Effect of Uterine Pressure on Premature Birth of Premature Birth by Recording EHG Signals and Tocogram
Received Date: September 30, 2024 Accepted Date: October 30, 2024 Published Date: November 02, 2024
doi: 10.17303/jwhg.2024.11.204
Citation: Zahra Abdolali Kazemi (2024) Effect of Uterine Pressure on Premature Birth of Premature Birth by Recording EHG Signals and Tocogram.J Womens Health Gyn 11: 1-13
Abstract
Background and Goals: : Premature birth, also called preterm birth, is defined by the World Health Organization as the birth of a live baby that occurs before the 37th week of pregnancy. In addition to premature birth, which medically means premature rupture of membranes. The normal frequency of uterine contractions is once every 2 to 3 minutes. However, with contractions less than this amount, a change in service may be seen. In most cases, 5 to 7 contractions over a period of 15 minutes indicate effective uterine activity.
Materials and Methods: One of these promising methods is electrohistrogram and tocogram. In this project, the technique of processing electro-histogram and tocogram signals with the help of wavelet transform and linear and nonlinear signal properties has been used to predict preterm delivery. The data used in this project were manually recorded using an Edan cardiograph (model F9). Also, the physiotherapy and tocogram databases were used. The above data set consists of 31 recordings of four 30-minute signals of uterine activity, including three EHG signals and a tocogram signal that simultaneously records measurements of uterine mechanical activity (Toko signal). 13 signals out of 31 signals are related to pregnant women with premature delivery, another 13 records are registered for pregnant women with premature birth and signals are registered from non-pregnant women.
Results: The extracted features were classified using a three-core linear support machine classifier, radial basis functions and polynomial polynomials, which resulted in 99.97% accuracy in the training phase and 91.67% in the test phase.
Conclusions: The results show that the proposed method is well able to distinguish between normal delivery and preterm delivery. The results from data obtained mostly from healthy fetuses suggest that with improved quality, more of the diagnostic signals received by the monitor may be obtained correctly for high-risk fetal conditions.
Keywords: Electrohistrogram; Tocogram; Preterm Delivery; Wavelet Transform; Linear and Nonlinear Characteristics; Support Vector Machine Classification
Introduction
Premature births are one of the most important concerns of couples, especially young mothers who are expecting their children. According to studies, the percentage of babies born prematurely is more than born naturally. Blood flow status and fetal heart rate are important clinical indicators in the diagnosis of many fetal defects [1].
Many researchers and scientists are researching new diagnostic methods for assessing fetal and maternal status over long-term phenomena. Analysis of the condition of the mother and fetus by monitoring over long periods of time, or even better, continuous monitoring is a powerful tool in detecting problems and dangerous cases during pregnancy [2].
The normal frequency of uterine contractions during labor is every 2 to 3 minutes, although with contractions less than this amount, changes may be seen in the cervix. In most cases, 5 to 7 contractions over a period of 15 minutes indicate effective uterine activity [3]. An increase in the frequency of contractions above this value is not known as uterine tachysystole and indicates 6 or more contractions over a period of 10 minutes, which is repeated in two subsequent periods. Uterine tachycystole can occur in cases of placental abruption or excessive stimulation of the uterus by oxytocin or the use of intracervical prostaglandins to soften it [4]. Predicting premature birth based on these factors alone is not definitive. Other techniques are needed to better predict. One of these promising methods is electrohistrogram and tocogram.
Evidence suggests that various pathological processes may play a role in initiating preterm labor, such as uterine ischemia, congestive blood vessel contraction, intrauterine infection or inflammation, excessive uterine stimulation, and many other risk factors, including diabetes, obstruction, hypertension, uterine abnormalities, smoking, alcohol and drug use, and lifestyle have also been reported [5]. Predicting premature birth based on these factors alone is not definitive. Other techniques are needed to better predict. One of these promising methods is the analysis of an electromyogram of a uterus recorded from a pregnant woman's abdominal wall, an electrohistrogram.
Theoretical Foundations and Research BackgroundPremature birth can have devastating effects on the baby's brain and body, as well as causing infection and infection in the baby. Premature babies are smaller and can hardly keep warm at this time. This combination affects the body with a lack of body fat and a high ratio of skin to body weight [4]. The baby will stay warm in the neonatal intensive care unit until he or she can regulate his or her body temperature on his or her own (where a tube helps him breathe) is connected [4]. Most premature babies do not have a surfactant even at 35 weeks, a substance in the lungs that keeps small air sacs open [5]. They are replaced with similar substances to prevent distress respiratory syndrome, which is very common in children born before 30 weeks and is less common at this age [5]. Mirroring when breathing or when the baby is breathing intermittently is another premature problem that most often affects babies born before 34 weeks [5]. Some procedures may involve vascular duct arthroscopy, which is open between the blood vessels and the heart [5]. The disease can be cured alone or with medication, a catheter-based procedure, or surgery. Cerebral hemorrhage is more likely to occur in premature infants (born before 28 weeks) and to varying degrees [6]. Some hemorrhages are mild and heal on their own, while others can lead to serious brain damage. All babies born before the 30th week or weighing less than 1,500 grams will be screened for a condition called premature retinopathy. Blood vessels in the eye can be detached from the retina and if left untreated can cause blindness [7].
arthroscopy, which is open between the blood vessels and the heart [5]. The disease can be cured alone or with medication, a catheter-based procedure, or surgery. Cerebral hemorrhage is more likely to occur in premature infants (born before 28 weeks) and to varying degrees [6]. Some hemorrhages are mild and heal on their own, while others can lead to serious brain damage. All babies born before the 30th week or weighing less than 1,500 grams will be screened for a condition called premature retinopathy. Blood vessels in the eye can be detached from the retina and if left untreated can cause blindness [7].
Research BackgroundReducing maternal and infant mortality is one of the strategic goals and policies of every country. By using fetal examination methods during pregnancy, especially in late pregnancy and during childbirth, intrauterine death and hypoxic brain damage can be prevented by correctly and timely diagnosis of unreliable and risky patterns of fetal condition and performing the necessary interventions and measures [13]. The techniques currently used to predict fetal health focus on fetal biophysical findings, including heart rate, movement, respiration, and amniotic fluid production. These findings are used to perform prenatal fetal surveillance to prevent fetal death and to avoid unnecessary interventions [13,12]. In most cases, a negative result, ie a normal test result, is largely reliable, as fetal death rarely occurs within a week of obtaining a normal test result [14]. In fact, in most tests, the negative predictive value (true negative test) is 99.8% or more. In contrast, the estimated value of positive prediction (true positive test) for abnormal test results is low and in the range of 10-40% [15]. In 2015, Niroumanesh et al., by examining the non-contraction test method (increase in fetal heart rate following movements), found that all fetuses developed a destructive pattern in the examination process with a repetitive pattern of prenatal heart rate. In contrast, only one case (in a retarded fetus) was disrupted during delivery, in which case the advantages of this method were ease of use and interpretation and low cost and the minimum time required to perform the test were expressed against the disadvantages of a high positive rate. False and negative values were expressed in comparison with other methods [16].
Uterine contractions naturally resolve within 40 to 60 seconds. Prolonged contractions may be the result of pairing contractions of the uterus, or complications such as placental abruption or rupture of the uterus. The basal pressure of the uterus is normally in the interval between contractions of about 10 mm Hg. In abnormal cases, the basal pressure reaches 20 mm Hg, which changes due to excessive stimulation or rarely due to excessive dilation of the uterus, which occurs in cases of fluid injection into the uterus or fetal enlargement. During contractions, intrauterine pressure increases to 30 to 80 mm Hg, although during the second stage of labor it can be even higher [16,17]. Calderoparsia developed a convenient way to measure uterine activity by calculating pressure (from peak pressure to baseline pressure) over a period of 10 minutes. The sum of these contractile pressures was introduced as the unit of Montevideo [18]. Colby et al. found that the late onset of fetal heart failure during spontaneous uterine contractions was associated with increased fetal mortality, growth retardation, and neonatal complications. Similar observations have been reported by other researchers to induce uterine contractions using oxytocin or nipple stimulation [19,20]. Freeman et al. performed a contraction-induced stress test (using oxytocin-induced spontaneous contraction stress to determine inadequate uterine blood flow in the event of late-onset heart failure) on 4,600 pregnant women, with approximately false-negative results. They reported 0.4 per 1000 when the last prenatal test has a negative and reactive result, the mortality rate around delivery is 3 and 2 per 1000, while in positive and inactive cases it is 176.5 per 1000. False positive cases reported for CST are between 8 and 57% of cases which is an average of 30%. The main benefit of this test is its very high sensitivity and the need to do it once a week. An increase in fetal heart rate following its movements forms the basis of a non-contraction test. Most of these tests are repeated once or twice a week [22,21].
The second goal was to treat BV, first with dequalinium chloride vaginal tablets and directly after continued treatment with clindamycin cream for 7 days, and study if the molecular test can be used as “test of cure”.
The first report on electronic fetal monitoring was published in 1970. Two physicians, Powell and Home, at New Haven Hospital in Yala, USA, monitored 6% of the 4,561 deliveries performed at that hospital during antenatal care, concluding that: Electronic monitoring is helpful in complication deliveries. In the early days, electronic fetal heart rate monitors were more commonly used in complications of pregnancy; but gradually it was also used in most pregnancies. In 1978, it was estimated that approximately two-thirds of American women underwent electronic monitoring during childbirth. In 1993, 78.78% of American women were monitored during childbirth. In the maternity wards of hospitals and medical centers, it is almost inevitable and essential for the management of a delivery process for the relevant staff. Therefore, technical systems for monitoring fetal electrocardiograms during labor have been developed as a next step in continuous monitoring of fetal heart rate to improve fetal monitoring results and minimize unnecessary interference with delivery. The relatively small benefits of using vaginal delivery should be considered against the disadvantages of using an internal skin electrode to record the electrocardiogram waveform after rupture of the membrane [23]. Evidence suggests that reducing the PR compressor distance in fetal electrocardiogram wave data improves the results. There was a clear difference in the number of infants who needed neonatal intubation or the number of infants who needed to be admitted to the intensive care unit. Monitoring through the analysis of PR compressor distances had every advantage [24]. In 2018, a randomized clinical trial was conducted by Hoffman et al. using indirect monitoring of fetal heart rate and uterine contractions, in which measurements of fetal skin acidity and fetal heart rate were compared. Women in whom fetal heart was monitored electronically (fetal monitoring) experienced less labor pain [25]. In addition, evidence suggests that various pathological processes may play a role in the onset of preterm labor, such as uterine ischemia, congestive blood vessel contraction, intrauterine infection or inflammation, uterine hyperstimulation, and many other risk factors. Diabetes, obstruction, hypertension, uterine abnormalities, smoking, alcohol and lifestyle drugs have also been identified [26]. Predicting premature birth based on these factors alone is not definitive [27]. Other techniques are needed to better predict. One of these promising methods is the electro-analytical analysis of the uterus recorded from the abdominal wall of a pregnant woman, EHG, which allows a slightly non-invasive evaluation of mechanical uterine contractions during pregnancy. This is due to the spontaneous explosion of the uterine muscle action potentials due to spontaneous electrical discharge [28,29].
Research Method
Database
The data used in this project are Physiothe database and Term-Preterm EHG DataSet with Tocogram [26]. The above data set (TPEHGT DS) consists of 31 recordings of four 30-minute signals of uterine activity, including three EHG signals and a tocogram signal that simultaneously records measurements of uterine mechanical activity (Toko signal). 13 signals out of 31 signals are related to pregnant women with premature delivery, another 13 registrations are registered for pregnant women with premature delivery and signals are registered from non-pregnant women [26].
Pregnant women have a history of pregnancies leading to preterm delivery (13 records before delivery) and pregnancies leading to normal delivery (13 records) [26]. The main purpose of the data set is to provide a set of marginal contraction intervals (marginal intervals related to uterine contractions) and another set of non-marginal contraction intervals (artificial distances, ie distances outside uterine contractions) [26]. Marginal shrinkage records and artificial distances allow:
Investigate the characteristics of uterine history, contraction intervals and miscarriages during pregnancy [26].
Algorithms have been developed that are used to classify between preterm, preterm delivery, and even the diagnosis of infertility [26].
This dataset was compiled by the School of Computer Science and Information (Laboratory of Medical and Imaging Computer Systems), University of Ljubljana at the University of Ljubljana Medical Center, Department of Obstetrics and Gynecology. Obtaining uterine records and research has been approved by the National Medical Ethics Committee of the Republic of Slovenia (No. 2/1/97 and No. 108/09/09). Recording protocol (including electrode position) which was also used when collecting TPEHG DB database records [26].
The women in this study show a sample of the general population. TPEHGT DS contains 31 uterine files that:
- 13 records are premature with spontaneous delivery; the average delivery time was 33.7 weeks (1.97%) weeks and contains 47 contraction compressions and 47 artificial contractions [26].
- 13 records of timely delivery with an average delivery time of 38.1 weeks (1.04 ±) weeks and contains 53 contractile compression and 53 artificial compression [26].
- 5 records are related to non-pregnant women and include 53 artificial compressions [26].
Pregnant women’s records were obtained during regular pregnancy examinations around the 31st week of pregnancy [26]. The mean recording time and standard deviation of pregnant women's records was 30.2 (76 2.76) weeks of gestation. For manual annotation, graphical user interface and annotation editor have been used [26]. In addition to the main signal visualization and annotation editing, the graphical user interface allows the calculation and visualization of spectra and spectroscopy of signals. Regarding the intervals of annotations, an agreement has been reached between the two annotations [26].
EHG signals were collected from the surface of the abdomen. The electrodes were placed in two horizontal rows, symmetrically above and below the navel, at a distance of 7 cm to measure EHG signals from the records:
The first electrode (1E) was placed 3.5 cm to the left and 3.5 cm above the umbilicus.
The second electrode (2E) was placed 3.5 cm to the right and 3.5 cm above the umbilicus.
The third electrode (3E) was placed 3.5 cm to the right and 3.5 cm below the umbilicus.
The third electrode (3E) was placed 3.5 cm to the right and 3.5 cm below the umbilicus.
The reference electrode was attached to the thigh.
The difference in the electrical potentials of the electrodes leads to the production of three EHG signals:
S1 = E2 - E1 (EHG first signal);
S2 = E2 - E3 (EHG second signal);
S3 = E4 - E3 (EHG third signal) (1)
Prior to sampling, EHG signals were filtered using a Butterworth analog three-pole filter with a bandwidth of 0 to 0.5 Hz [26]. The fourth simultaneous signal is the analog signal related to the external tocogram (toku signal), which is responsible for measuring the mechanical pressure of the uterus [26]. This signal was recorded using an Adan cardiograph (Model F9). The analog toko signal was transmitted to one of the analog-to-digital converter amplifiers (150 μV corresponds to a pressure of 1 kPa) [26]. The sampling frequency for EHG and Toko signals is 20 samples per second or 20 Hz, with a resolution of 16 bits [26].
The main EHG and Toko signals were further filtered from most records using the Butterworth digital filter pass quadrupole filter with cut-off frequency at 0.08 to 5.0 Hz in two directions. TPEHGT DS records contain both main and filtered signals [26].
How to do the workThis method uses an ultrasound transducer that is placed directly on the mother's abdomen. Ultrasound waves originating from the transducer penetrate into the tissues and are returned by the tissue surfaces. In this way, the reflected waves from the moving parts of the fetal heart are converted into converters and converted into electrical signals, which, in a similar way to direct monitoring, are finally recorded in a diagram that shows the fetal heart rate. Indirect evaluation of uterine activity is also performed by a pressure transducer (tocodynamometer) located on the mother's abdomen above the cervix. Uterine contractions put pressure on the wall of the mother's abdomen, which in turn is transferred to the tocodynamometer. Pressure changes are converted into electrical signals that are recorded on the uterine activity tape.
The fetal heart monitor is a paper strip consisting of two cartesian charts. The fetal heart rate is plotted on the graph above, showing time on the x-axis and fetal heart rate on the y-axis. The range of this pulse varies from 30 to 240 per minute. Uterine activity is plotted on the bottom graph so that time is plotted on the x-axis and intrauterine pressure is plotted on the y-axis (in the range of 0 to 100 mm Hg). Fetal heart rate and uterine activity are plotted separately on heat-sensitive paper. Thin vertical lines represent 10-second intervals and thick lines represent 1-minute intervals. In the United States, the standard speed of paper movements is 3 centimeters per minute.
Flowchart DescriptionFigure 1 shows the signal processing diagram of the proposed method for predicting preterm birth.
Block 1: Here all signals include (contraction or dummy intervals, uterine activity recording, all selected (or available) signals, signals (tocogram and EHG) are recorded as R signals using a band line the passage is pre-processed.
Block 2: The nature of the R signal is not considered as frequency time and frequency time range or as artificial contraction intervals.
Block 3: After recording the signal, we used a linear throughpass filter with cut-off frequencies of 0.08 and 5 Hz (to remove artifacts and disturbance signals and frequencies above 5 Hz) for R0-3 processing.
Block 4: With a source of linear phase filters, the bandwidth with cut-off frequencies is related to the frequency bands B0, B1, B3 and B2 and produces subgroups R0-3.
Note: Toko signals are processed in the same way as EHG signals at all stages. Four four-pass digital inheritance filters to shift phase zero and accurately separate four frequency bands applied bi-directionally in each signal from R (main recorded signal).
Block 5: Butterworth filters have a uniform and uniform frequency response and are uncompressed in the band and cut-off band. In each period, the frequency response of the filters ends at -80 dB and after using them in both directions ends at -160 dB. The entropy of the SE sample for each signal is then obtained from a specified range of contractions or from the principal signal recorded for each R0-3 signal, which is the same frequency bands (B0, B1, B3, and B2).
Block 6: Heming window filter is used to design a filter with limited impact response. This filter is suitable for preserving the original information while eliminating noise. For the Fourier series, it follows that the rectangular window produces the best approximation of the mean square to a frequency response for a given value of M. The filter has several obvious properties: 1- The output at any moment depends on the amount of input at the same moment and the previous moments, and the previous values of the output have no role in determining the output at a particular moment. 2- There is no feedback in the structure of these systems. 3- The impact response width of these systems is limited. 4- There is no polarity in the impact response of these filters and all are zero.
Here the power spectrum is calculated using the Fourier transform.
Block 7: Power spectra are smoothed and normalized using a moving average at a frequency interval of 0.1 Hz. The median frequency of the MF and the peak (amplitude) of the PA amplitude for each signal are extracted from a specified interval or from the main recorded signal for each of the frequency bands (B0, B1, B3, and B2).
Block 8: The characteristics obtained from the recorded primary signal and the characteristics obtained from the response of the filters used lead to the classification of the duration and conditions of premature birth of infants and the risks of preterm delivery.
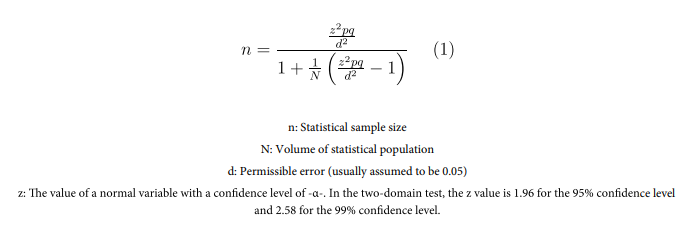
Calculating the sample size is very important in statistical inference and findings. Researchers can draw conclusions about the characteristics of society through examples.
One of the most widely used methods for calculating the sample size is the Cochran's formula. The main formula for calculating the Cochran sample size is as follows:
Results
The extracted properties were classified using SVM classifier with three linear cores, RBF and polynomials. Two RBF cores and polynomials make the SVM classifier nonlinear. Each classification is taught 10 times and the data of each training are randomly selected. This makes it possible to better represent the performance of the classifier by calculating the mean and standard deviation of the 10 stages of training. Tables 1 to 3 present the classification results with linear, RBF, and polynomial cores, respectively. Figures 2 to 5 also show the perturbation matrices for linear, RBF, and polynomial nuclei, respectively. In the RBF core classification mode, the accuracy was 99.97 in the training phase and 91.67 in the test phase. The clutter matrix displays the results of the classification based on actual available information. Accuracy parameter is the most common, basic and simplest criterion for measuring the quality of a category and is the degree of correct recognition of the category in total. Sensitivity and characteristic parameters were also calculated by converting three classes to correct diagnosis class and incorrect diagnosis class. The sensitivity was 99.97 for the training phase and 97.32 for the test phase. Based on these values, different criteria for evaluating classification and measuring accuracy can be defined. The characteristic was also calculated to be 99.84 for the training phase and 95.4 for the test phase. Therefore, RBF gives a better answer than the linear mode. The original diameter values of the matrices are integers and other values are integers.
Conclusion
In this project, only 3 criteria of accuracy, sensitivity and specificity have been used to present the results. Sensitivity and characteristic parameters were also calculated by converting three classes to correct diagnosis class and incorrect diagnosis class. The sensitivity was 99.97 for the training phase and 97.32 for the test phase. The characteristic was also calculated to be 99.84 for the training phase and 95.4 for the test phase. The results show that the proposed method is well able to distinguish between normal delivery and preterm delivery. The results from the data obtained mostly from healthy fetuses suggest that as the quality improves, more diagnostic signals received from the monitor may be obtained correctly for high-risk fetal situations.
Premature birth is a global issue for pregnant women and infants, often leading to death or lifelong health problems. In addition, there is no permanent solution or treatment for preterm labor, as the cause is usually unknown. In addition, although preterm labor is more effective in developing countries, it is also present in developed countries with very high costs of treatment. For these reasons, this project uses two methods to detect preterm labor with the help of EHG and tocogram signals. The aim of this project is to identify the pattern of delivery and send a warning to the pregnant woman by monitoring the EHG contractions of the uterus. Also, the results of the proposal are compared with the existing studies in the literature and the results of previous proposals. One of the main aspects of the proposed system is the use of uterine EHG signals. Of the six proposed studies, only the proposed system and the study (Jacob et al., 2010) used EHG signals. In addition, the proposed system is uniquely designed to use valuable time to monitor and analyze uterine EHG signals without the need for obstetricians. None of the proposed studies were designed to monitor and analyze uterine EHG signals without the need for a gynecologist. According to study by Mark Deleuze et al. (2018), the fetus was well defined. The aim of this study was to provide additional evidence on the true clinical value of the analysis as well as its clinical signs in which fetal blood sampling was required in addition to systemic analysis. There were limitations, and placing the electrode on the face or fetal arteries of the fetus could be dangerous, and the entrapment of the cord could lead to severe pressure on the cord and disruption of maternal blood flow to the fetus. In addition to the lack of existing problems, this proposal made it possible to evaluate uterine contraction activity, which was the only purpose of the previous study.
- Johannes W Bergmans, Massimo Mischi, S Guid Oei, Rodica Strungaru (2005) Improved method for heart rate monitoring. Conf Proc IEEE Eng Med Biol Soc. 5916-9.
- Begum S (2018) Role of non stress test on admission (admission test) at term and its fetal outcome. Int J Sci Res. 7: 63-5
- F Kovacs, Cs Horvath, M Torokv (2006) Long term phonocardiographic fetal home monitoring for telemedicine system. IEEE Engineering in Medicine and Biology 27th Annual Conference. 0-7803
- Iams JD (2003) Prediction and early detection of preterm labor. Am Col Obstet Gynecol. 101: 402-12
- Marque C, Duchene JM, Leclercq S, Panczer GS, Chaumont J (1986) Uterine EHG processing for obstetrical monitoring. IEEE Trans Biomed Eng. 333: 1182-7
- Rabotti C, Mischi M (2015) Propagation of electrical activity in uterine muscle during pregnancy: A review. Acta Physiol. 213: 406-16
- de Lau H, Rabotti C, Oosterbaan HP, Mischi M, Oei GS (2014) Study protocol: PoPE-Prediction of preterm delivery by electrohysterography. BMC Pregnancy and Childbirth. 14: 192.
- Horoba K, Wrobel J, Jezewski J, Kupka T, Roj D, Jezewski M (2016) Automated detection of uterine contractions in tocography signals—Comparison of algorithms. Biocybernetics and Biomedical Engineering. 36: 610-8.
- Lučovnik M, Maner WL, Chambliss LR, Blumrick R, Balducci J, Novak-Antolič Ž, et al. (2011) Noninvasive uterine electromyography for prediction of pretermdelivery. Am J Obstet Gynecol. 204: 1-10.
- Jezewski J, Horoba K, Matonia A, Wrobel J (2005) Quantitative analysis of contraction patterns in electrical activity signal of pregnant uterus as an alternative to mechanical approach. Physiol Meas. 26: 753-67.
- Vlemminx MW, de Lau H, Vullings R, (2015) Peters CH.Electrohysterography. A promising alternative for monitoring contractions. 159: 35-85
- Idowu IO, Fergus P, Hussain A, Dobbins C, Khalaf M, Casana Eslava RV, et al. (2015) Artificial Intelligence for Detecting Preterm Uterine Activity in Gynecology and Obstetric Care. In: Proceedings IEEE International Conference on Computer and Information Technology; 215-20.
- Hussain AJ, Fergus P, Al-Askar H, Al-Jumeily D, Jager F (2015) Dynamic neural network architecture inspired by the immune algorithm to predict preterm deliveries in pregnant women. Neurocomputing. 151: 963-74
- Chen L, Hao Y (2017) Feature Extraction and Classification of EHG between Pregnancy and Labour Group Using Hilbert-Huang Transform and Extreme Learning Machine. Computational and Mathematical Methods in Medicine. 9: 10-1
- Terrien J, Marque C, Gondry J, Steingrimsdottir T, Karlsson B (2010) Uterine electromyogram database and processing function interface: An open standard analysis platform for electrohysterogram signals. Computers in Biology and Medicine. 40: 223-30
- Richman JS, Moorman JR (2000) Physiological timeseries analysis using approximate entropy and sample entropy. American Journal of Physiology Heart and Circulatory Physiology. 278: 2039-49
- Moslem B, Khalil M, Marque C, Diab MO (2010) Energy Distribution Analysis of Uterine Electromyography Signals. Journal of Medical and Biological Engineering. 30: 361-6.
- Ivanov PC, Mark R, Stanley HE, Physio Bank, Physio Toolkit and Physio Net M. Faezipour, TM Tiwari A Saeed, M Nourani, and LS Tamil (2000) Wavelet-based denoising and beat detection of ECG signal. IEEE/NIH Life Science Systems and Applications. 101: 215-20
- EM Stein, G Weiss (1971) Introduction to Fourier Analysis on Euclidean Spaces. Princeton University Press. 691-807
- Garcia-Casado J, Ye-Lin Y, Prats-Boluda G, Mas-- Cabo J, Alberola-Rubio J, Perales A (2018) Electrohysterography in the diagnosis of preterm birth: a review. 39: 1361-6579
- T Hastie, R Tibshirani, J Friedman (2009) “The Elements of Statistical Learning” Bayesian Forecast. Dyn. Model. 1-694
- Provost F, Fawcett T (2013) Data Science for Business: What you need to know about data mining and data-analytic thinking. "O'Reilly Media٬ Inc. 33: 11-5
- Piryonesi S. Madeh; El-Diraby Tamer E (2020) "Role of Data Analytics in Infrastructure Asset Management: Overcoming Data Size and Quality Problems". Journal of Transportation Engineering٬ Part B: Pavements. 146: 1-6
- Cortes Corinna, Vapnik Vladimir N (1995) "Support- -vector networks" (PDF). Machine Learning. 2: 273-97.
- Ben-Hur Asa, Horn David, Siegelmann Hava, Vapnik Vladimir N (2001) "Support vector clustering.Journal of Machine Learning Research". 2: 125-37.
- Hanke YO, Halchenko PB Sederberg, SJ Hanson, JV Haxby, S Pollmann (2009) PyMVPA: A Python toolbox for multivariate pattern analysis of fMRI data. Neuroinformatics, 7: 37-3
- Aizerman Mark A, Braverman Emmanuel M, Rozonoer Lev I (1964) "Theoretical foundations of the potential function method in pattern recognition learning". Automation and Remote Control. 25: 821-37.
- Jin Chi, Wang Liwei (2015) Dimensionality dependent PAC-Bayes margin bound. Advances in Neural Information Processing Systems. Archived from the original on 4-02.
- Schaul J Bayer, D Wierstra, Y Sun, M Felder, F Sehnke, T Ruckstie, J Schmidhuber PyBrain (2010) The Journal of Machine Learning Research. 11: 743-6
FIGURE 1
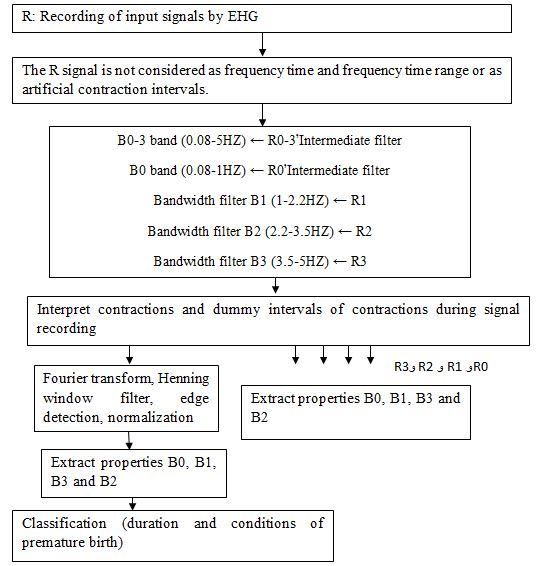
FIGURE 2
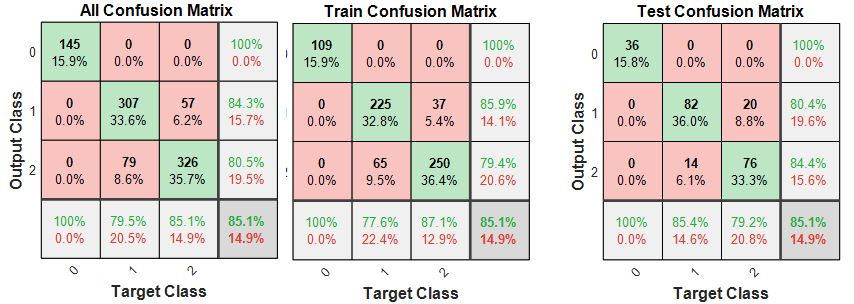
Figure 2: Fusion matrix with linear core
FIGURE 3
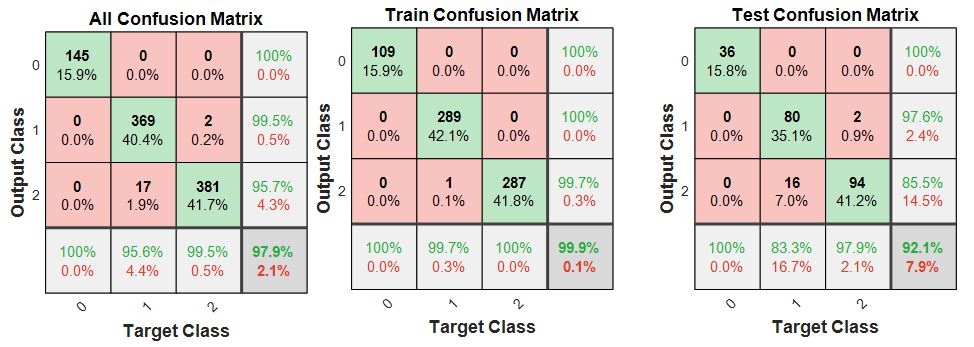
Figure 3: Decomposition matrix with RBF core
FIGURE 4
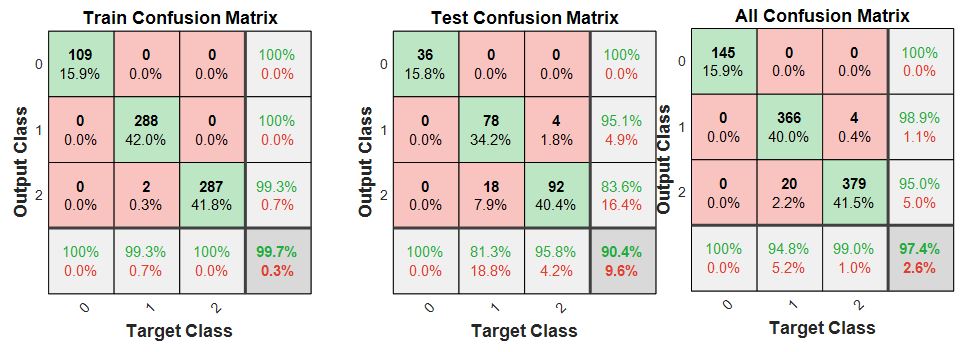
Figure 4: Decomposition matrix with polynomial nucleus
Tables at a glance
Figures at a glance