Effects of Pleasant Stimulation with Sea Video Viewing on Heart Rate Variability and Frontal Lobe Brain Activity in Early Pregnancy: A Pilot Study Assessing Perinatal Depression Risk
Received Date: January 07, 2024 Accepted Date: February 07, 2024 Published Date: February 10, 2024
doi: 10.17303/jwhg.2024.11.102
Citation: Hiromi Suenaga, Masae Tsutsumi, Misae Ito, Miyako Saito, Keiko Kamitani et al. (2024) Effects of Pleasant Stimulation with Sea Video Viewing on Heart Rate Variability and Frontal Lobe Brain Activity in Early Pregnancy: A Pilot Study As sessing Perinatal Depression Risk. J Womens Health Gyn 11: 1-11
Abstract
Objective:This study aims to examine whether viewing sea images affects heart rate variability (HRV) and brain activity during early pregnancy
Methods:This observational study evaluated changes in HRV indices and brain activity of pregnant women during the first trimester, both before and after viewing 5-minute sea videos. The inclusion criteria consisted of singleton pregnancies at 14–23 weeks of gestation, with no history of cardiac disease. The study included 32 pregnant women. The electrocardiogram (ECG) and brain activity were assessed from before the video viewing to the end of the session, which also involved completing the Edinburgh Postnatal Depression Scale (EPDS). HRV from the ECG was used to assess autonomic activity. Based on their EPDS scores, the women were divided into low- and high-EPDS groups.
Results:Comparing the HRV of the low- and high-EPDS groups, no significant difference was observed before and after viewing the video. However, there was a significant increase in the high frequency powers of HRV expressed in normal units (HFnu) (p< 0.05, p < 0.01) and a decreasing trend in HRV (LF/ HF) after viewing the sea video regardless of the EPDS group. In the high-EPDS group, sea video viewing led to decreased activity in the left frontal lobe and increased activity in the right frontal lobe. In the low-EPDS group, both left and right frontal lobe activity showed a tendency to increase after viewing the sea video.
Conclusions:Sea videos, known for their relaxing effect, may induce negative emotional responses in individuals with a higher risk of depression. Assessing brain activity rather than autonomic function may prove more effective in predicting the onset of perinatal depression.
Keywords:Perinatal Depression; Heart Rate Variability; Brain Activity; Japanese Version of the Edinburgh Perinatal Depression Questionnaire; Near Infrared Spectroscopy
Introduction
Depression is considered the most common perinatal complication, with 15% of pregnant women experiencing depression and anxiety [1-4]. Various epidemiological and case-control studies have shown that perinatal depression could also lead to delayed physical, psychological, and social development in the child [5-9]. Severe cases could result in maternal suicide. Depression, anxiety, and stress during pregnancy are often undetectable and remain untreated by health professionals. In an effort to improve maternal well-being globally, the World Health Organization recently stepped up preventive efforts to reduce maternal morbidity and mortality [10]. In January 2016, the U.S. Preventive Services Task Force recommended screening for maternal depression [11]. The 2017 Japanese Society of Obstetrics and Gynecology guidelines recommend the Edinburgh Postnatal Depression Scale (EPDS) evaluation during antenatal checkups.
Early diagnosis and intervention for perinatal depression are important social issues; however, the sensitivity and specificity of EPDS for perinatal depression are low, and a definitive mass screening system to predict depression has not been established.
In general depression, heart rate variability (HRV) measurements, the most commonly used test to assess autonomic function, are frequently reported, and meta-analyses suggest that HRV is characterized by dysregulation of autonomic nervous system (ANS) activity [12,13]. Dysregulation of cardiac vagal control, as indexed by relatively low high-frequency HRV (HF-HRV), has been implicated in depressed mood and hypertensive disorders in non-pregnant adults [14]; however, studies during pregnancy are limited.
Rouleau et al. reported a trend toward lower HRV in cases of perinatal depression and general depression [15]. However, Rådmark et al. reported no predominant difference in HRV between non-depressed pregnant women and pregnant women with perinatal depression [16]. Nevertheless, their findings have not consistently aligned with other studies in this area. This can be attributed to the fact that blood circulation increases significantly during pregnancy, and to bring about this change, sympathetic activity is also markedly increased in normal pregnancy [17-19], resulting in a significant change in ANS compared to pre-pregnancy.
Screening for depression by measuring HRV could be challenging because this change already occurs at 8 weeks of gestation [20], and there are large inter-individual differences in autonomic activity. However, it is already known that high autonomic activity, particularly vagal activity, is associated with high resistance and adaptability to environmental stress [21].
In recent years, there has been a significant interest in depression in the field of neuroscience, and there have been many reports on this topic. Several studies have reported that left–right differences in the emotionally-reactive frontal lobes are more common in patients with depression, with several studies showing reduced activity in the left frontal lobe, which is responsible for positive emotional responses [22-25].
Near-infrared spectroscopy (NIRS) is gaining attention as a non-invasive method for evaluating brain activity. NIRS measures changes in weak oxyhemoglobin (oxy-Hb) and deoxyhemoglobin (deoxy-Hb) concentrations in cerebral blood vessels by placing sensors with a 3 cm sensibility on the head, making it possible for visualization [26,27]. Studies using NIRS to assess anxiety states have shown that subjects with right-dominant resting oxy-Hb changes in the frontal lobe have higher anxiety levels and those with left-dominant resting oxy-Hb changes have lower anxiety levels [28]. However, to the best of our knowledge, no reports have evaluated brain activity in pregnant and parturient women.
Many studies have reported that the natural environment has a positive effect on ANS, and we have also reported the effects of walking in the ocean, flowers, artificial gardens, and forests on ANS balance [29]. We also demonstrated that parasympathetic nervous activity is activated by moving images such as the sea [30]. Stress from various environments is widely known to be a risk factor for perinatal depression. Previous studies have shown that sea images can reduce stress by introducing a relaxing effect, suggesting that they may also have a positive effect on emotional activity [31]. However, to date, no study has examined the effects of these natural environments and images on the ANS activity of pregnant women. Our hypotheses for the present study are as follows: 1) depression and anxiety in pregnant women are associated with left–right differences in brain activity and lower activity in the left frontal lobe and 2) assessment of changes in ANS activity by viewing sea images is associated with perinatal depression. We evaluated the effects of viewing pleasant sea images on relaxation from the perspectives of both the brain and autonomic activity.
In this study, we evaluated the effects of pleasant stimuli using sea images on HRV and brain activity in the frontal lobes of pregnant women in the first trimester of pregnancy, which is an important period for fetal development, especially for the differentiation of the central nervous system. Simultaneously, we conducted the EPDS test to evaluate the relationship with EPDS.
Materials and Methods
The participants were pregnant women undergoing antenatal care at the outpatient obstetrics clinic of Yamaguchi University Hospital. Those who were (1) aged 18 or older, (2) in an early pregnancy of less than 24 weeks, and (3) with no history of cardiovascular disease were enrolled in the study after obtaining written informed consent. Based on the demographic results, participants did not include pregnant women with a history of anxiety disorders.
This study was initiated after receiving approval from the Ethics Review Committee of Yamaguchi University Hospital in 2022 and was conducted in accordance with the Helsinki Declaration, as revised in 1989. All the collected data were anonymous and confidential.
Procedure
Participants were asked to wear electrocardiogram (ECG) electrodes on their chest and optical topography test sensors on their foreheads to measure brain activity in the examination room after the completion of the antenatal checkup. In a sitting position, the participants entered the following information on a PC: date of birth, expected date of delivery, history of delivery, miscarriage, occupation, and family structure. Conditions such as the distance between the sea image and participant, viewing time, and volume were determined with reference to previous studies [30]. The participants then watched a 5-minute sea video and were prompted to respond to the EPDS on a PC. During this period, ECG and brain activity were continuously recorded.
The ECG was recorded from the beginning until the end of the examination. The laboratory temperature was set at 25° C for a quiet environment. Spectral analysis [32] was performed on the obtained R-R intervals using MemCalc software (GMS). The frequency components in the three domains were quantified to determine the HRV parameters: low frequency (LF) (ms2) power (0.04–0.15 Hz, indicating sympathetic and parasympathetic activity); high frequency (HF) (ms2) power (0.15–0.40 Hz, reflecting the parasympathetic nervous system); LF/HF ratio (indicating the balance between sympathetic and parasympathetic activity); and time HRV index in the domain (RR interval coefficient of variation [CVRR]) [33]. HFnu (= HF/(LF+HF) ×100, nu: normalized unit) was also calculated to reflect the balance between sympathetic and parasympathetic activities. Regarding the HRV index, the average of the first few minutes after the ECG was attached was used as the baseline, and the average of the 5 minutes during sea video viewing was used as the effect of pleasant stimuli index.
Brain Activity
HOT-2000, a two-channel wearable portable brain activity measurement device that monitors blood flow changes in the frontal lobe using near-infrared light was used [34]. A laser beam of 810 nm wavelength was used, with a sampling rate of 10 Hz. This made it possible to measure brain activity by penetrating the scalp of the cerebral cortex up to approximately 2 cm and detecting total blood flow. Total hemoglobin (sum of oxy-Hb and deoxy-Hb; t-Hb), which is the raw data of signals obtained from the HOT-2000 at two locations on either side of the frontal lobe, was analyzed as the cerebral blood volume.
The device was worn such that sweat and dirt on the forehead were wiped away with an alcohol-impregnated cotton ball, and the headset was placed close to the forehead and above the eyebrows.
EPDS
EPDS, the most commonly-used screening instrument for perinatal depression, is a 10-item self-rating scale in which depressive symptoms over the past 7 days are scored on a 4-point Likert scale (0 to 3), with total scores ranging from 0 to 30 [35,36]. Of the EPDS items, two assessed loss of interest, and three assessed anxiety and depression. The Japanese version of the EPDS is considered to indicate a high propensity for depression, with a total score of 13 or higher during pregnancy and 9 or higher after delivery [2,37-38].
Statistical Analysis
The cutoff value for pregnancy in the Japanese version of the EPDS is 13 or higher, but considering the small participants pool and the fact that the positive predictive value of the Japanese version of the EPDS is approximately 50% when the cutoff value is set at 13 or higher [37], a cutoff value of 9 or higher was used in this study. Demographic factors were compared between pregnant women at high risk of depression (EPDS greater than 9) and those at low risk (EPDS less than 9) using the Student t-test, Wilcoxon nonparametric test, or Fisher’s exact test. HRV and brain activity measures were expressed as mean ± standard deviations. Regarding population demographic factors, the Student t-test was employed to compare pregnant women at high risk of depression (EPDS greater than 9) and those at low risk (EPDS less than 9). Wilcoxon’s signed rank test was conducted to analyze HRV and brain activity measurements before and after viewing the sea video. The Mann-Whitney U test was used to compare the two groups before and after viewing the video. Cohen's d was used to compare effect sizes of differences before and after video viewing. The statistical significance level was set at 5%. The results are presented as mean ± standard deviation. JMP Pro version 16 (SAS Institute Inc., Cary, NC, USA) was used for performing primary analysis. Statistical significance was set at p≤0.05.
Results
The participants’ characteristics are presented in Table 1. The average age of the participants was 33 years. They included 13 women who had already given birth once, 19 were first-time mothers (first-time birth rate: 59.4%), and 24 were employed (75% employment rate). Of the 32 participants, 26 (81.3%) had an EPDS lower than 9, placing them in the low-EPDS group, and 6 (18.8%) had an EPDS of 9 or greater, resulting in classification as high EPDS, and were assessed as being at high risk for depression (Table 1). There were no significant differences in age, height, weight, or BMI between the high- and low-depression groups. Similarly, although not significant, most of the high-EPDS group participants were housewives and postpartum mothers.
Effects of Sea Video Viewing on HRV Index
The results of the HRV index from the baseline and sea video viewing are shown in Table 2. There were no significant differences in HRV indices at baseline between the high- and low-depression groups. The standardized HFnu significantly increased in both the high- and lowEPDS groups (p< 0.05, p< 0.01) after viewing the sea video, compared to baseline. Both the high and low EPDS groups showed a moderate effect size (d = 0.67 and d = 0.64, respectively). However, the high-EPDS group showed a slightly higher increase (Figure 1). The LF/HF ratio also tended to decrease after viewing the sea video for both the high- and low-EPDS groups (Figure 1).
Effects of Sea Video Viewing on Brain Activity
Table 3 compares the brain activity indices between baseline and sea video viewing in the high- and lowdepression groups. There was no significant difference in baseline brain activity between the high- and low-EPDS groups. However, brain activity in the left frontal lobe after viewing the sea video was significantly lower in the high EPDS group (p< 0.05). A significant negative correlation was also found between brain activity in the left frontal lobe and EPDS score (p< 0.05) (Figure 2).
Comparing the changes in brain activity before and after viewing the sea video, the high-EPDS group showed a decreasing trend in left frontal lobe activity, while the low-EPDS group showed a significant increase (p < 0.01) (Figure 3). In addition, the low-EPDS group had significantly elevated brain activity in the right frontal lobe (p< 0.05), with a trend of increase also observed in the high- -EPDS group, although at a lower level than in the low EPDS group (Figure 3). The effect size of change in brain activity before and after video viewing was small for both the left and right frontal lobes in the low-EPDS group, but larger on the left side (d = 0.29 and d = 0.13, respectively).
There was a shift toward right frontal dominance in the high-EPDS group and toward left frontal dominance in the low-EPDS group after viewing the sea video (Figure 3). These results suggest that left frontal lobe activity tends to decrease in the high EPDS group with sea video viewing.
Discussion
The results of this study showed no significant differences in HRV indices between high- and low-risk depression among primiparas and multiparas. Sea video viewing increased HF, indicating parasympathetic activity, and decreased LF/HF in both participants at low risk for depression and those at high risk, suggesting a relaxing effect on pregnant women. Activity in the left frontal lobe, which controls positive affect, was significantly lower in participants at high risk for depression than in those at low risk for depression, as was activity in the right frontal lobe, which controls negative affect. These findings suggest that participants at high risk for depression may have decreased activity throughout the frontal lobe and poor emotional expression. Additionally, the EPDS score, indicating risk for depression, was negatively correlated with activity in the left frontal lobe, possibly due to weaker expression of positive emotions. Furthermore, participants at higher risk for depression tended to show decreased activity in the left temporal lobe, indicating positive affect, and relatively increased activity in the right frontal lobe, indicating negative affect, after viewing the sea video. Meanwhile, participants at low risk for depression tended to show increased activity in the left frontal lobe and relative left frontal dominance after viewing the sea video. Thus, even for participants at high risk for depression, sea video viewing may have caused unpleasant feelings, despite the relaxing effect on the ANS.
Although there have been many reports showing reduced HRV, especially HF, in depression, there are few reports on HRV in pregnant women, and the results are inconclusive.
In addition, ANS activity after pregnancy increases sympathetic activity in response to increased circulating blood volume, making it difficult to evaluate general depression using HRV. In this study, autonomic function assessment showed that HF was preserved even when the risk of depression was high, and tended to be lower compared to participants at lower risk in terms of LF/HF.
Many neurological studies on general depression have reported decreased left frontal lobe potentials and left- -right differences in frontal lobe potentials on EEG. The left frontal lobe is responsible for positive emotions and the right frontal lobe for negative emotions; the left frontal lobe is less active in depression. Although this study used brain activity rather than EEG, the results align with those of general depression.
Past studies have shown that natural environments and visual images, such as the sea, have relaxing effects [29,30,39–42]. The results of this study demonstrated that sea video viewing had a relaxing effect on ANS activity, even when the risk of depression was high, but it inhibited positive emotions based on brain activity levels.
Early diagnosis and intervention for pregnant women at high risk of mood depression may be necessary to prevent perinatal depression. However, viewing relaxing images may not be effective.
The results of this study suggest that ANS activity at rest alone is not associated with EPDS, but brain activity levels could be used to evaluate the response to stimuli like natural sea images, which are believed to have a relaxing effect, by examining these conditions.
Limitations
The limitations of this study include the small number of participants, as it was a pilot study aimed at early diagnosis and intervention of perinatal depression. Additionally, the study only used sea images as a comfortable stimulus and had a stimulus duration of 5 minutes.
Another limitation of this study is that the participants were limited to early pregnancy, with only one of the 32 having an EPDS cutoff value of 13 or higher at the time of pregnancy. Given that ANS activity during pregnancy differs significantly from that during non-pregnancy, it is challenging to use evidence from general depression as a reference. Thus, further data accumulation is necessary in the future.
Conclusions
There was no difference in the HRV index between pregnant women at high risk for depression and healthy pregnant women. While sea video viewing has been proven to have a relaxing effect on many pregnant women, it stimulated negative emotions in those at high risk for depression. Assessing changes in emotional responses from the viewing of nature videos, typically regarded for their relaxing effects, may help diagnose perinatal depression.
Acknowledgments
The authors are extremely grateful to the outpatient obstetrics and gynecology staff of Yamaguchi University Hospital for their cooperation in conducting the EPDS testing.
Conflict of Interest
The authors have no conflict of interest in relation to this article to disclose.
Ethical Considerations
This study was initiated after receiving approval from the Ethics Review Committee of Yamaguchi University Hospital in 2022 and was conducted in accordance with the Helsinki Declaration, as revised in 1989. All the collected data were anonymous and confidential. Patients were enrolled in the study after obtaining written informed consent.
Funding
This work received support from JSPS KAKENHI Grant Number JP22K12886 and JP20K10987 in post-authoring English editing.
Authors' Contributions
SH collected and analyzed and interpreted patient data and wrote the manuscript; TM contributed to the proposal of experimental ideas; IM, SM, KK, and MS contributed to patient recruitment; SN and HM contributed to the analysis of laboratory data; TM and HM performed the histological examination of the kidneys and contributed to the writing of the manuscript; TM and HM performed the histological examination of the kidneys and contributed to the writing of the manuscript. All authors read and approved the final manuscript.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
- Gelaye B, Rondon MB, Araya R, Williams MA (2016) Epidemiology of maternal depression, risk factors, and child outcomes in low-income and middle-income countries. Lancet Psychiatry 3: 973-82
- Usuda K, Nishi D, Okazaki E, Makino M, Sano Y (2017) Optimal cut-off score of the Edinburgh Postnatal Depression Scale for major depressive episode during pregnancy in Japan. Psychiatry Clin Neurosci 71: 836-42.
- Shorey S, Chee CYI, Ng ED, Chan YH, Tam WWS, Chong YS (2018) Prevalence and incidence of postpartum depression among healthy mothers: a systematic review and meta-analysis. J Psychiatr Res 104: 235-48.
- Lupattelli A, Twigg MJ, Zagorodnikova K, Moretti ME, Drozd M, Panchaud A, Rieutord A, Juraski RG, Odalovic M, Kennedy D, Rudolf G (2018) Self-reported perinatal depressive symptoms and postnatal symptom severity after treatment with antidepressants in pregnancy: a cross-sectional study across 12 European countries using the Edinburgh Postnatal Depression Scale. Clin Epidemiol 10: 655-69.
- O’Hara MW, McCabe JE (2013) Postpartum depression: current status and future directions. Annu Rev Clin Psychol 9: 379-407.
- Stein A, Pearson RM, Goodman SH, Rapa E, Rahman A, et al. (2014) Effects of perinatal mental disorders on the fetus and child. Lancet 384: 1800-19.
- Closa-Monasterolo R, Gispert-Llaurado M, Canals J, Luque V, Zaragoza-Jordana M, et al. (2017) The effect of postpartum depression and current mental health problems of the mother on child behaviour at eight years. Matern Child Health J 21: 1563-72.
- Farías-Antúnez S, Xavier MO, Santos IS (2018) Effect of maternal postpartum depression on offspring’s growth. J Affect Disord 228: 143-52.
- Banovcinova L, Skodova Z, Jakubcikova K (2019) Predictors of increased depressive symptoms in the postpartum period. Kontakt 21: 32-8.
- The World Health Organization (2014) WHO Recommendations on Postnatal Care of the Mother and Newborn.
- Siu AL, Bibbins-Domingo K, Grossman DC, Baumann LC, Davidson KW, et al. (2016) Screening for depression in adults: US Preventive Services Task Force recommendation statement (USPSTF). JAMA 3154: 380-87.
- Musselman DL, Evans DL, Nemeroff CB (1998) The relationship of depression to cardiovascular disease. Arch Gen Psychiatry 55: 580-92.
- Gorman JM, Sloan RP (2000) Heart rate variability in depressive and anxiety disorders. Am Heart J 140: 77-83.
- Kemp AH, Quintana DS, Gray MA, Felmingham KL, Brown K, Gatt JM (2010) Impact of depression and antidepressant treatment on heart rate variability: a review and meta-analysis. Biol Psychiatry 67: 1067-74.
- Rouleau CR, Tomfohr-Madsen LM, Campbell TS, Letourneau N, O’Beirne M, et al. (2016) The role of maternal cardiac vagal control in the association between depressive symptoms and gestational hypertension. Biol Psychol 117: 32-42.
- Rådmark L, Osika W, Wallén MB, Nissen E, Lönnberg G, Bränström R, et al. (2023) Autonomic function and inflammation in pregnant women participating in a randomized controlled study of Mindfulness Based Childbirth and Parenting. BMC Pregnancy Childbirth 23: 237.
- Ekholm EM, Piha SJ, Antila KJ, Erkkola RU (1993) Cardiovascular autonomic reflexes in mid-pregnancy. Br J Obstet Gynaecol 100: 177-82.
- Klinkenberg AV, Nater UM, Nierop AD, Bratsikas A, Zimmermann R, Ehlert U (2009) Heart rate variability changes in pregnant and non-pregnant women during standardized psychosocial stress. Acta Obstet Gynecol Scand 88: 77-82.
- Ekholm EM, Erkkola RU (1996) Autonomic cardiovascular control in pregnancy. Eur J Obstet Gynecol Reprod Biol 64: 29-36.
- Stein PK, Hagley MT, Cole PL, Domitrovich PP, Kleiger RE, Rottman JN (1999) Changes in 24-hour heart rate variability during normal pregnancy. Am J Obstet Gynecol 180: 978-85.
- Holzman JB, Bridgett DJ (2017) Heart rate variability indices as bio-markers of top-down self-regulatory mechanisms: A meta-analytic review. Neurosci Biobehav Rev 74: 233-55.
- Debener S, Beauducel A, Nessler D, Brocke B, Heilemann H, Kayser J (2000) Is resting anterior EEG alpha asymmetry a trait marker for depression? Findings for healthy adults and clinically depressed patients. Neuropsychobiology 41: 31-7.
- Davidson RJ (1995) Cerebral asymmetry, emotion, and affective style. In: Brain Asymmetry. Davidson RJ and K Hugdahl, eds. MIT, Cambridge, pp 361-87.
- Davidson RJ (1998) Affective style and affective disorders: perspectives from affective neuroscience. Cogn Emot 12: 307-30.
- Coan JA, Allen JJB (2004) Frontal EEG asymmetry as a moderator and mediator of emotion. Biol Psychol 67: 7-49.
- Villringer A, Chance B (1997) Non-invasive optical spectroscopy and imaging of human brain function. Trends Neurosci 20: 435-42.
- Strangman G, Culver JP, Thompson JH, Boas DA (2002) A quantitative comparison of simultaneous BOLD fMRI and NIRS recordings during functional brain activation. NeuroImage 17: 719-31.
- Ishikawa W, Sato M, Fukuda Y, Matsumoto T, Takemura N, Sakatani K (2014) Correlation between asymmetry of spontaneous oscillation of hemodynamic changes in the prefrontal cortex and anxiety levels: a near-infrared spectroscopy study. J Biomed Opt 19: 027005.
- Suenaga H, Murakami K, Murata N, Nishikawa S, Tsutsumi M, Nogaki H (2020) The effects of an artificial garden on heart rate variability among healthy Young Japanese adults. Int J Environ Res Public Health 17: 9465.
- Tsutsumi M, Nogaki H, Shimizu Y, Stone TE, Kobayashi T (2017) Individual reactions to viewing preferred video representations of the natural environment: A comparison of mental and physical reactions. Jpn J Nurs Sci 14: 3-12.
- Alcock I, White MP, Wheeler BW, Fleming L, Depledge MH (2014) Longitudinal effects on mental health of moving to greener and less green urban areas. Environ Sci Technol 48: 1247-55.
- Rottman JN, Steinman RC, Albrecht P, Bigger Jr JT, Rolnitzky LM, Fleiss JL (1990) Efficient estimation of the heart period power spectrum suitable for physiologic or pharmacologic studies. Am J Cardiol 66: 1522-24.
- Malik M, Bigger JT, Camm AJ, Kleiger RE, Malliani A, Moss AJ, Schwartz PJ (1996) Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Eur Heart J 17: 354-81.
- Takahashi S, Sakurai N, Kasai S, Kodama N (2022). Stress evaluation by hemoglobin concentration change using mobile NIRS. Brain Sci 12: 488.
- Cox JL, Holden JM, Sagovsky R (1987) Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br J Psychiatry 150: 782-6.
- Cox JL, Holden JM, Henshaw C (2014) Perinatal Mental Health. The Edinburgh Postnatal Depression Scale (EPDS) Manual. 2nd edn. Cambridge University Press.
- Okano T, Murata M, Masuji F, Tamaki R, Nomura J, Miyaoka H, et al. (1996) Validation and reliability of Japanese version of the EPDS. Arch Psychiatr Diag Clin Evaluat 7; 525-33.
- Sasaki Y, Baba T, Oyama R, Fukumoto K, Haba G, Sasaki M (2019). Re-evaluation of the Edinburgh Postnatal Depression Scale as screening for post-partum depression in Iwate Prefecture, Japan. J Obstet Gynaecol Res 45: 1876-83.
- Horiuchi M, Endo J, Takayama N, Murase K, Nishiyama N, et al. (2014). Impact of Viewing vs. not Viewing a Real Forest on Physiological and Psychological Responses in the Same Setting. Int J Environ Res Public Health 11: 10883-901.
- Triguero-Mas M, Dadvand P, Cirach M, Martínez D, Medina A, et al. (2015) Natural outdoor environments and mental and physical health: Relationships and mechanisms.Environ Int 77: 35-41.
- Ikei H, Komatsu M, Song C, Himoro E, Miyazaki Y (2014) The physiological and psychological relaxing effects of viewing rose flowers in office workers. J Physiol Anthropol 33: 6.
- Vert C, Gascon M, Ranzani O, Márquez S, Triguero-- Mas M, et al. (2020). Physical and mental health effects of repeated short walks in a blue space environment: A randomised crossover study. Environ Res 188: 109812.
FIGURE 1
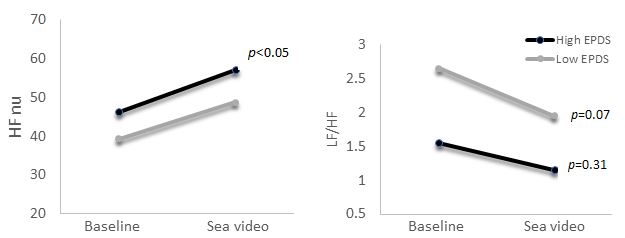
Figure 1: Comparison of heart rate variability (HRV) measures (Left: HFnu, Right: LF/HF) before and after viewing sea video. Gray bars represent the Low EPDS group and black bars represent the High EPDS group
FIGURE 2
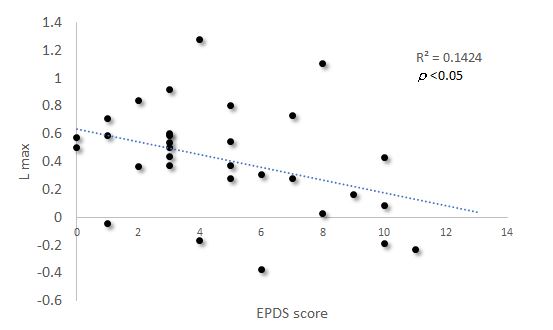
Figure 2: Association between the EPDS score and left frontal lobe brain activity. The amount of brain activity in the left frontal lobe by viewing sea images shows a negative correlation trend with the EPDS score
FIGURE 3
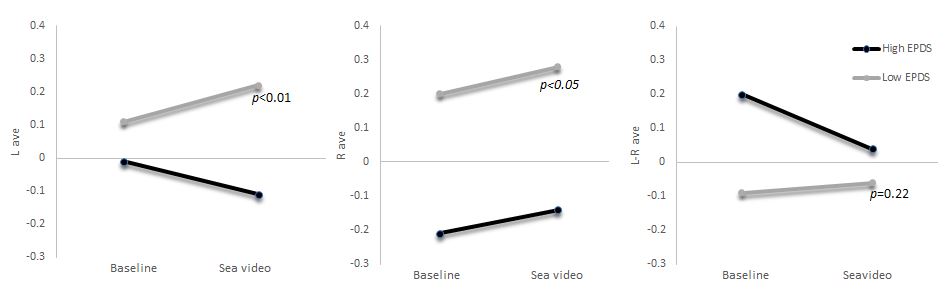
Figure 3: Comparison of brain activity measures before and after viewing the sea video. The graph shows the change in frontal lobe brain activity between baseline and sea video viewing. The left panel shows left frontal lobe brain activity, the center panel shows right frontal lobe brain activity, and the right panel shows the difference between the left and right frontal lobe activities
Tables at a glance
Figures at a glance