Prevalence of High-Risk Human Papillomavirus Serotypes and Confrontation with Available Vaccine Antigens: The Case of Cameroon
Received Date: May 26, 2023 Accepted Date: June 26, 2023 Published Date: June 29, 2023
doi: 10.17303/jwhg.2023.10.103
Citation: Ebong CE, Nzang JL, Nyada SR, Essiben F, Tompeen I et al. (2023) Prevalence of High-Risk Human Papillomavirus Serotypes and Confrontation with Available Vaccine Antigens: The Case of Cameroon. J Womens Health Gyn 10: 1-12
Abstract
Background: Cervical cancer, caused by oncogenic human papillomavirus (HPV) serotypes, is a devastating disease in the developing world, even though it is preventable and treatable. Cameroon currently offers immunization against only two high-risk HPV types (16 and 18), and screening for cervical cancer by testing for HPV is limited to pilot centers.
We therefore carried out this study to determine the prevalence of oncogenic serotypes of HPV in asymptomatic women of reproductive age attending cervical cancer screening in Yaoundé, Cameroon, to confront this data with available vaccines, and to identify some factors associated with HPV infection.
Methodology: We did a hospital based retrospective descriptive and analytical study at two hospitals of the Cameroon Baptist convention (CBC), located at the Etoug-Ebe and Ekoumdoum neighborhoods, in Yaoundé, which offer cervical cancer screening through HPV DNA testing. The study period was from February 2020 to December 2021.
Results: The prevalence of high-risk HPV was 41.8%. The non 16/18 HPV types were the most common (81.0%) type of high-risk HPV. HPV 16 and 18 had prevalence of 9.2% and 9.8%, respectively. The prevalence of high-risk HPV was associated with HIV-positivity.
Conclusion: The prevalence of high-risk HPV is higher than previously reported in the country. The prevalence of non-16/18 serotypes is disproportionately higher than that of types 16 and 18. The lone factor associated with HPV infection in this study was the existence of infection with the HIV.
Keywords: Cervical Cancer; Human Papillomavirus; Screening; High-Risk; Cameroon
Background
Cervical cancer is a devastating disease, yet it is preventable and treatable. There were about 604,000 new cases of invasive cervical cancer and 342,000 deaths from the disease globally in 2020, according to the global cancer observatory (GLOBOCAN). It is the fourth most common cancer in women after breast, colo-rectal and lung cancers, with a proportion of 6.5% [1] and the trend is not abating, with some 700,000 new cases and 400,000 deaths expected in 2030 [2].
About 80% of cases of cervical cancer occur in low- and medium-income countries (LMICs) [1,3], where the implementation of approved prevention strategies is lagging. In sub-Saharan Africa, cervical cancer is the second most common cancer in women (with a proportion of 23.3%), after breast cancer (27.3%). The sub-region accounts for 18.3% of global incidence and its 21.3% contribution to global cervical cancer mortality [1] reflects other weaknesses in the management of the disease. In Cameroon, there were about 2,770 new cases of cervical cancer in 2020, making it the second most common cancer in women, after breast cancer – with proportions of 22.6% and 34.1%, respectively [1]. However, in some Cameroonian studies, cervical cancer ranks first ahead of breast cancer [4,5]. Cervical cancer is, therefore, a real public health problem in Cameroon too.
In contrast, in the United States where cervical cancer was once one of the most common causes of cancer deaths among women [6], there are now eight new cases of invasive cervical cancer and two deaths per 100,000 women per year; an incidence sixteen times less than that of breast cancer [7]. Currently, cervical pre-cancers are diagnosed far more often than invasive cervical cancers [6], highlighting the benefits of implementation of screening.
Cervical cancer is a disease characterized by abnormal proliferation and aggressive transformation of the cells of the uterine cervix, the lower part of the uterus (womb) that opens into the upper part of the vagina. It is considered a sexually transmitted disease because it is caused by some (oncogenic) types of a sexually transmitted virus, the human papillomavirus (HPV). In addition to having a known etiology, cervical cancer has a long and detectable pre-invasive phase, making it vulnerable for elimination. Its control can be achieved through prevention of HPV infection – through immunization and sex education – and through timely detection and treatment of pre-cancerous lesions. Immunization against HPV has been launched in many countries to contribute to infection prevention in adolescents before the initiation of sexual activity.
The vaccines are safe and effective in preventing infections with HPV viruses, high-grade precancerous lesions and invasive cancer [8]. However, major vaccination programs target peri-pubertal girls and major benefits of their immunization on cancer occurrence are only expected after decades. Accordingly, the prevention of this cancer, especially in populations of adult women, will still have to rely on the early detection of persistent HPV infection by deoxyribonucleic acid (DNA) testing or the presence of precancerous lesions by visual methods or by cytology.
There is a current shift towards high-risk HPV DNA testing as the preferred screening method for cervical cancer. HPV DNA testing is more objective, simpler, more efficient in preventing pre-cancer and cancer, and more cost-effective. It also gives room for self-sampling [9]. In Yaoundé, Cameroon, high-risk HPV DNA testing is offered by the Cameroon Baptist convention (CBC) health services at 10,000 francs CFA (16.1 USD) and by the Centre Pasteur du Cameroun laboratory at 10,500 francs (16.9 USD). This is about the same amount charged for Pap smear, and the results are usually issued after about fourteen days for both tests. Visual inspection with acetic acid plus visual inspection with Lugol’s iodine costs about 4,500 francs CFA (7.3 USD) in public and confessional health facilities and the results are generally issued immediately after the procedure.
The World Health Organization (WHO) recommends that women start screening at age 30 (25 for women living with the human immunodeficiency virus (HIV)) and to repeat it every 5 to 10 years (every 3-5 years for women living with HIV) [9]. The WHO’s global strategy for cervical cancer elimination – endorsed by the World Health Assembly in 2020 – proposes a 90-70-90 global target by 2030 for the progressive containment of cervical cancer. This means:
- 90% of girls are fully vaccinated with HPV vaccine by age 15 years.
- 70% of women are screened with a highperformance test by age 35 and again by age 45 years
- 90% of women identified with cervical disease receive treatment (90% for women with precancer,and 90% for women with invasive cancer).
If these targets are met, even in the LMIC’s, about 300,000 deaths could be averted by 2030 and median cervical cancer incidence could fall by 42% by 2045 [2]. This would take us closer to the threshold incidence of 04 per 100,000 women-years set for the elimination of cervical cancer as a public health problem [2].
The HPV vaccines target a variable number of HPV serotypes recognized as important causes of cervical and other cancers – in both females and males – or genital warts. Globally, serotypes 16 and 18 are known to cause at least 70% of cervical pre-cancers and cancers [10]. In Cameroon, HPV vaccination was scaled-up in 2020 [11,12] and the choice of vaccines currently administered (Cervarix® and Gardasil®) – both of which contain antigens of types 16 and 18 – was probably based on the generic data above. This is because we found only a few studies on prevalence of a few oncogenic serotypes published before the scale-up of immunization in the country. Furthermore, the prevalence of HPV 16 and 18 in women and in pathology samples from these reports were modest [13,14]. Obviously, knowing the prevailing serotypes of HPV in the country could help inform on the choice of vaccine for the country’s vaccination program against cervical cancer, if optimum impact is the quest.
We therefore carried out this study to determine the prevalence of oncogenic serotypes of the HPV in a population of asymptomatic women of reproductive age attending cervical cancer screening in Yaoundé, Cameroon and to confront this data with the antigens covered by vaccines available in the country. We also sought to identify some factors that could be associated with this infection
Methodology
Study Design
We did a descriptive and analytic study with retrospective data collection at two hospitals in Yaoundé belonging to the faith-based organization, the Cameroon Baptist convention (CBC). These two hospitals located at the Etoug-Ebe and Ekoumdoum neighborhoods, in Yaoundé, each have a ‘women’s health programs’ (WHP) department that offers cervical cancer screening through HPV DNA testing. They are part of a network of 94 health facilities located in seven of the 10 regions of Cameroon.The study took place between April and September 2022 but included data from February 2020 to December 2021. The study population included files of women received at the WHP departments of the two hospitals for screening by HPV DNA testing during the period of study. All complete files of women screened during the study period were included. Records with inadequate HPV test results were excluded.
Procedure
After we obtained ethical clearance from the ethics committee of the faculty of medicine and biomedical sciences of the University of Yaoundé 1 and from the CBC Health Service Institutional Review Board, we proceeded to obtain permission to recruit from the management of the Etoug-Ebe and Ekoumdoum Baptist health complexes in Yaoundé. In these institutions, cervical cancer screening was performed using the Ampfire HPV DNA test (Atila Biosystems Ltd). The test enables qualitative detection of 15 high-risk HPV (HR HPV) types (16, 18, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68) with simultaneous genotyping of HPV16 and 18 in one tube. The participant collects a dry high vaginal swab, places it in a dry tube, and hands it to the lab for processing. Alternatively, a health care provider collects the cervical swab for the test. Results are displayed as positive or negative for Non 16/18 HR HPV (HPV 13) while HPV 16 and 18 are identified individually and reported as such.
We collected data using a data collection tool designed for the study. The data extracted from client records included socio-demographic and medical characteristics, and HPV DNA test results. No personal information was included in the data collection tool. The data from the collection tool were entered into an Epi-info database and analyzed using SPSS version 20.0 for Windows. We used descriptive statistics to describe the data. We also carried out bivariate analysis of variables such as age at first coitus, marital status, parity, years of education and HIV status for association with HPV prevalence. We used the Chi square test to determine the statistical significance of differences in prevalence. P values <0.05 were considered significant at 95% confidence interval.
Results
Out of 760 women screened during the period of study, 08 had inadequate results. Accordingly, 752 files were retained for the study.
Socio-Demographic Profile of Participants
The mean age was 41 ± 10.14 years. The major part (60%) of women had eight or more years of education and 40 % had more than 12 years of education.
Obstetric and Medical Parameters
The majority of women (62%) had more than two children and 133 (17%) were HIV positive.
High-Risk HPV: Test Sampling and Prevalence
Out of 752 cases with adequate results, 315 (41.89%) were positive for (at least one) HR HPV DNA, while 437 were negative. In 630 cases (83%) the sample was self-collected while in the remaining 122 cases (17%) a health provider collected the sample for HR HPV DNA testing.
Factors Associated with High-Risk Hpv Infection
The mean age at sexarche among women infected with HR HPV was 18.09 ± 2.9 years and 18.39 ± 3.6 among HR HPV-negative women. Being HIV positive was associated with a greater risk of having HR HPV infection (RR: 3.78, 95% CI: 2.53-5.65; P value = 0.0001).
Prevalence of HR HPV Types
The non 16/18 HPV were the most common type, present in 282 women (81.0%). HPV 16 and 18 were detected in 32 (9.2%) and 34 (9.8%) women, respectively.
Discussion
This study assessed the prevalence of high-risk human papilloma virus (HR HPV) infection among women aged 30 and above coming for cervical cancer screening at two hospitals in Yaoundé, Cameroon, for the period spanning from February 2020 to December 2021. The research also sought to determine the factors associated with HR HPV positivity.
Socio-Demographic and Medical Data
The age grouping of the study sample population shows a progressive drop in participant numbers and proportions as age increases. This reflects the youthful nature of the Cameroonian population [15,16]. There is also a high proportion of educated women above primary level, the majority of women are married, and more than 80% of women had their first coitus by age 20, characteristics that mirror the general situation in the country [16]. These elements suggest that our study sample could be acceptably representative of the general population with respect to these parameters. The 17.69 % proportion of positivity of the women for HIV, however, sharply contrasts with the 9.7% expected for women in Yaoundé [16]. This suggests a selection bias in favor of a high level of sensitization among HIV positive women towards screening for cervical cancer.
HPV Prevalence
The prevalence of HR HPV infection in our study was 41.8%. We did not find any official data on the national prevalence of high-risk HPV. However, our finding goes in line with reports from other studies on HR HPV prevalence in Yaoundé. Simo et al, in 2021, reported a prevalence of HR HPV of 38.7% at Saint Martin de Porres health center in Yaoundé [17]. Whereas, a much older report by Njouom, on women screened at the Centre Pasteur laboratory in Yaoundé between 2011 and 2013, revealed a prevalence of HR HPV infection of 30.1% [18]. Doh et al in their systematic review on HPV in Cameroon in 2017 found a prevalence of 36.3% [14]. Some authors, however, report a prevalence of HR HPV markedly lower than we found. Tebeu et al. reported a prevalence of HR HPV of 27% in Tiko and Yaoundé [19]. Cholli et al, in their study in Mutengene and Douala, found a prevalence of HR HPV of 24.2% [20]. Levy et al reported a prevalence of HR HPV of 19.8 % in 2020 in Dschang [21]. The relatively low prevalence reported by these studies can be explained, at least in part, by the nature of the HPV tests used and the semi-urban nature of parts of the study settings. Our study used the Ampfire HPV test that detects 15 types of HR HPV. Levy et al used the Xpert HPV assay, Cholli used the CareHPV test, and Tebeu et al used the Abott Realtime HR HPV assay; all of which detect only 14 types of HR HPV. It is possible that the higher number of HR HPV types detected contributed to drive the prevalence up, in our study, in addition to a possible increase in HPV prevalence over time and in relation to the strictly urban population of our study.
In other African countries, several studies have explored the prevalence of HR HPV. In Ghana, Donkoh et al found the prevalence of oncogenic HPV to be 37.2% [22]. Mutombo et al found the prevalence of HR HPV infection to be 24.8% in the Democratic Republic of Congo. In South Africa, Tiiti et al found the prevalence of HR HPV to be 48.1% [23]. Overall, the studies portray sub-Saharan Africa as the region with the highest prevalence of HR HPV infections in the world [23]. This may be related to the higher burden of HIV and other sexually transmitted infections in this region, as it is known that HIV infection is a risk factor for HPV infection and its persistence [24]. The low level of coverage of HPV vaccine is probably also a contributing factor.
HPV Sample Collection
One of the reasons why cervical cancer screening by HR HPV test has been appealing to women is the possibility for the latter to collect the genital swabs themselves, thereby, avoiding a vaginal procedure uncomfortable to some of them [25,26]. Some clinicians have been concerned that self-collected genital samples for HPV may have lower sensitivity than provider-collected samples. In 2014, Untiet et al showed in their study at the University hospital center of Yaoundé that there was no statistically significant difference in terms of HPV prevalence between self-collected and provider-collected samples [25]. In our study, the majority (83%) of women screened self-collected their samples and these had slightly more positive cases to the HR HPV test than provider-collected samples (42.54% vs 38.5%). However, the difference was not statistically significant. In Taiwan, Nutthachote et al had similar findings; a slightly higher detection rate of HR-HPV DNA for self-collected samples compared to the clinician-collected samples that was not statistically significant [26]. However, during a health campaign in Cameroun in 2013, Berner et al found that although most of the women were more comfortable and less embarrassed with the self-collected HPV sampling, they did not trust the method and did prefer provider sampling [27].
Distribution of HPV Types
The HPV test used in our study is the Ampfire HPV test, a PCR isothermal HPV DNA-based test. It detects 15 HR HPV types (16, 18, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, and 68) and gives partial genotyping of HPV 16 and 18. We found that the most prevalent HPV type was the non-16/18 HR HPV group (80%), followed by HPV 18 (5%) and HPV 16 (4%). Coinfection with HPV 16 and HPV 18 was seen in only two participants. There were varying coinfections of non-16/18 HPV (HR HPV 13) with HPV 16 or 18. Several Cameroonian authors have reported that non-16/18 HPV types are the most prevalent HPV types in Cameroon. Sosso et al found in 2020 that HPV 16 and HPV 18 represented 3% and 4% of cases, respectively [28]. Tebeu et al as well as Njouom also reported that non-16/18 are the most prevalent HPV types in Yaoundé [18, 19]. Njouom further specifies that HPV 16 and HPV 18 represented 1.3% and 3.3% of cases, respectively [18]. Doh et al in their 2017 systematic review found that HPV 16 and 18 represented 6.25% and 3.28% of HR HPV infections among women screened in Cameroon.
A few authors, however, report findings that show a different trend as concerns HPV type distribution. In their study in Yaoundé, Simo et al reported a prevalence of HPV 16 at 28.46%, HPV 18 at 17.5%, and coinfection with 16 and 18 at 16.78% [17]. However, the type of test they used for their study could explain these results: a HPV DNA test that could only detect HPV 16, 18, 33 and 45. Global data also shows that HPV 16 represents the most prevalent HPV type. However, when this data is segregated per region it is observed that Western Africa has the lowest HPV 16 prevalence (11.1%) compared to 24.4% in Western Europe and 32.3% in Southern Asia [25].
Factors Influencing HPV Infection
HIV infection was strongly associated with an increased prevalence of HR HPV infection. We found that 68% of HIV-positive participants had a HR HPV infection compared to 36% for their HIV-negative counterparts and this difference was statistically significant. Sosso et al had a similar finding in their study in Yaoundé in 2012, with a prevalence of HR HPV of 43.47% in HIV positive women against 28.42% in the HIV-negative [29]. Adedimeji et al also reported a similar difference: 46% in HIV-positive women against 21% for HIV-negative women [30]. This goes in line with the belief that immunosuppression, as seen in HIV infection, plays an important role in the natural history of HPV infection, from acquisition through persistence, and progression to precancerous lesions [24]. First sexual intercourse before 18 years, having three or more term births, having a secondary or higher level of education, and being married were not shown to have a significant association with HR HPV infection. However, according to some studies, and the American Cancer Society, early debut of sexual activity (especially before age 18) is a risk factor for HPV infection [31, 32]. Simo et al in Yaoundé in 2021 found that 40% of HPV positive women in their study had their first sexual intercourse before 16 years of age [17]. We did not use this cut-off for comparison; hence, it is difficult to confront these findings. Akabourne et al. found a parity greater than 5 to be associated with a higher prevalence of HR HPV infection [33]. This cut-off is however different from that of parity above 03 that we used in our study and found no association, with a bigger sample size.
The Limits of the study
Even though this study had a good sample size, it was health facility based and the findings may not be a replica of the situation in the community due to selection bias. The retrospective nature of the study made it difficult to obtain complete records, especially for some variables like age at sexarche. This may have affected analysis, especially as regards evaluation for risk factors of HPV infection. In addition, we could not study some variables of interest, like cumulated number of sexual partners and HPV vaccination status; even though for the latter, very few or no women of that age bracket are expected to have taken the vaccine. Furthermore, the HPV test used here presents the results of the 13 non-16/18 serotypes as a bundle, such that the details of their prevalence cannot be obtained for a fine confrontation with the antigens of the nonavalent HPV vaccine available in the market.
Conclusion
This study reveals a higher prevalence of high-risk HPV (41.8%) than previously reported in most studies of women screened for the infection in the country, suggesting an increase in prevalence over time. The prevalence of non-16/18 serotypes is disproportionately higher (81.0%) than that of types 16 (9.2%) and 18 (9.8%) covered by the vaccine distributed in the country.
The great majority of women opted for self-sample collection for the HPV DNA test and this method had same test efficacy as with provider-collected sampling. Meanwhile, the lone factor significantly associated with HPV infection in this study was the existence of infection with HIV.
Recomendations
Based on the findings and conclusions of this study, we suggest to government and research bodies to do nationwide studies of prevalence of HPV serotypes, preferably detailing the non-16/18 types, and their real involvement in cervical cancer occurrence to ascertain the need to resort to an HPV vaccine that integrates more non-16/18 serotypes
The use of HR HPV tests, as the primary screening method for cervical cancer, especially in HIV positive women, should be promoted. Clinicians should emphasize the efficacy of both self- and provider-collected samples during counseling for the HPV DNA test, and make provisions to accommodate the few who prefer provider-collected sampling, so as to give the women greater informed autonomy in the choice of a sampling method.
- Globocan (2020) Available at: https://gco.iarc.fr/today/data/factsheets/cancers/23-ervix-uteri-fact-sheet.pdf
- Global strategy to accelerate the elimination of cervical cancer as a public health problem. WHO.
- International Agency for Research on Cancer (2020) Cancer Today [Internet]. WHO.
- Tebeu PM, Petignat P, Mhawech Fauceglia P (2009) Gynecological malignancies in Maroua, Cameroon. Int J Gynaecol Obstet 104: 1489.
- Sando Z, Fouogue JT, Fouelifack FY, Fouedjio JH, Mboudou ET, Essame JLO. [Profile of breast and gynecological cancers in Yaoundé-Cameroon]. Pan Afr Med J 17: 28.
- American cancer society (2022) Available at: https://www.cancer.org/cancer/cervical cancer/about/ key-statistics.html
- CDC (2022) Available at: https://www.cdc.gov /cancer/cervical/statistics/index.htm
- Lei et al. (2020) HPV Vaccination and the Risk of Invasive Cervical Cancer. N Engl J Med 383: 1340-8.
- New recommendations for screening and treatment to prevent cervical cancer, 6 July 2021.
- WHO (2015) Human papillomavirus (HPV) and cervical cancer.
- Lorraine Elit, Calvin Ngalla, Glen Mbah Afugchwi, Eric Tum, Joël Fokom-Domgue, Elysée Nouvet (2022) Study protocol for assessing knowledge, attitudes and belief towards HPV vaccination of parents with children aged 9–14 years in rural communities of North West Cameroon: a qualitative study. BMJ Open 12: e062556.
- Human Papillomavirus and Related Diseases Report. ICO/IARC Information Centre on HPV and Cancer (HPV Information Centre) 2022.
- Tebeu PM, Ako A, Nguefack TC, Tseunwo TC, Kengne FG, Sando Z (2018) Épidémiologie de l’Infection à HPV en Région Semi-Urbaine du Cameroun: l’Expérience du District de Santé de Baham (Ouest-Cameroun). Health Sci. Dis 19
- G Doh, GM Ikomey, D Njenda, J Gichana, MG Katusiime et al. (2017) Oncogenic Human Papillomavirus Genotypes 16 and 18 Prevalence Among Women with Normal Cervical Cytology and Neoplasia in Cameroon: A Systematic Review. Health Sci. Dis 18.
- Aaron O'Neill (2022) Age structure in Cameroon 2021.
- SC Billong, J Fokam, JD Anoubissi, CK Nde, RT Fodjo et al. (2020) The declining trend of HIV-Infection among pregnant women in Cameroon infers an epidemic decline in the general population. Heliyon 6: e04118.
- Tagne Simo R, Djoko Nono AG, Fogang Dongmo HP, Seke Etet PF, Fonyuy BK et al. (2021) Prevalence of precancerous cervical lesions and high-risk human papillomavirus types in Yaounde, Cameroon. The Journal of Infection in Developing Countries 15: 1339-45.
- Njouom R (2013) Prévalence des génotypes du HPV à HR oncogènes dans les échantillons cervicaux analysés au Centre Pasteur du Cameroun. Workshop on HPV/Cervical cancer network in Francophone Africa, Durban, South Africa.
- Tebeu PM, Fokom-Domgue J, Crofts V, Flahaut E, Catarino R, Untiet S et al. (2014) Effectiveness of a two-stage strategy with HPV testing followed by visual inspection with acetic acid for cervical cancer screening in a low-income setting. International Journal of Cancer 136: E743-50.
- Cholli P, Bradford L, Manga S, Nulah K, Kiyang E, Manjuh F et al. (2018) Screening for cervical cancer among HIV-positive and HIV-negative women in Cameroon using simultaneous co-testing with careHPV DNA testing and visual inspection enhanced by digital cervicography: Findings of initial screening and one-year follow-up. Gynecologic Oncology 148: 118-25.
- Levy J, Preux M, Kenfack B, Sormani J, Catarino R, Tincho EF et al. (2020) Implementing the 3T‐approach for cervical cancer screening in Cameroon: Preliminary results on program performance. Cancer Medicine.
- Donkoh ET, Asmah RH, Agyemang-Yeboah F, Dabo EO, Wiredu EK (2022) Prevalence and Distribution of Vaccine-Preventable Genital Human Papillomavirus(HPV) Genotypes in Ghanaian Women Presenting for Screening. Cancer Control 107327482210947.
- Tiiti TA, Selabe SG, Bogers J, Lebelo RL (2022) High prevalence of and factors associated with human papillomavirus infection among women attending a tertiary hospital in Gauteng Province, South Africa. BMC Cancer 22.
- Bruni L, Diaz M, Castellsagué X, Ferrer E, Bosch F Xavier, de Sanjosé S (2010) Cervical Human Papillomavirus Prevalence in 5 Continents: Meta‐Analysis of 1 Million Women with Normal Cytological Findings. The Journal of Infectious Diseases 202: 1789-99.
- Liu G, Sharma M, Tan N, Barnabas RV (2018) HIV-positive women have higher risk of human papilloma virus infection, precancerous lesions, and cervical cancer. AIDS 32: 795-808.
- Untiet S, Vassilakos P, McCarey C, Tebeu P-M, Kengne-Fosso G, Menoud P-A, et al. (2014) HPV self-sampling as primary screening test in sub-Saharan Africa: Implication for a triaging strategy. International Journal of Cancer 135: 1911-7.
- Nutthachote P, Oranratanaphan S, Termrungruanglert W, Triratanachat S, Chaiwongkot A, Baedyananda F et al. (2019) Comparison of detection rate of high risk HPV infection between self-collected HPV testing and clinician-collected HPV testing in cervical cancer screening. Taiwanese journal of obstetrics & gynecology 58: 477-81.
- Berner A, Hassel SB, Tebeu P-M, Untiet S, Kengne-Fosso G, Navarria I et al. (2013) Human Papillomavirus Self-Sampling in Cameroon: Women’s Uncertainties Over the Reliability of the Method Are Barriers to Acceptance. Journal of Lower Genital Tract Disease 17: 235-41.
- Sosso SM, Tchouaket MCT, Fokam J, Simo RK, Torimiro J, Tiga A et al. (2020) Human immunodeficiency virus is a driven factor of human papilloma virus among women: evidence from a cross-sectional analysis in Yaoundé, Cameroon. Virology Journal 17.
- Adedimeji A, Ajeh R, Dzudie A, Kendowo E, Fuhngwa N, Nsame D et al. (2020) Cervical human papillomavirus DNA detection in women living with HIV and HIV-uninfected women living in Limbe, Cameroon. Journal of Clinical Virology 128: 104445.
- Nejo YT, Olaleye DO, Odaibo GN (2018) Prevalence and Risk Factors for Genital Human Papillomavirus Infections Among Women in Southwest Nigeria. Archives of basic and applied medicine 6: 105-12.
- American Cancer Society (2017) Risk Factors for Cervical Cancer [Internet]. Cancer.org. American Cancer Society.
- Akaaboune M, Kenfack B, Viviano M, Temogne L, Catarino R, Tincho E et al. (2018) Clearance and persistence of the human papillomavirus infection among Cameroonian women. Women’s Health 14: 174550651880564.
FIGURE 1
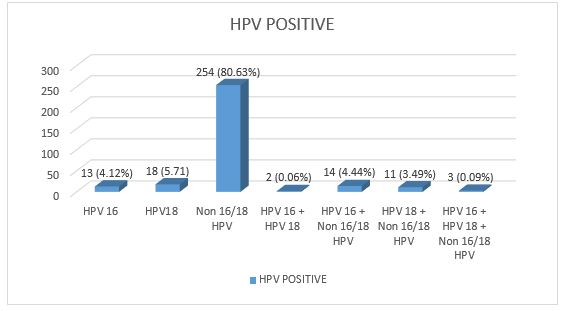
Figure 1: Distribution of HR HPV types among infected women (single serotype and coinfections)
Tables at a glance
Figures at a glance