Endometrial Cancer in Young Women: About a Case
Received Date: December 31, 2024 Accepted Date: January 31, 2025 Published Date: February 03, 2025
doi:10.17303/jwhg.2025.12.103
Citation: M. Lahmar, S. Bicha, N. Dehimi, M. Zaarour (2025) Endometrial Cancer in Young Women: About a Case. J Womens Health Gyn 12: 1-8
Abstract
Endometrial cancer is a disease of menopausal or perimenopausal women. Endometrial cancer in women in their twenties is a rare situation. The rarity of this cancer in this age group, in addition to the difficulty of access to care during a pandemic such as the Coronavirus, can be the cause of delayed diagnosis.
We report a case of endometrial cancer in a young woman to raise the problem of diagnosis that it raises.
Keywords: Endometrial Cancer; Young Age; Inter-Adnexal Hysterectomy; Menopausal or Perimenopausal
Introduction
In 2020, globally, 417,367 new cases of endometrial cancer were diagnosed, 97,370 deaths were caused by endometrial cancer, making this cancer the most prevalent gynecologic cancer [1]. The average age of diagnosis is 68 years of age with 5 to 30% of women diagnosed under 50 years of age.
In the wilaya of Constantine, between 2013 and 2019, endometrial cancer affected 101 women, including 2 under 30 years old, with age extremes at 28 and 90 years old, and a median age of 62 years old, all types of cancer combined.Advanced age (75% of endometrial cancers occur after menopause) is the main risk factor for the classic histological form (type 1) in addition to overweight, obesity, nulliparity, anovulation, diabetes, early puberty, late menopause and oestrogenic impregnation not compensated by progesterone.
The diagnosis of endometrial cancer in a 23-year-old woman is a rare situation. The low incidence of this cancer in this age group can lead to a delay in diagnosis, hence the delay in the management of a cancer known to have a good prognosis in the event of early diagnosis. The relative survival at 5 years is 84% for all stages and histological types combined [2]. In addition to the rarity of endometrial cancer in women in their twenties, the Coronavirus pandemic has made access to care more difficult: confinement, fear of catching the disease in the hospital.
Case Description
This article focuses on a case of a 23-year-old patient who had her menarche at the age of 13, unmarried, nulliparous, BMI at 28.8, with no personal or family pathological history, having never taken contraceptives, without a family history of cancer, who consulted at the gynecological emergency room for metrorrhagia with repercussions on the general condition.
The history of the disease dates back to 2 years earlier marked by menometrorrhagia, with a history of multiple transfusions (a previous hemoglobin level of 4 g/dl) and a long history of taking progestogens without any notable effects. The patient was admitted for the purpose of hemodynamic stabilization with exploration of the symptoms, the ultrasound of the pubic area found a voluminous cervical mass of 3*4 cm.
Under hysteroscopy, the mass was extirpated with exploration of the uterine cavity, which presented a very suspicious appearance: an irregular and hypervascularized mass that extends from the cervix to the uterine cavity. The histological study of the mass carried out by two different pathologists was in favour of a well-differentiated infiltrating endometrial adenocarcinoma of the cervix. Pelvic MRI found a corporeofundal polypoid formation with invasion of less than 50% of the myometrium without locoregional extension, no lymphadenopathy or signs of peritoneal carcinomatosis; at the ovarian level, multiple follicular micro nodules.
The gynecologic oncology decision was to perform an enlarged lymphadenectomy colpohysterectomy (CHEL) with ovarian transposition and adjutant radiotherapy. Macroscopically, at the opening of the uterine lumen, the presence of a pinkish-white tumor proliferation protruding from the cervix was noticed, anatomical pathology revealed a grade 1 endometrioid carcinoma of the uterine body with invasion of less than 50% of the myometrium, the cervix parameters were unharmed. An actual image of the surgical specimen and another taken under an electron microscope are attached.
Discussion
The main conclusion to be drawn from this work is that endometrial cancer is, in general, of good prognosis with a survival rate after 5 years of 84% explained by the early diagnosis and the predominance of the hormone-sensitive histological type: endometrioid adenocarcinoma, but any cancer exposes to the risk of death so it is necessary to know how to evoke this disease regardless of age. In the case of metrorrhagia, it is necessary to triage ultrasound patients requiring additional hysteroscopy and histological analysis, especially since ultrasound is an easy and reproducible examination. A (preventable) delay in diagnosis can be caused by a mispractice that consists of ruling out the diagnosis of endometrial cancer as the causes of bleeding in young women, the case of our patient with bleeding that has been progressing for 2 years treated with dydrogesterone without in-depth investigation.
The Coronavirus pandemic has been partially blamed for the delay in the diagnosis and treatment of several diseases, including cancer. The diagnosis of endometrial cancer is based on the study of ultrasound aspects with the indication of histological analysis in case of suspicious appearance according to IETA (The International Endometrium Tumor Analysis group): (1) poorly defined myometrium-endometrial interface, (2) heterogeneous echogenicity of the endometrium, (3) thickness of the endometrium, (4) Doppler score greater than 2 and (5) irregularity of the endometrial line. (1+2 are the two most reliable ultrasound variables) [3].
Etiological Hypotheses Specific to our Study
Lynch syndrome with a pathogenic constitutional variant: Lynch syndrome is the most common of the syndromes of hereditary predisposition to cancer, of autosomal dominant inheritance [4] occurring at an early age, its prevalence in the general population is 1/1000 to 1/250 [5]. It is the consequence of a constitutional genetic variation on a gene that is part of the DNA repair system MisMatch Repair (MMR): MLH1, MSH2, MSH6 or PMS2; or the EpCAM gene (promoter of the MSH2 gene). Approximately 3% of all endometrial carcinomas and 10% of those with histomoléculaire unstable microsatellites (MSI) are due to constitutional mutation of one of the MMR (mismatch repair) genes MLH1, PMS2, MSH2 and MSH6.
It has been proven that the test for MSI/MMRd is of great importance for 4 reasons: (1) diagnostic: it is considered a marker of endometrioid adenocarcinoma of the endometrium, (2) screening of patients at high risk of presenting Lynch syndrome, (3) prognosis: according to the TCGA (The Cancer Genome Atlas) model, (4) prediction of the usefulness of immunotherapy [6].
The ISGyP (the International Society of Gynecological Pathology) has recommended testing for MMR/MSI status regardless of the age of the patient, the tumor subtype is the tumor subtype [7]. The National Cancer Institute (INCa) recommends the systematic performance of a tumor test to look for failure of the MMR system in the event of: diagnosis of colorectal cancer before the age of 60, endometrial cancer before the age of 50 and/or an evocative personal and/or family history [8]. Patients likely to be carriers of Lynch syndrome (index case) must be referred to an oncogenetic consultation with a view to carrying out a constitutional genetic analysis, which is the only way to confirm the syndrome in the event of a mutation in an MMR gene. Pre-symptomatic tests: genetic tests targeted at the identified mutation are then offered in the family [9]. The age of onset of cancer in Lynch syndrome depends on the gene mutated, the type of mutation and the age of onset of cancer in family members. Monitoring should begin at the age of 35 (personal factors must be taken into consideration), this is a very early age compared to the average age of endometrial cancer, as well as the age of our patient. Endometrial monitoring is done by an annual transvaginal ultrasound and an annual or biannual biopsy. A total hysterectomy with bilateral annexectomy should be considered after completion of the parental project, preferably before the age of 40 in order to prevent the risk of endometrial and ovarian cancer, the risk of finding occult cancer during prophylactic surgery is not negligible (17%) and must be informed to the patient. Hormone replacement should be initiated if the woman is not menopausal. At the age of 70, the incidence of endometrial cancer is 34%, 51%, 49%, and 24% for the MLH1, MSH2, MSH6, and PMS2 genes respectively [10]. The MMR status of our patient has not been studied due to the impracticality of immunohistochemical tests of the new histomolecular classification at the Constantine University Hospital, these tests are not available.
Other Hereditary Cancer Syndromes
Although our patient does not have the clinical criteria for Cowden syndrome, we thought it useful to cite them as an example of hereditary cancer syndrome. That syndrome, also known as multiple hamartoma syndrome, is rare, of autosomal dominant inheritance associated with mutation constitutionnelle PTEN. Patients with this syndrome are at risk of developing breast, thyroid, endometrial or colon cancer. A case of grade 1 endometrioid adenocarcinoma in a 14-year-old girl was cited in 2012 in "THE JOURNAL OF Obstetrics and Gynecology Research", the patient then presented with fibrocystic dystrophy of the breasts and colonic polyps. She was diagnosed with Cowden syndrome at the age of 20. It is recommended to look for Cowden syndrome in the presence of endometrial cancer in adolescence [11].
Polycystic Ovary Syndrome (PCOS)
According to a study carried out between 1989 and 2003 on 188 women diagnosed with endometrial cancer before the age of 50 in order to identify new risk factors for endometrial cancer in young women by studying their clinical characteristics by dividing them into three groups according to their BMI (normal weight, Overweight and obesity): A large proportion of obese and overweight women had diabetes and irregular menstrual cycles. Among women of normal weight, a large proportion were nulliparous, had a history of infertility, or had synchronous ovarian cancer.
These Results Are Part of a Well-Known Hormonal Profile
Polycystic ovary syndrome [12], which is the most common hormonal disease in women of childbearing age. A causal link between endometrial cancer and polycystic ovary syndrome was clearly established in an article in CMAJ (the Canadian Medical Association Journal) published in 2021 citing oligomenorrhea and polycystic ovary syndrome among the risk factors for endometrial cancer [13]. Chronic anovulation is related to chronic hyperestrogenism giving estrogenic stimulation of the endometrium not compensated by progesterone, This appears to be the basis of the causal link between polycystic ovary syndrome and endometrial cancer. Obesity, metabolic syndrome, hyperinsulinism and hyperandrogenism seem to be implicated in hyperestrogenism. Our patient had polycystic ovaries on the MRI report. The patient does not remember the characteristics of her menstrual cycle before the onset of metrorrhagia, she had a BMI of 28.8. Our patient probably had undiagnosed and untreated polycystic ovary syndrome. A study carried out between 2007 and 2013 in a Chinese hospital in 9 young women (between 24 and 38 years old) histologically diagnosed with endometrial cancer with polycystic ovary syndrome concluded that none of these patients took regular treatment for polycystic ovary syndrome or had undergone the necessary follow-up. In this article, it is mentioned that the rate of atypical endometrial hyperplasia in the case of syndrome polycystic ovaries without regular treatment is 35.7%, while the prevalence of endometrial cancer in women with this syndrome is 37%. It has been cited that the endometrium of patients with polycystic ovary syndrome has excessive estrogen and androgen receptors. This study highlights the risk of endometrial cancer in the presence of polycystic ovary syndrome, and therefore requires consideration of this fatal association in providing the necessary treatment and monitoring for this category of women. This will make it possible to diagnose and treat endometrial cancer in this young population at an early stage [14].
Endometrial Cancer without Conventional Risk Factors
According to a study published in a journal of gynecologic oncology, more than a third of young women's cases with endometrial cancer were not linked to the classic risk factors. This retrospective study divided a group of 327 women between the ages of 15 and 49 years at the time of endometrial cancer diagnosis into three groups: (1) women with hyperestrogenism, (2) women with suspected Lynch syndrome, and (3) women with no classic risk factors for endometrial cancer. There was no difference between these three groups in terms of age, pregnancy, tumour grade, choice of treatment and response to hormonal treatment.
Comparison with Other Cases of Endometrial Cancer in a Young Woman
We will take the case of a 30-year-old Italian woman diagnosed with well-differentiated endometrial cancer and conservative treatment was initiated, became pregnant after 3 months of treatment and underwent a caesarean section at the 36th week with multiple negative biopsies. 8 months after giving birth, Exploratory laparotomy revealed metastatic poorly differentiated adenocarcinoma. Despite chemotherapy, the patient died of acute respiratory syndrome due to massive neoplastic pulmonary lymphangitis [15]. This young woman received conservative treatment, unlike our case study, which underwent radical treatment. Certainly, the patient put on conservative treatment was able to conceive, but unfortunately the evolution of the cancer was not controlled at the end, unlike the case of our study which underwent radical treatment and adjuvant radiotherapy. Our patient lives in a region relatively far from the University Hospital, in addition to the sanitary conditions of this period (COVID 19) which could have made monitoring difficult and demanding in the event of conservative treatment. In addition, if we take published studies about conservative treatment outcomes and treatment recommendations, to assess a maximum time between diagnosis/start of conservative treatment and hysterectomy (in the absence of relapse or recurrence), a very important notion because of the common history of infertility in This population, there is a great deal of heterogeneity. Hysterectomy after childbirth is indisputable given the risk of relapse, but there is no exact time limit to be respected in the absence of conception or after childbirth. The average duration of follow-up under conservative treatment is 3 years for the studies used: (1) a study carried out in Japan on 28 women under 40 years of age, diagnosed with stage 1A endometrial cancer and 17 women with atypical endometrial hyperplasia [16], (2) a study carried out in Spain on 133 patients under 45 years of age [17], and (3) a study of 14 Italian women with an average age of 38 years [18]. Our patient is not married and does not seem to have precise landmarks concerning her first conception, unlike the case treated in Italy where the woman became pregnant after three months of treatment, which justifies our conduct.
The effectiveness of conservative treatment is currently being evaluated. The very encouraging results of the published studies in this regard cannot be generalized due to the limited number of cases and the differences in epidemiological characteristics.
Strengths and Limitations of the Article
Limitations
The set of statistics targeted by our study lacks generalization criteria: the limited number of women, heterogeneous epidemiological criteria. The impracticality of immunohistochemical tests of the new histomolecular classification at the Constantine University Hospital.
Strengths
This is a rare scientific publication on endometrial cancer in a woman in her twenties belonging to the Maghreb country and even elsewhere in the world.
Conclusion
All cancer exposes you to the risk of death, so you have to know how to talk about this disease regardless of age. Never rule out endometrial cancer from the etiological hypotheses of metrorrhagia, even in young women. The standard treatment for endometrial cancer is colpo-hysterectomy with bilateral annexectomy without resection of the roof of the vagina supplemented by external beam radiation therapy. Any conservative attitude must be carefully evaluated, this requires: (1) the selection of a target population for conservative treatment, (2) the establishment of a good doctor-patient relationship, (3) the consent of the person concerned by explaining the various advantages and risks of this approach, which is not a standard treatment, and the obligation of the ultimate use of radical treatment, (4) the maintenance of the necessary rigorous monitoring: clinical, ultrasound and histological. Polycystic ovary syndrome is the most common hormonal disease in women of childbearing age, known as a risk factor for endometrial cancer, hence the interest in treatment with regular follow-up in the presence of this syndrome. In the case of endometrial cancer in a young woman, a hereditary predisposition to cancer (Lynch) should be mentioned.
- Hsiu-Jung Tung, HJ HH (2022) Adjuvant and post-surgical treatment in endometrial cancer. ELSEVIER, 52-63.
- Ngo CG (2018) Classification des carcinomes de l'endomètre. Edimark.fr, 134-7.
- M Madkour N (2017) An ultrasound risk-scoring model for prediction of endometrial cancer in post-menopausal women (using IETA terminology). ScienceDirect, pp. 201-5.
- Elise Coffin, MD (2019). Identification and management of patients with Lynch syndrome. PubMed.gov, 904-14.
- Xi Li, GL (2021) Recent advances in Lynch syndrome. Springer Link, 1-8.
- Nicole Concin, X MG (2020) ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. International Journal Of Gynecologicalo cancer, 12-39.
- Ibid.
- Elise Coffin, MD (2019) Identification and management of patients with Lynch syndrome. PubMed.gov, pp. 904-14.
- Ibid.
- Nicole Concin, XM G (2020) ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. International Journal of Gynecologicalo cancer, 12-39.
- William David Baker AP (2012) Endometrial cancer in a 14-year-old girl with Cowden syndrome: A case report. Journal of Obstetrics and Gynaecology Research, 876-8.
- Kathleen M Schmeler, PT (2005) Endometrial cancer in young, normal-weight women. ELSEVIER, 388-92.
- Mara Sobel AN (2021) Endometrial cancer. CMAJ, 193-5.
- Xibiao Jia LY (2020) Endometrial cancer combined with polycystic ovary syndrome in 9 women under 40 years old: A case report.
- G Ferrandina, GV (2005) Progression of conservatively treated endometrial carcinoma after full term pregnancy: A case report. Elsevier, 215-7.
- Kimio Ushijima HY (2007) Multicenter Phase II Study of Fertility-Sparing Treatment With Medroxyprogesterone Acetate for Endometrial Carcinoma and Atypical Hyperplasia in Young Women. Journal of Clinical Oncology, 2798-803.
- Luis Chiva FL CM (2008) Sparing fertility in young patients with endometrial cancer. Gynecologic Oncology, S101-4.
- Giuseppe Laurelli GD (2011) Conservative treatment of early endometrial cancer: Preliminary results of a pilot study. Gynecologic Oncology, 43-6.
FIGURE 1
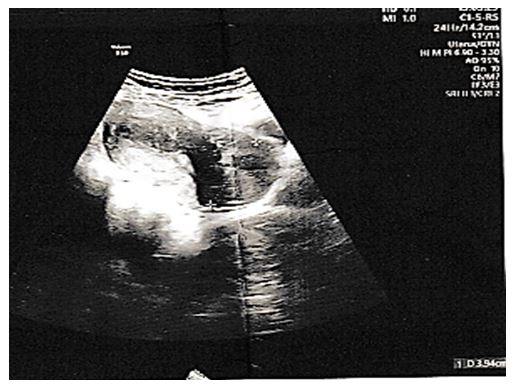
Figure 1: Ultrasound image objectifying the cervical mass
FIGURE 2
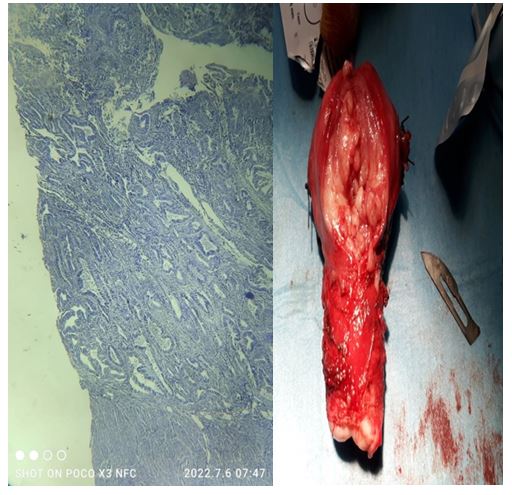
Figure 2: Left: an authentic photo of the operating room. Right: an electron microscope photo of the operating room
Figures at a glance