatment had the greatest impact on control and powerlessness and pain domains (Table 3). Percentage of patients with improvement in EHP-30 scores was the highest for control and powerlessness scale (Figure 2).
In the control and powerlessness domain, the proportion of women with improvement of the EHP-30 score at 6 months was 85.1% (n=40) whereas 4.3% (n=2) reported no change and 10.6% (n=5) showed a deteriorated state. In the pain domain, 78.7% (n=37), 6.4% (n=3) and 14.9% (n=7) reported improvements, no changes and deterioration, respectively. The self-image domain was the dimension in which fewer women reported improvements (53.2%, n=25).
Additional sub-analyses detected no clear correlations between the rate of improvement in EHP-30 scores and clinical characteristics at baseline such as method of diagnosis, endometriosis stage or the presented symptomatology.
Discussion
Although both pharmacological as well as surgical treatment of endometriosis can improve the patients’ quality of life, the available therapeutics target the sym- ptomatology rather than the etiology of the disease.
Dienogest reduces endometriotic lesions and it is associated with relatively moderate inhibition of gon- adotropin secretion, leading to a modest reduction in the endogenous production of estradiol. When given continuously, dienogest induces a hypoestrogenic, hyper- gestagenic local endocrine environment, causing a decidualization of endometrial tissue followed by atrophy of the endometriotic lesions. Animal studies indicate that dienogest may also reduce plasma estradiol levels directly, through inducing apoptosis of granulosa cells in the ovary [19]. Moreover, the efficacy of dienogest 2 mg daily has been extensively studied in randomized clinical trials for endometriosis related symptoms, demonstrating that long-term use (about 2 and half years) effectively reduced endometriosis-associated pelvic pain and avoided pain rec- urrence post-surgery [12,19,23]. Nevertheless, real-world studies in different worldwide populations are lacking in order to provide evidence to consolidate the routine clinical practice.
From our study, the therapeutic with dienogest 2 mg once daily significantly improved health-related quality of life in the five studied domains in Portuguese women. Health-related quality of life was evaluated through the validated questionnaire EHP-30. It is noteworthy that, just after 3 months of dienogest therapy, 72.7% of the women reported improved EHP-30 scores in pain and control and powerlessness domain, 71.2% improvements in emotional well-being and 63.9% and 59.1% in social support and self-image domains, respectively. Following the same trend, 6 months of therapy with dienogest 2 mg daily improved the EHP-30 scores in 85.1%, 78.7%, 72.3%, 63.8% and 53.2% of the recruited women in control and powerlessness, pain, emotional well-being, social support and self-image domains, respectively.
The data obtained with this study is in line with previous observations. Over 36-months treatment with dienogest therapy, patients with rectosigmoid endo- metriosis reported continuous improvement in EHP-30 scores [24]. Similarly, in patients with persistent pain associated with endometriosis, 6-month treatment with dienogest increased health-related quality of life [25]. In similar clinical settings to this study but in Asian women, the ENVISIOeN study also demonstrated significant improvement in health-related quality of life measured by the EHP-30 at 6 and 24 months following dienogest therapy [12]. Altogether, the available data seems to indicate that dienogest is able to improve health-related quality of life, in all of the associated domains, in a short-time period (3 to 6 months). of note, and besides dienogest did not provide the highest proportion of patients reporting improvement in the pain domain, maximum values for this category were the ones with greatest variation (baseline: 94.2 compared to 6 months follow up 78.2). This data supports the importance of dienogest in controlling endometriosis associated pain, in line with the existent randomized clinical trials results where dienogest therapy significantly reduces pain in endometriosis patients, namely debilitating chronic pelvic pain [19,26,27].
To the best of our knowledge, this is the first study evaluating the impact of dienogest therapy in Portuguese women with endometriosis. Still, this study has some limitations. Firstly, as the women were recruited by medical centers referral, the high intensity/severity of symptoms may be overrepresented. Of note, 33.7% of the participants had stage IV endometriosis. However, this is a common limitation transversal to the majority of clinical studies. Secondly, the participation rate was low while the dropout rate was high. Although a higher participation rate would increase the confidence intervals, it is unlikely that an increased number of participants would drastically change the results. Moreover, the difficulty in recruitment of a representative sample is a widely recognized challenge in endometriosis studies [28]
Conclusion
The results of this study suggest that dienogest 2 mg once daily improves health related quality of life just in the first three months of therapy with continuous improvements throughout time. Therefore, dienogest presents itself as a satisfying option for the long-term management of endometriosis among Portuguese women
Acknowledgments
The authors would like to thank their colleagues for participating in this study. Data collection, statistical and editorial support were performed by an independent committee, with funding from Gede¬on Richter Plc.
Conflict of Interest
The authors have no conflict of interest in re¬lation to this article to disclose
Patient Consent Statement
All patients signed a written informed consent form prior to their admission. The study was approved by the competent Ethics Committee and conducted in accordance with the Declaration of Helsinki
- França PR de C, Lontra ACP, Fernandes PD (2022) Endometriosis: A Disease with Few Direct Treatment Options. Molecules 27: 4034.
- Malvezzi H, Marengo EB, Podgaec S, De Azevedo Piccinato C (2020) Endometriosis: current challenges in modeling a multifactorial disease of unknown etiology Background: setting and disease. J Transl Med 18: 311.
- Nezhat C, Vang N, Tanaka PP, Nezhat C (2019) Optimal Management of Endometriosis and Pain. Obstet Gynecol 134: 834-9.
- Corte L Della, Di Filippo C, Gabrielli O et al. (2020) The burden of endometriosis on women’s lifespan: A narrative overview on quality of life and psychosocial wellbeing. Int. J. Environ. Res. Public Health 17: 1-17.
- Ben-Meir LC, Soriano D, Zajicek M et al. (2020) The Association between Gastrointestinal Symptoms and Transvaginal Ultrasound Findings in Women Referred for Endometriosis Evaluation: A Prospective Pilot Study. Ultraschall der Medizin
- Ruszała M, Dłuski DF, Winkler I et al. (2022) The State of Health and the Quality of Life in Women Suffering from Endometriosis. J Clin Med 11: 2059.
- Khong SY, Lam A, Luscombe G (2010) Is the 30-item Endometriosis Health Profile (EHP-30) suitable as a self-report health status instrument for clinical trials? Fertil Steril 94: 1928-32.
- Nogueira-Silva C, Costa P, Martins C et al. (2015) Validation of the portuguese version of EHP-30 (The endometriosis health profile-30). Acta Med Port 28: 347-56.
- Vincent K, Kennedy S, Stratton P (2010) Pain scoring in endometriosis: entry criteria and outcome measures for clinical trials. Report from the Art and Science of Endometriosis meeting. Fertil Steril 93: 62-7.
- Van De Burgt TJM, Kluivers KB, Hendriks JCM (2013) Responsiveness of the Dutch Endometriosis Health Profile-30 (EHP-30) questionnaire. Eur J Obstet Gynecol Reprod Biol 168: 92-4.
- Jones G, Jenkinson C, Kennedy S (2004) Evaluating the responsiveness of the endometriosis health profile questionnaire: The EHP-30. Qual. Life Res 13: 705-13.
- Techatraisak K, Hestiantoro A, Soon R et al. (2022) Impact of Long-Term Dienogest Therapy on Quality of Life in Asian Women with Endometriosis: The Prospective Non-Interventional Study ENVISIOeN. Reprod Sci 29: 1157-69.
- Marí-Alexandre J, García-Oms J, Agababyan C et al. (2020) Toward an improved assessment of quality of life in endometriosis: evaluation of the Spanish version of the Endometriosis Health Profile 30. J Psychosom Obstet Gynecol 1-7.
- Grundström H, Rauden A, Wikman P, Olovsson M (2020) Psychometric evaluation of the Swedish version of the 30-item endometriosis health profile (EHP-30). BMC Womens Health 20: 1-8.
- Mengarda CV, Passos EP, Picon P et al. (2008) Validação de versão para o português de questionário sobre qualidade de vida para mulher com endometriose (Endometriosis Health Profile Questionnaire - EHP-30). Rev Bras Ginecol e Obstet 30: 384-92.
- Jia SZ, Leng JH, Sun PR, Lang JH (2013) Translation and psychometric evaluation of the simplified Chinese-version Endometriosis Health Profile-30. Hum Reprod 28: 691-7.
- Vannuccini S, Clemenza S, Rossi M, Petraglia F (2022) Hormonal treatments for endometriosis: The endocrine background. Rev Endocr Metab Disord 23: 333.
- Lee JH, Song JY, Yi KW et al. (2018) Effectiveness of Dienogest for Treatment of Recurrent Endometriosis: Multicenter Data. Reprod Sci 25: 1515-22.
- Schindler AE (2011) Dienogest in long-term treatment of endometriosis. Int J Womens Health 3: 175.
- Alcalde AM, Martínez-Zamora MÁ, Gracia M et al. (2022) Assessment of Quality of Life, Sexual Quality of Life, and Pain Symptoms in Deep Infiltrating Endometriosis Patients with or Without Associated Adenomyosis and the Influence of a Flexible Extended Combined Oral Contraceptive Regimen: Results of a Prospective, Observational Study. J Sex Med 19: 311-8.
- . Bedaiwy MA, Allaire C, Alfaraj S (2017) Long-term medical management of endometriosis with dienogest and with a gonadotropin-releasing hormone agonist and add-back hormone therapy. Fertil Steril 107: 537-48.
- . El Taha L, Abu Musa A, Khalifeh D et al. (2021) Efficacy of dienogest vs combined oral contraceptive on pain associated with endometriosis: Randomized clinical trial. Eur J Obstet Gynecol Reprod Biol 267: 205-12.
- . Römer T (2018) Long-term treatment of endometriosis with dienogest: retrospective analysis of efficacy and safety in clinical practice. Arch Gynecol Obstet 298: 747-53.
- Barra F, Scala C, Maggiore ULR, Ferrero S (2020) Long-Term Administration of Dienogest for the Treatment of Pain and Intestinal Symptoms in Patients with Rectosigmoid Endometriosis. J Clin Med 9: 154.
- Morotti M, Sozzi F, Remorgida V et al. (2014) Dienogest in women with persistent endometriosis-related pelvic pain during norethisterone acetate treatment. Eur J Obstet Gynecol Reprod Biol 183: 188-92.
- Strowitzki T, Faustmann T, Gerlinger C et al. (2015) Safety and tolerability of dienogest in endometriosis: pooled analysis from the European clinical study program. Int J Womens Health 7: 393.
- Lang J, Yu Q, Zhang S, et al. (2018) Dienogest for Treatment of Endometriosis in Chinese Women: A Placebo-Controlled, Randomized, Double-Blind Phase 3 Study 148-55.
- Verket NJ, Andersen MH, Sandvik L et al. (2018) Lack of cross-cultural validity of the Endometriosis HealthProfile-30. J Endometr Pelvic Pain Disord 10: 107.
FIGURE 1
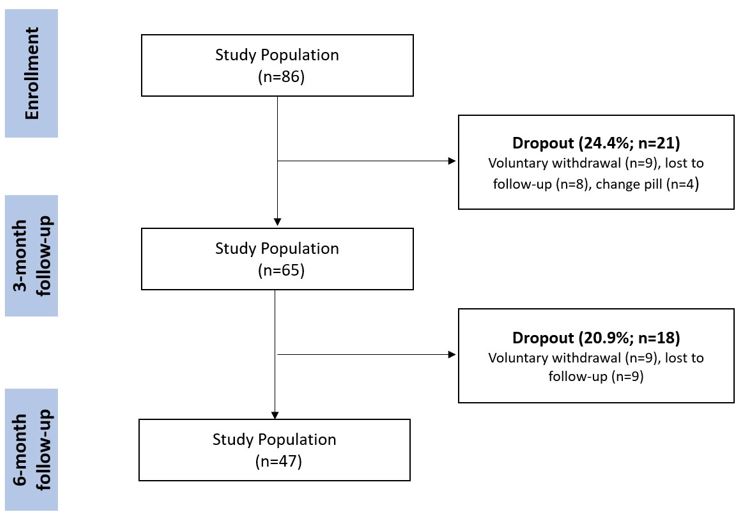
Figure 1: Flow diagram of the study, schematizing the women progress
FIGURE 2
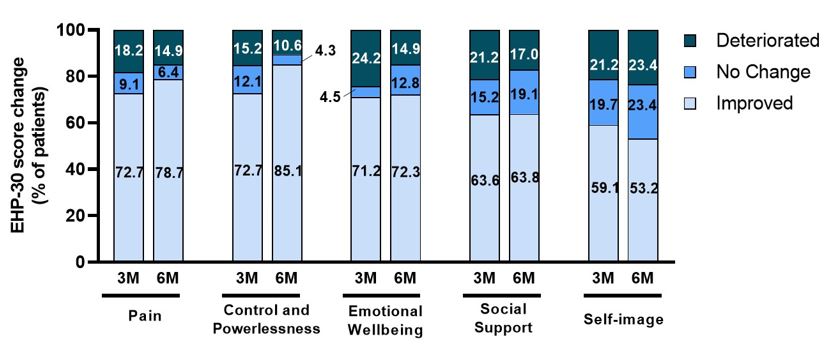
Figure 2: Changes in core EHP-30 scores from baseline to month 3 (3M) and to month 6 (6M) Results demonstrate proportions of patients with deterioration, no change and improvement defined as >0, 0 and < 0 difference in EHP-30 scores between baseline and questionnaires at month 3 and 6. Data were analyzed in 66 and 47 patients after 3- and 6-months follow-up, respectively. EHP-30, Endometriosis Health Profile-30 questionnaire
Tables at a glance
Figures at a glance