A Tubal Stump Ectopic Pregnancy: A Case Report
Received Date: February 21, 2025 Accepted Date: March 21, 2025 Published Date: March 24, 2025
doi:10.17303/jwhg.2025.12.105
Citation: Chloe Tytherleigh, Mr Karan Sampat (2025) A Tubal Stump Ectopic Pregnancy: A Case Report. J Womens Health Gyn 12: 1-8
Abstract
A 27-year-old female presented to the Early Pregnancy Unit (EPU) for a reassurance scan following a positive pregnancy test. The transvaginal ultrasound (TVUS) confirmed an ectopic pregnancy. She was consented for a diagnostic laparoscopy and removal of the ectopic pregnancy. Intra-operatively, a right tubal stump ectopic was visualised and removed. She was discharged home one day post the operation with advice to repeat urine human chorionic gonadotrophin level (hCG) three weeks’ time and to attend EPU for future pregnancies for reassurances scans and monitoring.
Keywords: Family planning, Pregnancy Loss, Ectopic pregnancy, Tubal stump
Background
This case highlighted the rarity of a tubal stump ectopic pregnancy. Panelli [1] reports that ectopic pregnancies occur in 1-2 % of all pregnancies, with the most common site being the fallopian tube. Ectopic pregnancy ruptures are the leading cause of maternal mortality within the first trimester, they contribute to 5-10 % of all pregnancy-related deaths [2]. The subtypes of ectopic pregnancies include tubal, interstitial, caesarean scar, heterotopic, cervical, ovarian and abdominal [3]. Loh and colleagues [4] noted that tubal stump ectopic pregnancies have an estimated incidence of 1.16 % of all ectopic pregnancies. Risk factors associated with ectopic pregnancies include previous ectopic pregnancies [5], smoking [6], aged above 35 years old and pelvic inflammatory disease [7]. Also, the ectopic pregnancy rate amongst in-vitro ferilisation (IVF) pregnancies is 2.1-8.6 % after embryo transfer which is higher than the incidence in natural conceptions which is 2% [8]. With this information in mind, we need to be aware that patients that have had previous salpingectomies may be at risk of tubal stump ectopic pregnancies and that when they present to the EPU or the Accident and Emergency (A&E) department, it is important for us to rule out whether the ectopic has ruptured.
Case Presentation
The patient contacted the EPU mid-August following experiencing abdominal pain and her last menstrual period (LMP) being mid-July alongside having a positive hCG test. The patient attended the EPU for a reassurance scan, at the time of presentation, the patient was gravida 4 para 0. The patient did not present with any abdominal pain, signs of haemodynamic instability or per vaginal bleeding. Further, she had no pelvic pain, no vomiting, no diarrhoea, or no episodes of dizziness or syncope.
Past medical history included a previous right sided ectopic pregnancy four months prior (surgically managed- right salpingectomy), a previous termination and a previous miscarriage, alongside reactive situational depression and anxiety. Information regarding her previous ectopic pregnancy was gathered from medical notes from the hospital system, however these were incomplete and therefore may not explain why certain decisions were made.
The patient presented four months prior to this case report’s presentation, following a positive pregnancy test at approximately six-weeks’ gestational age (GA). She was scanned at the EPU which revealed a right ectopic pregnancy and subsequently underwent a right salpingectomy. The operation notes did not detail why a tubal stump was left. The histology report was as follows: macroscopic- dilated fallopian tube 52 mm and up to 22mm in diameter, slicing revealing no obvious foetal parts of vesicles; microscopic examination- tube lumen distended by blood clot and chorionic villi, no trophoblast abnormality was seen; conclusion- right fallopian tube pregnancy. She was reviewed one month post operation and had not had a menstrual period yet. She was reviewed further one month later and was advised to contact the EPU once she had a positive pregnancy test in addition to being informed about the likelihood of another ectopic pregnancy as women with prior ectopic pregnancies have up to ten times risk compared to the general population [9]. It was not clear as per the patient’s notes what contraceptive advice was given following her first ectopic pregnancy.
Given the patient’s previous ectopic pregnancy and the fact that it was surgically managed, highlighted the importance of being aware of such rare cases and to be mindful of the management of these patients.
Investigations
The medical notes from the system noted documentation of scans and several hCG levels. She had hCG every 2 days (Table 1) and was advised regarding red flag signs at every contact. The serial serum hCG levels showed a trend upwards starting at 327 mIU/mL to 9204 mIU/mL. The TVUS reports can also be seen in Table 1, the patient had several scans between the day of initial presentation and the date of the final scan.
The TVUS (Figure 1) revealed a right sided ectopic pregnancy.
Differential Diagnosis
The fact that the patient was pregnant did narrow our differentials down quite significantly. Once the TVUS was performed, it was clear that the pregnancy was ectopic and due to the patient’s previous ectopic pregnancy she was at increased risk of having another. Other risk factors that predispose an individual to ectopic pregnancies include previous ectopic, tubal or pelvic surgery, pelvic inflammatory disease, sexually transmitted infections, sub-fertility, intrauterine copper device and the Mirena coil as well as the progesterone only pill. However, due to her presentation being routine she did not have signs of haemodynamic instability such as hypotension or tachycardia that may have pointed the diagnosis in the direction of a ruptured ectopic.
Treatment
Given the TVUS findings, the decision was made to take the patient to theatre for a diagnostic laparoscopy; intraoperatively a right sided tubal stump ectopic was removed (Figure 2). On day 11-post operation, she experienced PV bleeding that was deemed menstruation and had blood tests taken on day 17-post operation, which showed no abnormalities. A repeat hCG was not performed.
Outcome and Follow-Up
Shortly after the operation, the patient was sent a letter detailing the surgery formally and was advised to contact the EPU during future pregnancies at six-weeks post operation. The patient contacted the EPU day 8-post operation as she was concerned about the operation sites as she was reporting some oozing alongside some intermittent PV bleeding and cramping pain. She was provided with reassurance and safety netting advice was given. She had a telephone call on day 11-post operation with the consultant whereby she reported an episode of PV bleeding that was deemed to be menstruation. On day 17-post operation she presented to the EPU with abdominal pain around operation site wounds with some yellowish discharge from the wounds alongside headaches. She did not have any fevers, nausea or vomiting and she was passing urine alongside opening her bowels normally. Blood tests and observations were performed alongside an examination and no abnormal findings were found. She was sent home with safety netting advice. The histology report from the ectopic pregnancy is as follows: macroscopic- tan haemorrhagic tissue in aggregate 31 x 18 x 7 mm, no obvious foetal parts or vesicle identified; microscopic examination- sections show chronic villi and trophoblast, fragments of fallopian tubes are seen showing focal chronic inflammation with trophoblasts, there is also haemorrhage present, no atypical features are seen; conclusion- right fallopian tubal stump ectopic pregnancy.
Discussion
The atetiology of tubal ectopic pregnancies suggest that it involves abnormal embryo transport and alteration in the tubal environment which enables abnormal implantation to occur [10]. Factors that could contribute to this include increased ciliary motility driven by estradiol (E2), progesterone (P) [11] and nitrous oxide (NO) [12] which may cause aberrant tubal transport.
As previously mentioned, the risk factors associated with tubal stump ectopic pregnancies are the same risk factors that have been associated with ectopic pregnancies generally. Zuzarte and Khong [13] explored why an ipsilateral ectopic gestation occurred after a partial salpingectomy. They hypothesized that lumina persist in the interstitial portion and distal remnant of the left fallopian tube allows communication between the endometrial and peritoneal cavities and therefore the migration of spermatozoa or the fertilised egg from the endometrial cavity to the distal remnant of the left fallopian tube [13]. Furthermore, they hypothesized that in their described case, the spermatozoa passed through the intact right fallopian tube and pouch of Douglas to the distal remnant of the left fallopian tube [13].
Gaughran et al [14] reviewed the rationale for leaving a short versus a long stump at salpingectomy and concluded, albeit based on no formal evidence, the recurrence rate of ectopic pregnancies is independent of tubal stump length. Furthermore, a long stump is preferable to a short stump as the bleeding risk with rupture is lower and the surgery less technically challenging [15].
Samiei-Sarir and Diehm proposed potential management suggestions to help mitigate the risk of tubal stump ectopic implantation. These suggestions included adequate diathermy of the proximal portion of ligation with clips alongside performing hysterosalpingography to evaluate patency of the fallopian tube [16].
In terms of how the investigations informed our clinical management, the hCG levels increased from 327 mIU/mL to 9024 mIU/mL over the course of nine days. Given the timeline of the patient’s presentation, with her LMP being 1 month prior, the likely gestation of the pregnancy was deemed to be approximately 4-5 weeks. In a normal intrauterine pregnancy, the hCG level will typically increase by approximately 50 % every 48 hours, however if the rate of increase is slower than expected it may suggest early pregnancy loss or ectopic pregnancy [17]. In our case, on the 22/8, the hCG levels were 2083 mIU/mL and at this level we would expect to see clear signs of an intrauterine pregnancy. Considering that there was no clear intrauterine pregnancy seen at the time of the TVUS, it warranted concern. Although the hCG levels were useful to understand if the rate of increase was proportional to gestation, the hCG levels alone did not provide compelling evidence for an ectopic pregnancy therefore TVUS was required.
When reviewing the literature for further instances of tubal stump ectopic pregnancies, some case reports were found highlighting similarities in case presentation. Homagain and colleagues [18] detailed a case of a 29-year-old female with a history of amenorrhoea and severe lower abdominal pain, dizziness and generalised weakness. She had a history of a previous ruptured ectopic pregnancy and underwent a left salpingectomy 18 months prior. Transabdominal scan revealed a thick-walled cystic structure in the left adnexa. She underwent an exploratory laparotomy, which revealed a left tubal stump containing material resembling potential product of conception. Histopathology revealed chorionic villi like material suggestive of ectopic pregnancy. Although Homagain and colleagues [18] detailed a different patient presentation; our patient presented with no obvious symptoms and had a routine reassurance scan following a positive pregnancy test. Both cases highlighted the rarity of tubal stump ectopic pregnancies and revealed that patients can present differently ranging from asymptomatic to having severe abdominal pain and weakness.
Deryndaa and colleagues [19] reported a case of three consecutive ectopic pregnancies in a 36-year-old woman following birth of her first child via Caesarean section. She had the first ectopic pregnancy located in the left fallopian tube, which was initially managed using methotrexate and eventually a left salpingectomy was undertaken. Her second ectopic pregnancy, which arose from in-vitro fertilisation, occurred and was located in the right adnexa; methotrexate was given and was successful. Her third ectopic pregnancy was located on the left fallopian tube stump; it occurred 24 days after embryo transfer and resulted in a ruptured ectopic which was managed with an emergency laparoscopy and removal of left fallopian tube remnants. In our patient case, similar to case detailed by Deryndaa and colleagues [19], the patient had a previous right sided ectopic pregnancy four months prior to the presentation that was managed via a right salpingectomy. A few months later, she fell pregnant again and presented to the EPU for a reassurance scan. Upon scanning, an ectopic pregnancy was visualised. During the diagnostic laparoscopy, the ectopic pregnancy was located on the right fallopian tube stump and was subsequently removed.
Conclusion
This case has highlighted the importance of identifying ectopic pregnancies early to prevent further complications in the patient. In addition, this case reflects the rarity of a tubal stump ectopic pregnancy but does highlight that they are not unheard of. Therefore, tubal stump ectopic pregnancies should be within the differential when assessing individuals of childbearing age who present for any assessment in presence of a positive pregnancy test.
- Panelli DM, Phillips CH, Brady PC (2015) Incidence, diagnosis and management of tubal and nontubal ectopic pregnancies: a review. Fertil Res Pract. 1: 15.
- Houser M, Kandalaft N, Khati NJ (2022) Ectopic pregnancy: a resident’s guide to imaging findings and diagnostic pitfalls. Emerg Radiol. 29: 161-72.
- Mullany K, Minneci M, Monjazeb R, C. Coiado O (2023) Overview of ectopic pregnancy diagnosis, management, and innovation. Women’s Health. 19.
- Loh WN, Adno AM, Reid S (2020) VP59.30: Spontaneous tubal stump ectopic pregnancy following ipsilateral salpingectomy. Ultrasound in Obstetrics & Gynecology. 56: 322.
- Jacob L, Kalder M, Kostev K (2017) Risk factors for ectopic pregnancy in Germany: a retrospective study of 100,197 patients. Ger Med Sci. 15: Doc19.
- Saraiya M, Berg CJ, Kendrick JS, Strauss LT, Atrash HK, Ahn YW (1998) Cigarette smoking as a risk factor for ectopic pregnancy. Am J Obstet Gynecol. 178: 493-8.
- American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Gynecology. ACOG Practice Bulletin No. 193: Tubal Ectopic Pregnancy. Obstetrics and gynecology. 131: e91-103.
- Cheng LY, Lin PY, Huang FJ, Kung FT, Chiang HJ, Lin YJ, et al. (2015) Ectopic pregnancy following in vitro fertilization with embryo transfer: A single-center experience during 15 years. Taiwan J Obstet Gynecol. 54: 541-5.
- Mummert T, Gnugnoli DM (2023) Ectopic Pregnancy. StatPearls Publishing.
- Shaw JL V, Dey SK, Critchley HOD, Horne AW (2010) Current knowledge of the aetiology of human tubal ectopic pregnancy. Hum Reprod Update. 16: 432-44.
- Paltieli Y, Eibschitz I, Ziskind G, Ohel G, Silbermann M, Weichselbaum A (2000) High progesterone levels and ciliary dysfunction--a possible cause of ectopic pregnancy. J Assist Reprod Genet. 17: 103-6.
- Jain B, Rubinstein I, Robbins RA, Sisson JH (1995) TNF-alpha and IL-1 beta upregulate nitric oxide-dependent ciliary motility in bovine airway epithelium. Am J Physiol. 268: L911-7.
- Zuzarte R, Khong CC (2005) Recurrent ectopic pregnancy following ipsilateral partial salpingectomy. Singapore Med J. 46: 476-8.
- Gaughran J, Mitchell S, Holland T (2020) Salpingectomy for ectopic pregnancy: Does length really matter? Int J Reprod Contracept Obstet Gynecol. 10: 333.
- Takeda A, Manabe S, Mitsui T, Nakamura H (2006) Spontaneous ectopic pregnancy occurring in the isthmic portion of the remnant tube after ipsilateral adnexectomy: Report of two cases. Journal of Obstetrics and Gynaecology Research. 32: 190-4.
- Samiei-Sarir B, Diehm C (2013) Recurrent ectopic pregnancy in the tubal remnant after salpingectomy. Case Rep Obstet Gynecol. 2013: 753269.
- Barnhart KT, Guo W, Cary MS, Morse CB, Chung K, Takacs P, et al. (2016) Differences in Serum Human Chorionic Gonadotropin Rise in Early Pregnancy by Race and Value at Presentation. Obstetrics and gynecology. 128: 504-11.
- Homagain S, Kharal N, Khanal H, Shahi T, Pandey J, Katuwal N (2022) Ruptured ectopic pregnancy on a tubal stump: A case report. Clin Case Rep. 10.
- Derynda B, Griffith V, Malik R (2022) Tubal Stump Ectopic Pregnancy Following Two Previous Ectopic Pregnancies. J Clin Gynecol Obstet. 11: 47-52.
FIGURE 1
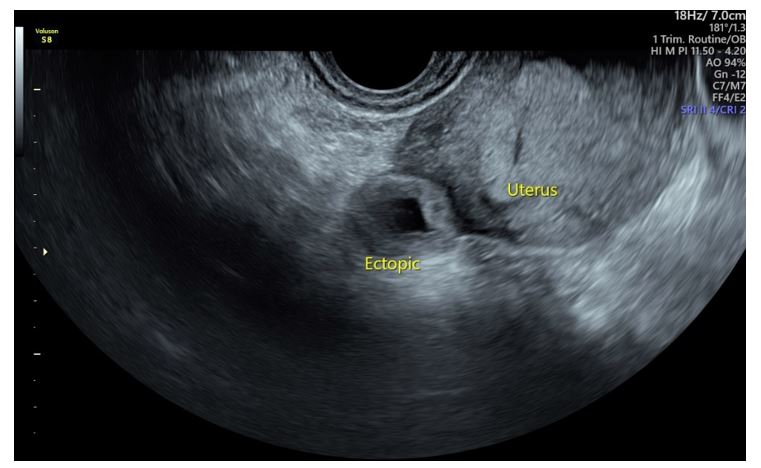
Figure 1: Transvaginal ultrasound, location of the uterus and ectopic pregnancy labelled, dated 26th August
FIGURE 2
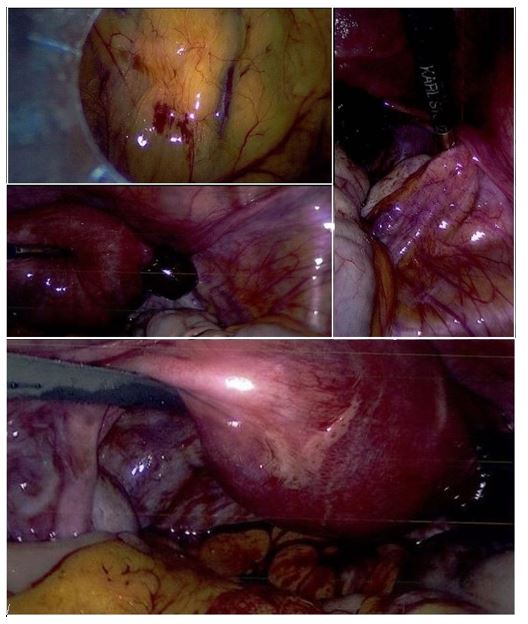
Figure 2: Laparoscopic surgery images. A (top left): entry into peritoneal cavity through port. B (top right) and C (middle): tubal stump ectopic pregnancy D (bottom): uterus with right tubal stump ectopic pregnancy
Tables at a glance
Figures at a glance