Clinical Efficiency of CO2 Laser Therapy for Vulvar Lichen Sclerosus in Dalian, China
Received Date: February 09, 2022 Accepted Date: March 09, 2022 Published Date: March 11, 2022
doi: 10.17303/jwhg.2022.9.107
Citation: Nasra Mohamoud Ali (2022) Clinical Efficiency of CO2 Laser Therapy for Vulvar Lichen Sclerosus in Dalian, China. J Womens Health Gyn 9: 1-10.
Abstract
Background: Lichen sclerosis is an inflammatory autoimmune skin disease that favors the anogenital area. VLS include symptoms pruritus, burning sensation, atrophy, shrinkage, scar formation, stricture in the introitus that make patients uncomfortably self-conscious, but also limits and complicates patients’ social life and sexual intimacy. VLS can be controlled with topical corticosteroids that Mainly offer temporary relief. In recent years, there have been reports that CO2 lasers have been used to treatment gynecological diseases including VLS.
Objective: In this study, we aim to analyze the clinical efficacy of CO2 laser therapy for vulvar lichen sclerosis; relevant factors related to the VLS lesion; and overall effectiveness of laser treatments.
Methods:We recruited 55 patients suffering from VLS at the gynecological outpatient clinics in Dalian Medical University Affiliated Gynecology and Obstetrics Hospital between May 2018 to August 2019. Data was collected through direct interviews and clinical examinations. Diagnosis was confirmed by biopsy.
Results: The age of the 55 patients ranged from 26 ~ 73 years old (average age 50±13.4 years old). All patients completed 3 to 5 laser sessions. 51 (94%) patients and 54 (98.1%) were free of itching and pain at Follow-ups of 6 and 12 months respectively (P<0.001). 42 (76%) paftients had a 60% reduction of vulvar skin lesion area at follow-up of 12 months (P <0.001). 17/55 (31%) patients with fissures and/or cracks experienced complete recovery of the fissures and/or cracks.
Conclusions: CO2 laser treatment is effective for the treatment of VLS and has minimal or no side effects. Dot CO2 laser has potential benefits for patients with VLS and requires our full attention to determine its long-term efficacy and safety.
Keywords: CO2 laser; Vulvar Lichen Sclerosis; efficacy of CO2 laser therapy; Dot laser
Introduction
Unplanned pregnancies
Vulvar Lichen sclerosis (VLS) is an Inflammatory auto-immune dermatological disease, that favors the anogenital area. The estimated prevalence of VLS lies between 0.1% for children [1] and 3% for women over 80 years of age [2]. However, up to 40% of women with LS will display onset of symptoms and cutaneous changes of vulvar LS during their reproductive years [3,4] The etiology and pathogenesis of VLS remain unclear. Current studies believe that etiology of VLS is multifactorial, with autoimmunity being the primary pathogenesis of VLS, while other etiologies include poor hygiene, chronic friction, trauma, chronic irritation, and infection (Borrelia burgdorferi [5] and human papillomavirus) [6]. Vulvar LS is also an important predisposing factor to vulvar squamous cell carcinoma, with an estimated 5% chance of malignant transformation [7]. In the early stages of VLS, slight redness may be seen. As the disease progresses white lesions occur (insufficient pigmentation), that can advance into plaques, superficial vulvar atrophy, follicular plugging, keratin-associated thickening, small bleeding foci under the epithelium, or erosions or fissures, leading to the disappearance of labia majora, scarring, and adhesion of labia minora, completely burying the clitoris. Lacerations are often seen at the labial posterior commissure and perineal area, as well as a narrowing of vaginal introitus resulting in dyspareunia and difficult insertion of speculum. Perianal stenosis and painful defecation typically occur later in the course of the disease [8,9]. The clinical manifestations of VLS may affect patients' social lives, family, interpersonal relationships, sleep, and intimacy, leading to an increased incidence of mental health disorders. VLS is mainly diagnosed by its unique clinical manifestations, but the final definitive diagnosis is a histopathological examination. A biopsy of the most affected area is recommended for accuracy.
Several treatment options for VLS have been introduced in the last decade to achieve remission and prevent disease progression. First-line treatments of VLS have been topical corticosteroids. However, topical corticosteroids require long-term maintenance, which most patients neglect or unable to maintain, long term use can also result in side effects like skin thinning and atrophy. Surgical approaches include vulvectomy and cryosurgery; however, these procedures leave scars on the damaged tissues and are associated with high recurrence rates [9]. Photodynamic [10], ultrasound therapy has been used for VLS treatment as well [11]. Lasers have recently been used to treat VLS, showing good efficacy with no or little discomfort during the treatment, and with no side effects. In a histological study, fractional microablative CO2 laser induced the production of new collagen and elastic fibers, thereby remodeling connective tissues without damaging adjacent tissues [12]. A few numbers of studies have demonstrated the disappearance of symptoms and significant improvement of signs when laser therapy is used for VLS [13-16]. In this study, we analyzed the clinical efficacy of CO2 laser therapy for vulvar lichen sclerosis, relevant factors related to the VLS lesion, and overall effectiveness of laser treatments. Our study not only emphasizes that an Early diagnosis, comprehensive patient counseling, appropriate management and long term follow up of patients suffering from vulvar lichen scleroses are necessary to prevent genital deformation and the development of malignancy. It is against this background that we prospectively summarize and analyze the efficacy and feasibility of CO2 laser in the treatment of VLS.
Materials and Methods
Study Protocol
We present a study of 55 patients suffering from VLS who underwent smartxide2 Dot CO2 laser treatment at Dalian Medical University affiliated Dalian Maternal and Child Health Hospital (Dalian Gynecology and Obstetrics Hospital) between May 2018 to August 2019. This study was approved by the Ethics Committee of the Obstetrics and Gynecology Hospital of Dalian Medical University and informed consent was signed by the patients. The mean age of patients were 50 years old (ranging from 26 to 73yrs old) with 68% (34/55) being postmenopausal.Most of the patients were previously treated with either topical corticosteroids or other topical traditional therapies, but experienced little or no relief, followed by a relapse of the condition. Of the 55 patients, 3 patients had Vulvar Lichen Sclerosus combined with vulvar epithelial hyperplasia (diagnosis were confirmed by biopsy). Inclusion criteria of the participants included: having itching symptoms; pathological diagnosis of VLS; informed consent. Exclusion criteria included: Genital tract infections (genital herpes, vaginitis, cervicitis, pelvic inflammatory disease, etc.); vulvar itching caused by lower urinary tract infection; pathological diagnosis of cervical, vaginal, vulva intraepithelial neoplasia and malignant tumors; vulva squamous cell hyperplasia, or the combination of vulva squamous cell hyperplasia of VLS; vulvar vitiligo; vulvar neuropathy; vulvar hyperpigmentation diseases; use of steroid hormones 3 months before treatment; abnormal uterine bleeding; pregnant women; mental illness; serious surgical and internal diseases (such as uncontrolled control diabetes). All the patients met the inclusion criteria.
Data collection
Data was collected and recorded through direct interviews, normal gynecological examinations and auxiliary examinations (routine examination of vaginal secretions, papanicolaou test, TCT, hepatitis A, hepatitis B, hepatitis C, HIV, syphilis, blood glucose and ECG etc.) were performed to exclude contraindications. Symptoms and signs were evaluated before the first laser treatment, before each laser session, and at follow-up of 3month, 6month and 12month following the last treatment. Symptom and signs were evaluated using a visual analogue scale (VAS: 0 being no signs and symptoms and 10 being the worst). All the patients were symptomatic, all of the patients presented itching (100%), dyspareunia (82%), burning pain, atrophy, thinning of the skin (Figure 1), epithelial pallor, and narrowing of the vaginal orifice (Figure 2). Patients’ lesion sites were mainly on the clitoris or labia minora, labia majora, perineum and perianal area (3 cases 5.4%). All the patients under went biopsies to confirmed diagnosis.
Patient assessment
General clinical data, Sociodemographic characteristics and VLS associated risk factors (thyroid disease, diabetes, history of IUD, oral contraceptive, previous history of laser treatment, family history of VLS, etc.) were recorded through direct interview.
Clinical symptoms including vulvar itching, vulvar burning, vulvar pain and dyspareunia were also recorded. A visual analogue scale (VAS) was used to evaluate the severity of patients' vulva itching, vulva pain and dyspareunia. Scoring was from 0 (none) to 10 (maximum). 0 marks: no itching/pain/dyspareunia; 1 ~ 3 points: mild; 4 ~ 6 points: moderate; 7 ~ 10 points: severe (Table 1).
The lesion ranged from the clitoris to the posterior perianal region and from both sides to the lateral margin of the labia major.
The course of disease was recorded from the time of clinical symptoms and from when the signs started.Complications such as injuries, infections, ulcers, skin atrophy, changes in pigmentation, acne and others were assessed intra and post operation.
Satisfaction judgment: The Likert scale was used to evaluate satisfaction, which was divided into very satisfied, satisfied, uncertain and dissatisfied. The overall satisfaction is satisfied + very satisfied.
Efficacy evaluation time: evaluation was conducted before treatment, 1 month after the first treatment, 1 month after the third treatment, and follow-up of 3, 6, and 12 months after the last treatment.
Treatment method
Pre-operation preparation: The skin of the vulva was disinfected with Iodophor, 5% compound lidocaine cream was utilized for a local infiltration anesthesia, a PVC membrane was used to cover the area for 30 minutes Then the area was wiped and cleaned with a normal saline solution and the vulvar skin was dried with sterile gauze (Figure 3).
Treatment: Patients were treated with the fractional microablative CO2 laser (SmartXide2V2LR;Deka) using the following Treatment parameters: power 20-24W, time 300-400μs, spacing 250-400μs (Figure. 4). Each patient went through 3-5 treatment sessions, with 1month intervals.
Postoperative cautions: (1) vulvar skin must be kept clean and dry; (2) local cold compressions were recommended for 12 hours after treatment; (3) avoid bathing for 24 hours; (4) avoid hot water bathing and vigorous exercise for 3-4 days; (5) avoid sexual intercourse and wear loose cotton underwear for 7 days.
Statistical Analysis
SPSS21.0 software was used for statistical analysis. The counting data are expressed by rate, the measurement data conforming to normal distribution are expressed by mean ± standard deviation (± s), and the variance is by paired sample t test; the measurement data not conforming to normal distribution are expressed by median (upper quartile, lower quartile), and by Wilcoxon signed rank sum test. P< 0.05 was considered statistically significant.
Results
The age range of 55 VLS patients was 26 ~ 73 years old (average age 50±13.4 years old). 33/55 (60%) were postmenopausal. 20 patients (36.4%) had thyroid disease, and one patient (2.5%) had diabetes, 21 patients (38.2%) had a history of oral contraceptives, 32 patients (52.8%) had a history of IUDs, 3 patients (5.4%) had a family history of VLS, 1(2.5%) patient had a history of extragenital lichen sclerosus and had received laser therapy. Patients’ Demographics are shown in Table 2. 90% of the patients had previously tried several kinds of topical treatments and reported little or no relief.
The disease’s duration ranged from 0.5 to 20 years, with mean duration of 7.1±5.6 years. All patients had different degrees of vulva pruritus. (46/55,83.6%) patients had vulva pain, (8/55, 14.5%) were not sexually active due to VLS caused severe dyspareunia and morphological changes, (47/55, 85.4%) patients were sexually active, (37/47,78.7%) of the sexually active patients had dyspareunia (8/40, 20%), 17/55(31%) patients had fissures/cracks Table 3.
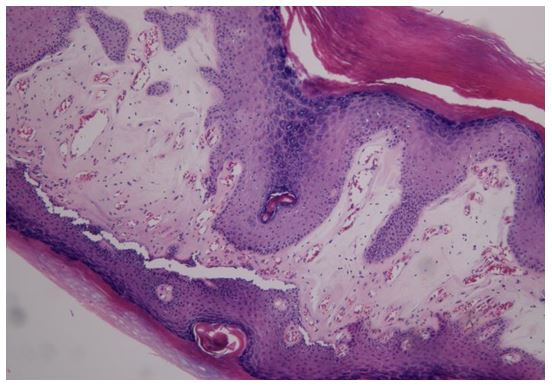
All patients’ diagnosis was confirmed with biopsies; pathological results showed hyperkeratosis on the surface extending to under epithelium, hypopigmentation of some basal layers, hyalinization of the dermis, inflammatory infiltrate of polymorphonuclear band and plasma cells (Figure 5).
All patients completed three to five treatment sessions (depending on the extent and severity of the lesions) with an average of (3.3±0.6) treatment sessions, 41/55 cases completed 3 sessions, 10/55 patients completed 4 sessions, and 4/55 patients completed 5 sessions. All of the patients completed follow-ups of 3 ~ 12 months, with an average of (9.90±3.73) months shown in Table 4. The average duration of the laser procedure was 5 to 13 minutes, no discomfort or serious adverse effects were reported during the procedure. Patients reported burning sensation for about 24hrs following the procedure which was relieved by cold compression, and only one patient experienced swelling which resolved within 24hours. All Patients experienced exfoliation within one week, and re-epithelization occurred within 3weeks.
One month after the 3rd treatment, 20 of the 55 patients were free of itching and pain, and 25 of the patients’ itching and pain was markedly reduced. At the 3 months follow-up 43(78.1%) patients were free of itching, and 46(84%) were free of pain(P<0.001), 51(94%) patients and 54(98.1%) were free of itching and pain respectively at 6 months and 12 months (P<0.001).
At one month after 3rd treatment there was improvement in dyspareunia although it was not statistically significant (P>0.05), 38 of the 45 sexually active patients reported no dyspareunia at the 6 months follow-up, 5/47 reported significant improvement or only experiencing dyspareunia occasionally, and 2/47 patients had no improvement due to irreversible vulvar deformity caused by VLS. There were statistically significant differences in dyspareunia between 1 month after the third treatment and 3, 6, and 12 months of the follow-up (P <0.001).
At one month after the third treatment, 8/47 patients with mild vulvar morphological changes (skin appearance, elasticity and fissures/erosions) showed significant improvement, but 39/47 showed little improvement (p>0.05). At 3 months and 6 months during the follow-up, 36/47 showed significant improvements, and further improvements at the 12 months follow-up (P <0.05).
Skin coloration showed no statistically significant differences at one month after the 3rd treatment (P>0.05). At a 3months follow-up, the vulvar skin color of 29/55 patients showed significant improvement, and, at 6 and 12 month follow-ups, 35/55 of the patients showed further improvement (P <0.001), although there was no significant change in the extent of vulvar skin lesion area at one month after the 3rd treatment (P>0.05). At the 3 months follow-up, 10 (18.1%) patients had a 40% reduction in size of the vulvar skin lesion area; 42 (76%) had a 60% reduction in size of the vulvar skin lesion area at the 6- and 12-months follow-up (P <0.001). 17/55(31%) patients who suffered from fissures and/or cracks had their situation resolved completely (Figure 6). VAS score of clinical symptoms and signs before and after treatment are shown in Table 5. At the 12 months follow-up (52/55) 95% of the patients were very satisfied and (3/55) 5% were satisfied, overall satisfaction rate of the patients was 100%. Recurrences of the disease were not reported.
Discussion
Vulvar Lichen sclerosis is an inflammatory auto-immune dermatological disease, characterized by atrophy, thinning, and whitening of the epithelial of the vulva and perianal skin. It has a negative impact on sexual intimacy and the quality of life of patients and may progress to a malignant disease. Even though clinical judgment is enough to diagnose vulvar lichen sclerosus, biopsy is recommended to confirm the diagnoses and exclude other overlapping or concurrent conditions or progression to malignancy
Minimally ablative fractional laser therapy has gained acceptance as a preferred method for skin restoration, especially in the field of dermatology and gynecology. CO2 laser ablates the improperly functioning dermal-epidermal zone, and creates a subsequent re-epithelisation characterized by the reduction of hyperkeratosis and a new zone that functions properly, thereby allowing for maintenance and the continued remission of LS [17]. In our study patients didn’t experience or report any discomfort during the laser procedure and experienced no side effects. Our patients experienced exfoliation of the ablated area (white spots that the laser scan created), then re-epithelization within 3 weeks. In consistence with our study, a study using human skin in vivo for the first time published that ablative fractional resurfacing demonstrated much more rapid re-epithelialization when compared to its non-fractional predecessors, whether powered by erbium or CO2 lasers. Within 48 hours, most subjects in that study demonstrated complete re-epithelialization with the restoration of the basement membrane apparent no later than 7 days post-treatment. This advantage over non-fractional ablative devices partially explains the apparent reduction in patient down times, such as persistent erythema and infection risk [18]. A cohort of 27 patients with VLS who had 3-4 laser treatments reported cessation of itching and pain/discomfort, as well, 26/27 patients demonstrated visible improvement of skin color, elasticity, and vascularity [13]. In a study of 40 patients with VLS, after appropriate laser sessions, 72.5% of patients reported a significant improvement of symptoms, 96.3% of the patients had visible vulvar skin improvement and a 20% decrease of white epithelium following the laser treatment and described the fractional CO2 laser as being a helpful approach for managing LS that is unresponsive to traditional treatment options [19]. In our study duration of symptoms ranged from 0.5 to 20 years. Most of them had used different traditional topical treatments and reported little or no improvement. After 3 to 5 sessions of laser therapy and at 3 months follow-ups, considerable number of the patients were free of itching (78.1%) pain (84%). Likewise, almost all the patients were free from itching (94.0%) and pain (98.1%) at 6 month and 12 month follow-ups. These findings are congruent with reports from previous studies [15-19]. Moreover, randomised case-control study by Bizjak Ogrinc U at el. reported that the laser-treated group showed significantly better results than the control group within 3 months of treatment, and improvement of symptoms in the laser group was still significant at 6 months [20].
It’s worth mentioning that improved clinical signs were observed in this present study but were not as significant compared with improvement of symptoms, especially severely scarred or deformed vulvar structures. These findings therefore allow us to fairly point out that laser therapy improves patients’ symptoms significantly although doesn’t completely repair already deformed vulvar structure due to VLS.
Notwithstanding those findings in this study are comparing to reports from previous studies, there a few limitations. The limitations of this study include; a small number of patients (55), post-operation biopsies not being done to observe the histological changes due to patients' refusals. Also, patients' physical examinations were obtained and evaluated using direct physical examination and photographs taken before every procedure and at follow-up by the doctors doing the procedure, instead of blind evaluators, thus making our results prone to bias. Our study has its strength of being, to our knowledge the first study to conduct the longest follow-up time for the treatment of VLS with Dot CO2 laser with good treatment efficacy, and no relapse of the VLS for years of follow-up after laser therapy.
Since VLS is such a debilitating, and traumatic condition, it's worth emphasizing that the attention of a multidisciplinary team (dermatologists, gynecologists, urologists, and psychologists) is needed, to carry out larger, more well-controlled studies with long-term follow-up to confirm the number of studies that demonstrate the feasibility of CO2 laser therapy for vulvar lichen sclerosus, as well as efficacious and safety, and to determine the permanence of the laser’s efficacy.
Conclusion
This study highlights that CO2 laser treatment is an effective for the treatment of VLS and has minimal to no side effects. In addition, Dot CO2 laser therapy has potential benefits for patients with vulvar lichen Sclerosis with different levels of pruritus, however can’t repair patients with major vulvar deformity due to VLS. our full attention to determine its long-term efficacy and safety. There is the need for further longitudinal studies on the clinical validity of CO2 laser treatment on VLS among larger cohort.
Authors’ contributions
Nasra M. Ali drafted the original manuscript. Xuelin Qu and Longwei Li assisted in data collection and clinical work. Han Lu revised the manuscript for advanced suggestions. The authors read and approved the final manuscript.
Conflict of Interest Disclosures
All authors declare that they have no conflicts of interest Funding: there was no funding from third party
Acknowledgement
The authors gratefully acknowledge all participants and staffs who have participated in this study and We thank Kyle Landon McKay (a native English speaker, an ESL instructor) for providing assistance in editing this manuscript.
- Powell J, Wojnarowska FJJotAAoD (2001) Childhood vulvar lichen sclerosus: an increasingly common problem. 44:803-806.
- Leibovitz A, Kaplun V, Saposhnicov N, Habot BJAog, (2000) geriatrics. Vulvovaginal examinations in elderly nursing home women residents. 31:1-4.
- Cooper SM, Gao XH, Powell JJ, et al. (2004) Does treatment of vulvar lichen sclerosus influence its prognosis? Arch Dermatol. 140:702–706.
- Schlosser BJ, Mirowski GW (2015) Lichen sclerosus and lichen planus in women and girls. Clin Obstet Gynecol. 58:125–142.
- Eisendle K, Grabner T, Kutzner H, Zelger BJAod (2008) Possible Role of Borreliaburgdorferi Sensu Lato Infection in Lichen Sclerosus.144 :591-8.
- Powell J, Strauss S, Gray J, Wojnarowska F (2003) Genital carriage of human papilloma virus (HPV) DNA in prepubertal girls with and without vulval disease. Pediatric dermatology. 20:191-4.
- Edwards SK, Bates CM, Lewis F, et al. (2014) 2014 UK national guideline on the management of vulval conditions. Int J STD AIDS 26: 611–24.
- Thorstensen KA, Birenbaum DL (2012) Recognition and management of vulvar dermatologic conditions: lichen sclerosus, lichen planus, and lichen simplex chronicus. Journal of midwifery & women’s health. 57:260-75.
- Walkden V., Chia Y., Wojnarowska F (1997) “The association of squamous cell carcinoma of the vulva and lichen sclerosus: implications for management and follow up”. J. Obstet. Gynaecol., 17; 551.
- Declercq A., Güvenç C, De Haes P (2020) Proposition of standardized protocol for photodynamic therapy for vulvar lichen sclerosus. Journal of Dermatological Treatment 1-9.
- Wu C, Zou M, Xiong Y, Wang L, Chen H, et al. (2017) Short‐and long‐term efficacy of focused ultrasound therapy for non‐neoplastic epithelial disorders of the vulva. BJOG: An International Journal of Obstetrics & Gynaecology, 124: 87-92.
- Lubach D, Rath J, Kietzmann M (1995) Skin atrophy induced by initial continuous topical application of clobetasol followed by intermittent application. Dermatology. 190:51-5.
- Hutchinson-Colas J, Segal S (2015) Genitourinary syndrome of menopause and the use of laser therapy. Maturitas.82: 342-5.
- Pagano T, De Rosa P, Vallone R, Schettini F, Arpino G, Giuliano M, et al. (2018) Fractional microablative CO2 laser in breast cancer survivors affected by iatrogenic vulvovaginal atrophy after failure of nonestrogenic local treatments: a retrospective study. Menopause. 25:657-62.
- Balchander D, Nyirjesy P (2020) Fractionated CO2 Laser as Therapy in Recalcitrant Lichen Sclerosus. J Low Genit Tract Dis. 24:225-8.
- Pagano T, Conforti A, Buonfantino C, Schettini F, Vallone R, Gallo A, et al. (2020) Effect of rescue fractional microablative CO2 laser on symptoms and sexual dysfunction in women affected by vulvar lichen sclerosus resistant to long-term use of topic corticosteroid: a prospective longitudinal study. Menopause. 27:418-22.
- Teodoro M, Scibilia G, Lomeo E, Pecorino B, Galia A, Scollo PJC, et al. (2019) Carbon dioxide laser as a new valid treatment of lichen sclerosus. 46:206-10.
- Hantash BM, Bedi VP, Kapadia B, Rahman Z, Jiang K, Tanner H, et al. (2007) In vivo histological evaluation of a novel ablative fractional resurfacing device. Lasers in surgery and medicine. 39:96-107.
- Baggish MSJJoGS (2016) Fractional CO2 laser treatment for vaginal atrophy and vulvar lichen sclerosus. 32: 309-17.
- Bizjak Ogrinc U, Senčar S, Luzar B, Lukanović A (2019) Efficacy of Non-ablative Laser Therapy for Lichen Sclerosus: A Randomized Controlled Trial. J Obstet Gynaecol Can. 41:1717-25.
FIGURE 1

FIGURE 2

FIGURE 3
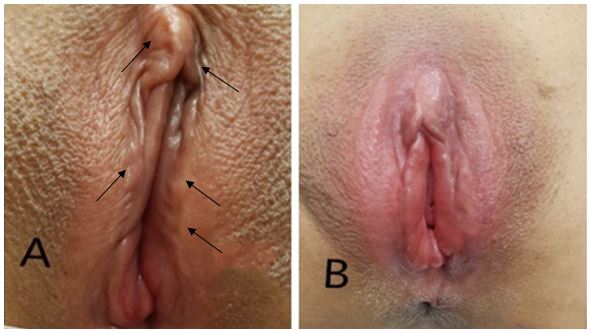
FIGURE 4

FIGURE 5

FIGURE 6
Tables at a glance
Figures at a glance