An Unusual Presentation of Renal Infarct in the Early Postpartum Period
Received Date: September 07, 2024 Accepted Date: October 07, 2024 Published Date: October 10, 2024
doi: 10.17303/jwhg.2024.11.203
Citation: De Jesus Nunez K (2024) An Unusual Presentation of Renal Infarct in the Early Postpartum Period. J Womens Health Gyn 11: 1-5
Abstract
Postpartum renal infarction is an uncommon but serious complication that can arise after delivery, often associated with significant blood loss or underlying thrombophilia. This report aims to highlight the clinical presentation, diagnosis, and management of renal infarction during the postpartum period.
Keywords: Renal Infarct; Postpartum Period; Migraines; Venous Thrombosis; Uterine; Chorioamnionitis
Case Description
A 23-year-old female with the past medical history of migraines without aura and bipolar disorder presented with uterine contractions at 36 weeks gestation of her first pregnancy. Family history was notable for provoked deep venous thrombosis in her mother. Social history indicated occasional alcohol intake, which the patient ceased during pregnancy, and no tobacco use was reported.
On physical exam, the patient appeared well-developed but in mild distress due to uterine contractions, the abdominal examination revealed a gravid uterus, and a pelvic exam showed cervical dilatation of 4 centimeters. Laboratory tests indicated normochromic normocytic anemia. Chemistry and coagulation profiles were within normal limits.
During hospital admission, delivery was complicated by labor arrest and chorioamnionitis, which was treated with gentamycin and ampicillin. A cesarean section was performed, complicated by an estimated blood loss of 1500 ml necessitating 3 units of packed red blood cells and methylergonovine. Despite adequate analgesia, the patient experienced severe postoperative pain on day 2. Subsequent physical examinations revealed left-sided flank pain and suprapubic tenderness. Repeat laboratory tests showed mild normochromic normocytic anemia and normal renal and coagulation function.
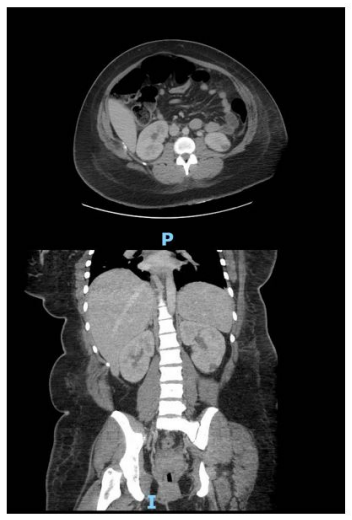
Given disproportionate postoperative pain, a computerized tomography was performed, revealing a wedgeshaped hypodensity in the left kidney consistent with an infarct and a small loculated pelvic collection suggestive of postsurgical changes.
A hypercoagulability workup, including the antiphospholipid panel, coagulation profile, protein C, protein S, Factor V of Leiden mutation analysis, hemoglobin electrophoresis, and homocysteine level was sent and reported as within normal limits. An echocardiogram showed a normal ejection fraction with no vegetation or wall motion abnormalities. The patient was started on breastfeeding-compatible full-dose anticoagulation per hematology recommendations. Nephrology was consulted, and after evaluation, the lesion was determined to be not amenable to embolization. Ultimately, postpartum hemorrhage was identified as the underlying cause.
Discussion
Even though postpartum hemorrhage is a common complication seen in labor and delivery, and after cesarean sections, it can lead to significant sequelae affecting vital organs such as the kidneys.
There are two main etiologies for renal infarction: thromboembolic events originating from the aorta and in situ thrombosis secondary to renal artery dissection or significant blood loss. Associated risk factors for renal infarction in the postpartum period include extremes of age, pre-existing cardiovascular disease, thrombophilia, infectious etiologies such as COVID-19 infection and chorioamnionitis, a family and personal history of hypercoagulable disorders, multiple gestations, tobacco and cocaine use, postpartum hemorrhage requiring transfusions and prothrombotic medications, and delivery by cesarean section compared with vaginal delivery. Additionally, compromised renal artery blood flow during trauma or dissection has also been described. While migraines with aura have been associated with an increased risk of stroke, it is unknown whether this represents a systemic risk for thrombosis.
In the postpartum period, renal circulation can be compromised, particularly when excessive blood loss surpasses the increase in thrombin production and decrease in fibrinolysis that have been observed since the early stages of pregnancy. In this case, this is the most likely explanation, given the absence of evidence for a personal or family history of hypercoagulable disorders, no thromboembolic source, and significant blood loss during the cesarean section that required a blood transfusion, along with chorioamnionitis treated with antibiotics. Although the patient's family history included deep venous thrombosis in her mother, that event occurred after a surgical intervention and is thus considered a provoked thrombosis due to a temporary hypercoagulable state following a prolonged immobilization period; no workup was done at that time. The patient’s hypercoagulable workup was found to be within normal limits, and no atrial fibrillation or arrhythmias were identified.
When evaluating thrombotic phenomena in the postpartum period, it is crucial to recognize that pregnancy itself induces a hypercoagulable state to protect against massive blood loss during delivery. However, under normal circumstances, there is a balance between hypercoagulable and fibrinolytic factors, with no evidence of systemic thrombosis. An increase in thrombin levels can be detected as early as the fifth week of gestation.
Renal infarcts are often undiagnosed due to their similar clinical presentation to pyelonephritis and nephrolithiasis. In addition to the typical clinical presentation characterized by flank pain, it is important to consider the likelihood of embolic and thrombotic phenomena. Factors that may suggest a renal infarct include atrial fibrillation, postsurgical bleeding, acute kidney injury associated with microscopic hematuria, and elevated LDH levels.
Diagnosis is supported by findings of renal infarction on computed tomography, which is generally described as a wedge-shaped hypodensity; MRI with gadolinium is an alternative to CT. Renal artery Doppler is a non-invasive and cost-effective diagnostic tool that aids in diagnosis. In the past, radioisotope scans were commonly used, but they have since been replaced by newer techniques. A hypercoagulability and embolic workup is recommended, including an echocardiogram and continuous cardiac monitoring. Treatment should be tailored to the root cause of the infarction. In cases of embolic etiology or hypercoagulable states, lifelong anticoagulation is necessary. For patients with identified renal artery stenosis, revascularization techniques, such as stent placement, are described as therapeutic interventions. In cases of identifiable local thrombosis, interventional thrombectomy techniques can be employed. Repeat renal imaging is recommended 6-12 months after the initial infarct to monitor the evolution of local infarcts and identify any recurrence of new areas of infarction. In this case, because the affected area was relatively small, the patient was not a candidate for any revascularization therapies.
Conclusion
This case underscores the importance of a multifactorial approach when assessing renal infarcts, considering hypercoagulable disorders, blood loss, medication-induced thrombosis, and the postpartum period. Postpartum renal infarcts have been documented in the literature as a consequence of blood loss rather than direct thrombosis or embolic sources. This reinforces the need to ensure hemodynamic stability intraoperatively and during delivery to minimize the risk of end-organ damage.
When treating renal infarction prompt identification is crucial for intervention, particularly if a large area of kidney territory is affected. However, if the infarct is related to blood loss rather than local thrombosis, the likelihood of the area being amenable to embolization is very low.
Postpartum hemorrhage can lead to unusual presentations that may mimic hypercoagulable disorders and pregnancy is recognized as a hypercoagulable state; however, the presence of thrombosis in the postpartum period necessitates further investigation. Additionally, chorioamnionitis is a well-known cause of postpartum hemorrhage, highlighting how one complication can lead to further complications.
Conflict of Interest Disclosure
The author has no conflicts of interest to declare. I certify that the submission is original work and is not under review at any other publication.
- Bourgault M, Grimbert P, Verret C, Pourrat J, Herody M, et al. (2013) Acute renal infarction: a case series. Clin J Am Soc Nephrol. 8: 392-8.
- Kole Monica, Keerthy Madhurima (2019) Postpartum Hemorrhage Leading to Renal Infarction, 55.
- Mouhsine A, Belkouch A, Atmane el M, Rokhssi R, Berrada Y, et al. (2014) Renal vein thrombosis in the post-partum period: a case report. J Med Case Rep. 8: 462.
- Jai Prakash, Pragya Pant, Anil K. Singh, Shashidhar Sriniwas, Vijay P. Singh, Usha Singh (2015) Renal cortical necrosis is a disappearing entity in obstetric acute kidney injury in developing countries: our three decades of experience from India, Renal Failure, 37: 1185-9.
FIGURE 1
Figures at a glance